Impact of the COVID-19 pandemic on routine surveillance for adults with chronic hepatitis B virus (HBV) infection in the UK
Cori Campbell, Tingyan Wang, David A. Smith, Oliver Freeman, Theresa Noble, Kinga A Várnai, Steve Harris, Hizni Salih, Gail Roadknight, Stephanie Little, Ben Glampson, Luca Mercuri, Dimitri Papadimitriou, Christopher R Jones, Vince Taylor, Afzal Chaudhry, Hang Phan

TL;DR
The study found that routine monitoring of chronic hepatitis B patients in the UK dropped significantly during the COVID-19 pandemic.
Contribution
The study quantifies the impact of the pandemic on HBV surveillance using real-world health data from NHS Trusts.
Findings
There was a significant reduction in the proportion of patients with at least one biomarker measurement annually during the pandemic.
The mean number of biomarker measurements per patient also decreased during the pandemic compared to pre-pandemic years.
Abstract
Background:To determine the impact of the COVID-19 pandemic on the population with chronic Hepatitis B virus (HBV) infection under hospital follow-up in the UK, we quantified the coverage and frequency of measurements of biomarkers used for routine surveillance (alanine transferase [ALT] and HBV viral load). Methods: We used anonymized electronic health record data from the National Institute for Health Research (NIHR) Health Informatics Collaborative (HIC) pipeline representing five UK National Health Service (NHS) Trusts. Results: We report significant reductions in surveillance of both biomarkers during the pandemic compared to pre-COVID-19 years, both in terms of the proportion of patients who had ≥1 measurement annually, and the mean number of measurements per patient. Conclusions: These results demonstrate the real-time utility of HIC data in monitoring health-care provision,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
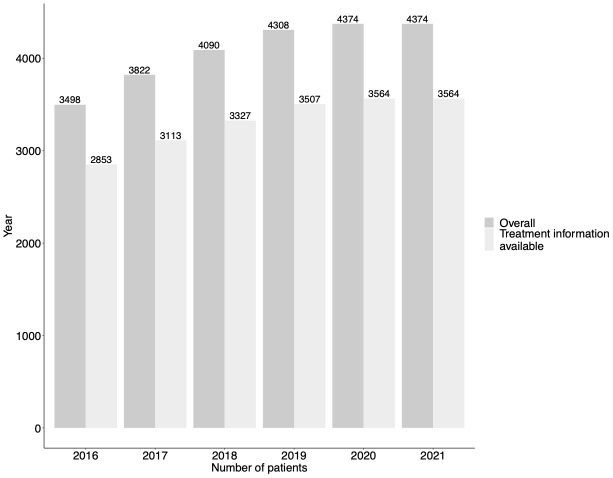 Figure 1
Figure 1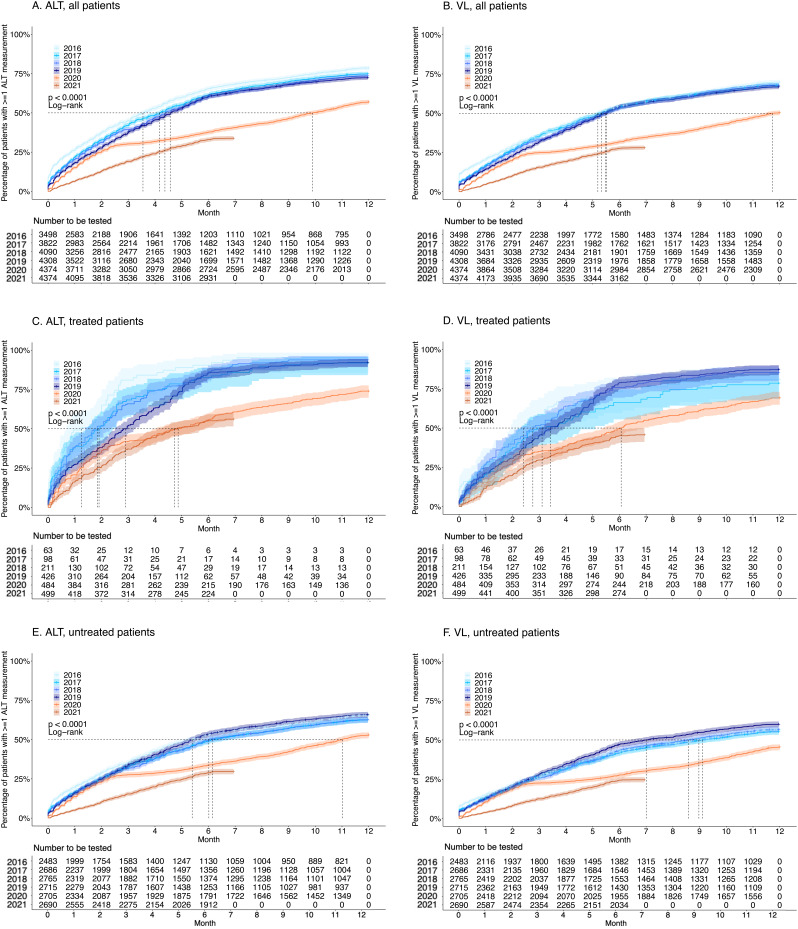 Figure 2
Figure 2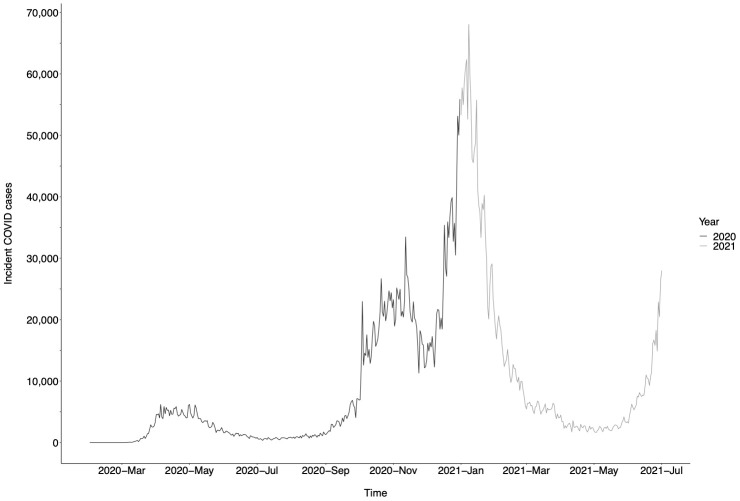 Figure 3
Figure 3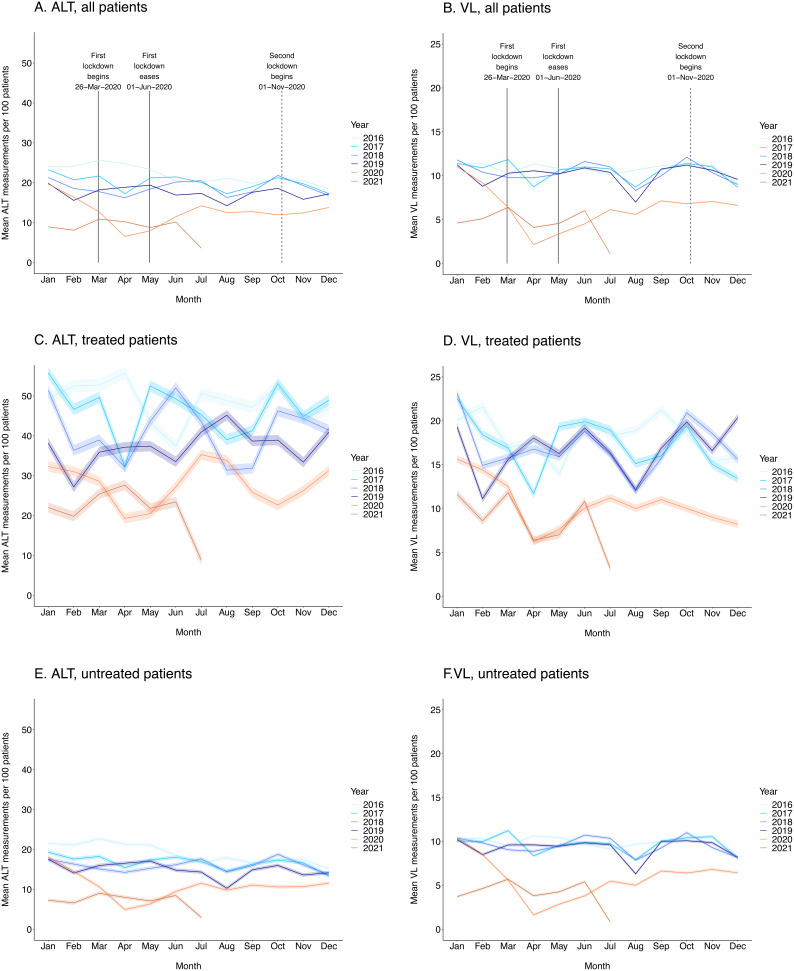 Figure 4
Figure 4| ALT | Alanine transferase |
| CHB | Chronic HBV |
| COVID-19 | Coronavirus Disease 2019 |
| GHSS | Global Health Sector Strategy |
| HBV | Hepatitis B virus |
| HCC | Hepatocellular carcinoma |
| HIC | Health Informatics Collaborative |
| NHS | National Health Service |
| NIHR | National Institute for Health Research |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| VL | Viral load |
| WHO | World Health Organization |
- —Wellcome Trust
- —NIHR Oxford Biomedical Research Centre
- —GlaxoSmithKline
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatitis B Virus Studies · Liver Disease Diagnosis and Treatment · Hepatitis C virus research
Abbreviations
**: **
Introduction
Mortality and morbidity associated with the Coronavirus Disease 2019 (COVID-19) pandemic can be directly attributed to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), but also result from indirect impacts on other conditions.
In order to progress towards elimination targets for Hepatitis B virus (HBV) infection ^ 1 ^ there is an urgent need for improvement of surveillance and treatment coverage. This will necessitate enhanced screening, followed by surveillance of individuals with chronic HBV (CHB) to determine treatment eligibility. Clinical follow-up includes routine monitoring of liver enzymes (e.g., alanine transferase (ALT)), hepatitis B virus (HBV) DNA viral load (VL), elastography, ultrasound, and occasionally liver biopsy ^ 2– 4 ^. In those receiving antiviral treatment, laboratory parameters are monitored to ensure virologic suppression is achieved and maintained, and to identify complications.
Surveillance using VL and liver enzymes is recommended, typically at intervals of 3–12 months, and more frequently among males at older age, those with biochemically active hepatitis, risk factors for hepatocellular carcinoma (HCC), complications of liver disease, recent diagnosis, or changing treatment plans ^ 5, 6 ^. COVID-19-attributable disruptions to HBV elimination efforts have been broadly described ^ 7, 8 ^, but we set out to quantify the specific impact on routine HBV surveillance in secondary care services in England using individual-level patient data.
Methods
We undertook longitudinal and cross-sectional analyses using routinely-collected individual-level secondary care data collected across five NHS Trusts in England by the National Institute for Health Research (NIHR) Health Informatics Collaborative (HIC), as previously described ^ 9, 10 ^. HBV treatment data were available from three NHS Trusts. We investigated how ALT and VL surveillance varied between pre-COVID-19 (years 2016–2019) to COVID-19 (year 2020 and part of 2021), comparing surveillance metrics in patients on and off antiviral therapy.
We calculated cumulative probabilities of undergoing ≥1 ALT and HBV DNA VL measurement each year using the Kaplan-Meier method, comparing probabilities across years using the log-rank test. We quantified the mean number of ALT and HBV DNA measurements per 100 patients, during pre-COVID-19 and COVID-19 years, with 95% CIs calculated using the normal distribution (whereby standard error (SE) is estimated by with n denoting sample size and s denoting standard deviation). Official UK government COVID-19 incidence data are presented ^ 11 ^.
Ethics approval
The research database for the NIHR HIC viral hepatitis theme was approved by South Central - Oxford C Research Ethics Committee (REF Number: 21/SC/0060). All methods in this study were carried out in accordance with relevant guidelines and regulations. The requirement for written informed consent was waived by South Central - Oxford C Research Ethics Committee, because data has been anonymised before its use and the study is retrospective.
Results
Coverage of ALT and VL testing (proportion tested at least once a year)
We analysed data representing 3498 individuals in 2016; this increased to 4374 for 2020 ( Figure 1). In 2016, 78.6% (95% CI 77.1–79.9%) of individuals with CHB had ALT measured on ≥1 occasion throughout the year; this significantly decreased to 57.0% (95% CI 55.5–58.4%) in 2020 ( Figure 2A). Median time to 50% of the cohort achieving ≥1 ALT measurement was <140 days for 2016–19 and 301 days for 2020. Similarly, throughout 2016, 70.0% (95% CI 68.3–71.3%) of patients had VL measured at least once, whilst this significantly decreased to 50.0% (95% CI 48.9–51.8%) in 2020 ( Figure 2B). Median time to 50% of patients having achieved ≥1 VL measurement was 158–167 days for 2016–19 and 357 days for 2020. COVID-19 incidence data are displayed in Figure 3.
Number of HBV patients included in study period sample.Denotes number of patients overall, and those with treatment information available. Our analysis included 3,498 individuals in 2016; this increased to 4,374 for 2020. The proportion of patients with treatment data available remained consistent throughout our study period at 2852/3498 (81.6%) in 2016 and 3,564/4,374 (81.5%) in 2020.
Kaplan-Meier plots demonstrating the cumulative proportion of adults with chronic Hepatitis B virus (HBV) infection undergoing routine laboratory surveillance.Plots show patients who have had ≥1 alanine transferase (ALT) (panels A, C, E) and ≥1 HBV DNA viral load (VL) (panels B, D, F) measurement each year for pre-COVID-19 (2016–19) and COVID-19 (2020 and part of 2021) years. For both ALT and VL, plots are stratified by treated (panels C and D, respectively) and untreated (panels E and F, respectively) patients. Dashed lines depict median time for 50% of the cohort to have the laboratory assessment undertaken. Cumulative probabilities for each year were calculated using the Kaplan-Meier method, comparing probabilities across years using the log-rank test, with 2016 serving as the reference/baseline year.
*UK coronavirus disease 2019 (COVID-19) incidence, displayed as number of incident daily COVID-19 cases
12 .Data from March 2020 to July 2021 are displayed.*
Coverage of ALT and VL testing stratified by treatment status
A subset of 82% of patients had treatment data recorded (which remained consistent during the period observed. In treated patients, the proportion with ≥1 ALT measurement decreased significantly from 95.2% (95% CI 85.6–98.4%) in 2016 to 74.0% (95% CI 69.7–77.6%) in 2020 ( Figure 2C), and in untreated patients from 65.4% (95% CI 63.5–67.3%) to 53.0% (95% CI 51.1–54.8%) in 2020 ( Figure 2E). The proportion of treated patients with VL measured decreased from 81.0% (95% CI 68.3–88.6%) in 2016 to 69.2% (95% CI 64.8–73.1%) in 2020 ( Figure 2D), and from 56.7% (95% CI 54.7–58.7%) to 45.6% (95% CI 43.7–47.4%) in untreated patients ( Figure 2F).
Frequency of ALT and VL testing
Pre-COVID, the mean number of ALT measurements varied from 14 (95% CI 14–14) to 26 (95% CI 26–26) per 100 patients per month, with annual dips in August and December ( Figure 4A). From March 2020 to June 2021, this range reduced to between 7 (95% CI 7–7) and 14 (95% CI 14–14), with a loss of the seasonal patterns previously observed, and reaching a nadir of 7 per 100 patients (95% CI 6–7) in April 2020 during the first lockdown. The same trend was observed for VL ( Figure 4B), with mean numbers of measurements ranging from 7 (95% CI 7–7) to 12 (95% CI 12–12) per 100 patients pre-COVID, and from 2 (95% CI 2–2) to 7 (95% CI 7–7) during the COVID-19 period, with a nadir of 2 measurements per 100 patients (95% CI 2–2) in April 2020.
*Mean numbers of ALT and HBV DNA VL measurements per 100 patients per month during pre-COVID-19coronavirus disease 2019 (COVID-19, 2016–19) and COVID-19 (2020 and part of 2021) periods.Data are shown overall and stratified by treatment status for both viral load (VL, panels A, C, E) and alanine transferase (ALT, panels B, D, F). Dates of UK national COVID-19 lockdowns are denoted in overall plots. 95% CIs were calculated using the normal distribution (whereby standard error (SE) is estimated by
sn with n denoting sample size and s denoting standard deviation).*
Frequency of testing by HBV treatment status
VL and ALT measurements were more frequent in treated ( Figure 4 C, D) compared to untreated ( Figure 4 E, F) patients throughout the study period. In treated patients pre-COVID, mean number of ALT measurements fluctuated between and within years but remained >25 measurements per 100 patients per month ( Figure 4C); hence, treated patients had ALT measured on average once every 4 months (in keeping with the routine interval for clinic visits in patients on treatment).
Mean numbers of monthly tests fluctuated between 19 (95% CI 18–21) and 35 (95% CI 34–37) per 100 patients during the COVID-19 period but were generally significantly lower compared to pre-COVID-19 years. This pattern was also observed for VL, with mean numbers of measurements ranging from 11 (95% CI 11–12) to 23 (95% CI 23–24) during pre-COVID-19 years and 6 (95% CI 6–7) to 13 (95% CI 12–13) during the COVID-19 period ( Figure 4D).
In untreated patients pre-COVID, mean number of ALT measurements per 100 patients per month ranged from 10 (95% CI 10–11) to 23 (95% CI 22–23), with a significant drop in the COVID-19 period to between 5 (95% CI 5–5) and 15 (95% CI 14–15) ( Figure 4E). This pattern was also observed for VL, with pre-COVID-19 and COVID-19 measurements ranging from 6 (95% CI 6–7) to 11 (95% CI 11–11) and from 2 (95% CI 2–2) to 7 (95% CI 7–7) measurements per 100 patients, respectively ( Figure 4F).
Discussion/conclusions
These data demonstrate the negative impact of the COVID-19 pandemic on routine clinical surveillance for patients with CHB infection in the UK. Reduction in rates of surveillance closely track SARS-CoV-2 incidence ( Figure 3) and thus periods of population lock-down.
During lockdown periods, much clinical care was switched to telemedicine ^ 13, 14 ^, intended to maintain contact between patients and healthcare providers, but at the detriment of laboratory monitoring. Although patients may have an option to attend phlebotomy appointments, services have been stretched, and clinicians and/or patients may have elected to defer routine blood tests. Telephone appointments are impractical for certain patients, and contact may have been lost altogether – for example, for those who do not communicate confidently in English. Furthermore, CHB patients who left the UK early in the course of the pandemic may have been unable to return due to travel restrictions, thereby foregoing routine surveillance.
The impact of the pandemic was seen across treated and untreated individuals. However, the impact on ALT measurement was greater in those on treatment during lockdowns.
We were unable to investigate how imaging-based surveillance strategies were impacted due to lack of complete elastography and ultrasound data in our current dataset. Furthermore, as complications of CHB evolve over the long-term (months to years), it is not yet possible to quantify how service disruptions may impact incidence of HCC and other adverse endpoints. Surveillance disruption may be associated with an increased risk of CHB progression and delays in starting antiviral therapy. Further prospective data are required to determine the impact on long-term outcomes.
Our data represent only five large, urban centres, in the South East of England; trends may differ across settings and additional data will be required to determine the extent to which our observations apply in other regions. HIC data collection is being expanded ^ 10 ^, providing enhanced opportunities to incorporate a wider view of the UK over time. Effort and resources are required to refine telemedicine services and optimise access to laboratory surveillance ^ 15 ^, re-establish face-to-face services and catch-up on monitoring and interventions. Future analyses are warranted to investigate how imaging surveillance and telemedicine service uptake have been impacted when these data become available in the NIHR HIC database. Longitudinal follow-up is warranted to ascertain how COVID-attributable disruptions will impact the incidence of HCC and other relevant endpoints, and to ensure activity is re-aligned to support progress to elimination goals.
Data availability
Individual-level electronic health record were used to conduct this investigation. Data are anonymised and collected using National Institute for Health Research (NIHR) Health Informatics Collaborative (HIC) data resources. In order to ensure patient confidentiality and data privacy, raw underlying data cannot be made publicly available, and data are made available to researchers via a controlled access repository. The NIHR HIC Viral Hepatitis data repository is hosted by Oxford University Hospitals NHS Foundation Trust under a governance framework which includes a data sharing agreement and terms on confidentiality, contractual responsibilities, intellectual property, and publication. A scientific steering committee, comprised of at least one representative from each participating NIHR HIC site, meets regularly to review data collection, feedback progress on active projects, consider updates to the database, and review all data requests. Any potential collaborations are welcomed, and data are available to researchers on request following review by the steering committee. Further details are available at https://hic.nihr.ac.uk. Queries regarding data access should be directed to [email protected].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global Health Sector Strategy on viral hepatitis 2016– 2021.Geneva;2016; [cited 2021 Jun 14]. Reference Source
- 2Sarin SK Kumar M Lau GK : Asian-Pacific clinical practice guidelines on the management of hepatitis B: a 2015 update. Hepatol Int. 2016;10:1–98. 10.1007/s 12072-015-9675-4 26563120 PMC 4722087 · doi ↗ · pubmed ↗
- 3Terrault NA Lok ASF Mc Mahon BJ : Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67(4):1560–99. 10.1002/hep.29800 29405329 PMC 5975958 · doi ↗ · pubmed ↗
- 4European Association for the Study of the Liver (EASL): EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67(2):370–98. 10.1016/j.jhep.2017.03.021 28427875 · doi ↗ · pubmed ↗
- 5European Association for the Study of the Liver: The summarized of EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67:370–98.28427875 10.1016/j.jhep.2017.03.021 · doi ↗ · pubmed ↗
- 6National Institute for Health and Care Excellence: Hepatitis B (chronic): diagnosis and management.2017;2016:1–36. Reference Source 32068988 · pubmed ↗
- 7Pley CM Mc Naughton AL Matthews PC : The global impact of the COVID-19 pandemic on the prevention, diagnosis and treatment of hepatitis B virus (HBV) infection. BMJ Glob Health. 2021;6(1):e 004275. 10.1136/bmjgh-2020-004275 33402334 PMC 7786543 · doi ↗ · pubmed ↗
- 8Wingrove C Ferrier L James C : The impact of COVID-19 on hepatitis elimination. Lancet Gastroenterol Hepatol. Elsevier Ltd;2020;5(9):792–4. 10.1016/S 2468-1253(20)30238-7 32730783 PMC 7384773 · doi ↗ · pubmed ↗