Letter to the Editor Regarding the Article, “Development of a Nomogram to Predict Clinically Relevant Postoperative Pancreatic Fistula After Pancreaticoduodenectomy on the Basis of Visceral Fat Area and Magnetic Resonance Imaging: A Nomogram Incorporating the Inflammatory Burden Index and Drainage Fluid Amylase Levels”
Jiayue Zou, Xiaofeng Xue, Lei Qin

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
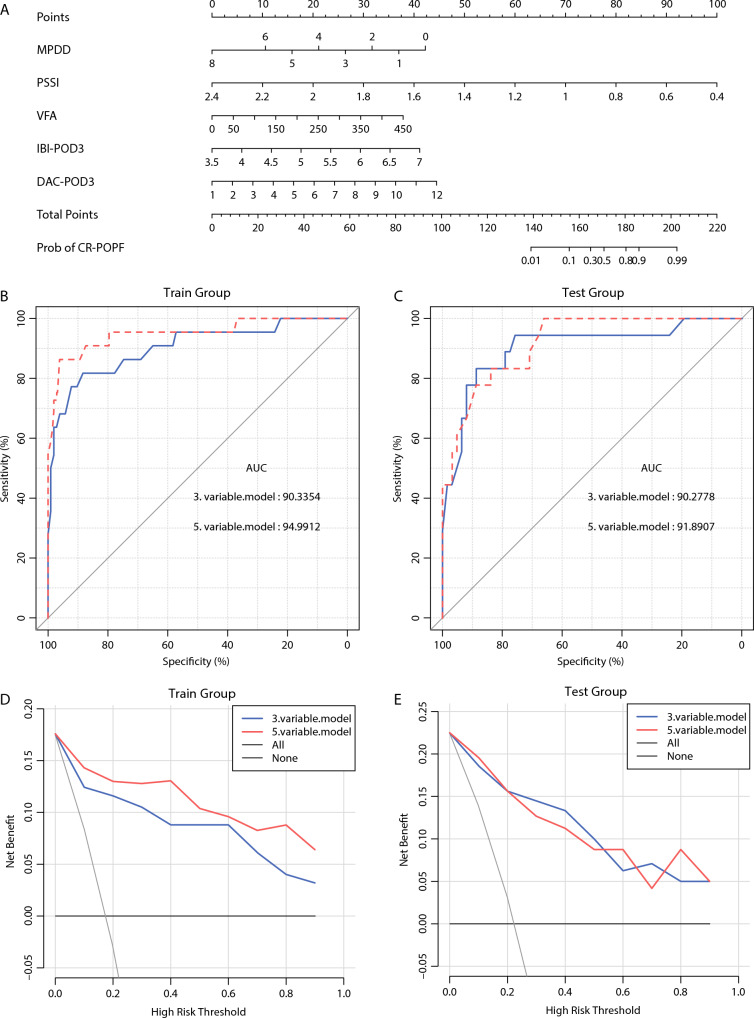 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Pancreatitis Pathology and Treatment · Inflammatory Biomarkers in Disease Prognosis
Dear editor,
We appreciate your suggestions in the article titled, “Development of a Nomogram to Predict Clinically Relevant Postoperative Pancreatic Fistula After Pancreaticoduodenectomy on the Basis of the Visceral Fat Area and Magnetic Resonance Imaging.”
Clinical data from 205 patients who underwent pancreaticoduodenectomy (PD) were collected and randomly divided into a training set and a testing set. Data were missing due to the retrospective design of the study. Data on the inflammatory burden index (IBI) were collected before surgery and on postoperative day (POD) 3. Data on drainage fluid amylase concentrations (DFAC) and serum amylase concentrations (SAC) were collected on PODs 1 and 3, and the ratio of drainage fluid to serum amylase concentrations (DFSAC) was calculated. The subgroups with clinically relevant postoperative pancreatic fistula (CR-POPF) were compared using the Mann-Whitney U test.
The results showed that preoperative IBI did not differ significantly between the patients with and those without CR-POPF (P = 0.713). In turn, significant between-group differences in IBI were observed on POD3 (P < 0.001), in DFSAC on POD1 (P = 0.004), in DFSAC on POD3 (P < 0.001), in DFAC on POD1 (P < 0.001), and in DFAC on POD3 (P < 0.001) (Table 1).Table 1. Comparison of clinical variables between the patients with and those without clinically relevant postoperative pancreatic fistula (CR-POPF)VariableCR-POPFnon-CR-POPFP ValuePreoperative IBI2.559 (− 2.101 to 4.95)2.514 (− 3.602 to 5.483)0.713IBI on POD35.612 (4.729 to 7.472)5.172 (2.128 to 6.956)<0.001DFAC on POD17.342 (5.078 to 10.689)5.911 (− 0.693 to 11.076)<0.001DFAC on POD37.496 (4.519 to 11.091)5.332 (0.833 to 9.711)<0.001DFSAC on POD18.586 (0.172 to 4984.205)2.805 (0.016 to 1457.567)0.004DFSAC on POD316.544 (0.303 to 547.974)2.711 (0.0149 to 774.413)<0.001IBI inflammatory burden index; POD postoperative day; DFAC drainage fluid amylase concentrations; DFSAC ratio of drainage fluid to serum amylase concentrations
Patient characteristics did not differ significantly at baseline between the training and testing sets (P > 0.05; Table 2). Clinical variables were analyzed by uni- and multivariate logistic regression. Both IBI on POD3 and DFAC on POD3 were added to the predictive model such that the final model contained five variables: visceral fat area (VFA), pancreas-to-spleen signal intensity ratio (PSSI), main pancreatic duct diameter (MPDD), IBI on POD3, and DFAC on POD3 (Tables 3, 4). Among the patients with POPF, IBI on POD1, DFSAC on POD1, DFSAC on POD3, and DFAC on POD1 differed significantly but were not included in the model.Table 2. Comparison of clinical variables between the training and testing setsVariableTraining setTesting setP ValuePreoperative IBI2.576 (− 2.102 to 5.483)2.410 (− 3.602 to 5.418)0.413IBI-POD35.290 (3.638 to 6.956)5.227 (2.128 to 7.472)0.696DFAC-POD16.304 (2.163 to 10.416)6.624 (− 0.693 to 11.076)0.816DFAC-POD35.657 (1.482 to 11.091)5.706 (0.833 to 10.994)0.502DFSAC-POD14.803 (0.027 to 636.053)2.318 (0.016 to 4984.205)0.189DFSAC-POD34.060 (0.104 to 774.413)3.362 (0.0149 to 547.974)0.258IBI inflammatory burden index; POD postoperative day; DFAC drainage fluid amylase concentrations; DFSAC ratio of drainage fluid to serum amylase concentrationsTable 3Analysis of clinical variables by univariate logistic regressionCharacteristicsOR95 % CIP ValueBMI1.321.11–1.57<0.001DFAC on POD11.471.11–1.970.01DFAC on POD31.811.35–2.43<0.001IBI on POD35.982.39–14.99<0.001MPDD0.580.40–0.84<0.001PSSI00–0.08<0.001VFA1.011.01–1.02<0.001OR odds ratio; CI confidence interval; BMI body mass index; DFAC drainage fluid amylase concentrations; POD postoperative day; IBI inflammatory burden index; MPDD main pancreatic duct diameter; PSSI pancreas-to-spleen signal intensity ratio; VFA visceral fat areaTable 4Analysis of risk factors by multivariate logistic regressionVariablesOR95 % CIP ValueDFAC on POD31.771.10–2.830.018IBI on POD35.071.35–19.060.016MPDD0.470.27–0.840.010PSSI00–0.060.002VFA1.011.00–1.020.043OR odds ratio; CI confidence interval; DFAC drainage fluid amylase concentrations; POD postoperative day; IBI inflammatory burden index; MPDD main pancreatic duct diameter; PSSI pancreas-to-spleen signal intensity ratio; VFA visceral fat area
The equation for the final five-variable model was
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$ \begin{aligned} X & = \left( {1.6990 \times {\text{IBI}} - {\text{POD}}3} \right) + \left( {0.5845 \, \times {\text{DFAC}} - {\text{POD}}3} \right) \\ & \quad + \left( {0.0122 \times {\text{VFA}}} \right){-}\left( {7.2302 \times {\text{PSSI}}} \right){-}\left( {0.7638 \times {\text{MPDD}}} \right). \\ \end{aligned} $$\end{document}The nomogram was plotted using the rms package in R version 3.5.0 (Fig. 1A). The area under the curve (AUC) of the final model in the training set was 0.950, slightly higher than the AUC of the original three-variable model (0.903). The AUC of the final model in the testing set was 0.919, slightly higher than the AUC of the original model (0.903) (Fig. 1B, C).Fig. 1A The optimized prediction model in which five variables were scored, with higher total scores indicating a higher risk for occurrence of clinically relevant postoperative pancreatic fistula. B, C Comparison between the original three-variable model and the final five-variable model in the testing and training sets. The area under the curve (AUC) of the original and final models was 0.903 and 0.950 in the training set and 0.903 and 0.919 in the testing set. D, E Decision curve analysis of the two models in both datasets.
Previous studies showed that DFAC on POD1 and POD3 determined the time when the drainage tubes were removal, consistent with our results. Decision curve analysis showed that the final model was superior to the original model in the training set (Fig. 1D, E). Integrated discrimination improvement (IDI) of the final model relative to the original model was 0.146 (95 % confidence interval [CI] 0.049–0.243; P = 0.003) in the training set and 0.021 in the testing set (95 % CI 0.058–0.099; P = 0.608) (Table 5).Table 5. Integrated discrimination improvement (IDI) of the final model compared with the three-variable modelDatasetIDI95 % CIP ValueTraining0.1460.049 to 0.2430.003Testing0.021− 0.058 to 0.0990.608CI confidence interval
The risk of POPF can be predicted by DFAC and SAC.^1,2^ Inadequate blood supply to the anastomosis and local inflammation after PD are reflected by high SAC, impairing anastomotic healing and potentially leading to POFP. Consistent with our findings, high SAC and acute pancreatitis were shown to correlate with POPF.^3^ Additionally, DFSAC on POD3 can predict CR-POPF.^4^ Although DSFAC differed significantly between the patients with and those without CR-POPF, this parameter was not included in the model.
The IBI is used to assess the inflammatory status and survival in cancer patients. Higher IBI correlates with poorer outcomes and reduces patients’ quality of life and physical function.^5,6^ The neutrophil-to-lymphocyte ratio and C-reactive protein (CRP) are measures of systemic inflammation. Large surgical incisions and prolonged surgical time may affect local and systemic inflammation, further impairing the nutritional status and local healing and leading to delayed anastomotic growth and fistula development.^7^
The inclusion of DFAC on POD3 and IBI on POD3 increased the predictive ability of the final model. Thus, this model can guide the early removal of drainage tubes and postoperative recovery. However, this model could not predict CR-POPF preoperatively due to the inclusion of postoperative indicators.
A good model must make predictions as early and accurately as possible using simple data and easily accessible methods. The predictions made by the original model were based on preoperative variables. Moreover, although the predictive performance of the original model in the training set was slightly lower than that of the final model, the former identified patients at high risk of CR-POPF earlier for treatment and decision-making in the immediate preoperative period.
A larger multicenter study was not performed because of limited resources, reducing the generalizability of the findings. Nonetheless, we intend to conduct a large prospective clinical trial using the improved model to reduce the incidence of pancreatic fistula in our center.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fukada M Murase K Higashi T Yokoi R Tanaka Y Okumura N Early predictive factors for postoperative pancreatic fistula after distal pancreatectomy for pancreatic cancer Cancer Diagn Progn.2022245246110.21873/cdp.1012835813012 PMC 9254104 · doi ↗ · pubmed ↗
- 2Fukada M Murase K Higashi T Fujibayashi S Kuno M Yasufuku I The pancreas-to-muscle signal intensity ratio on T 1-weighted MRI as a predictive biomarker for postoperative pancreatic fistula after distal pancreatectomy: a single-center retrospective study World J Surg Oncol.20222025010.1186/s 12957-022-02718-835932021 PMC 9354425 · doi ↗ · pubmed ↗
- 3Paik KY Oh JS Kim EK Amylase level after pancreaticoduodenectomy in predicting postoperative pancreatic fistula Asian J Surg.20214463664010.1016/j.asjsur.2020.11.02233323317 · doi ↗ · pubmed ↗
- 4Fukada M Murase K Higashi T Yasufuku I Sato Y Tajima JY Drain fluid and serum amylase concentration ratio is the most reliable indicator for predicting postoperative pancreatic fistula after distal pancreatectomy BMC Surg.2023238710.1186/s 12893-023-01980-137046241 PMC 10091553 · doi ↗ · pubmed ↗
- 5Xie H Ruan G Wei L Deng L Zhang Q Ge Y The inflammatory burden index is a superior systemic inflammation biomarker for the prognosis of non-small cell lung cancer J Cachexia Sarcopenia Muscle.20231486987810.1002/jcsm.1319936852672 PMC 10067487 · doi ↗ · pubmed ↗
- 6Xie H Ruan G Ge Y Zhang Q Zhang H Lin S Inflammatory burden as a prognostic biomarker for cancer Clin Nutr.2022411236124310.1016/j.clnu.2022.04.01935504166 · doi ↗ · pubmed ↗
- 7Cheng X Wang C Liu Y Zhang X Zhou L Lin Z Effects of different radical distal gastrectomy on postoperative inflammatory response and nutritional status in patients with gastric cancer Front Surg.202310111247310.3389/fsurg.2023.111247337009613 PMC 10050336 · doi ↗ · pubmed ↗