A Critically Ill Influenza A-Positive Patient With Spontaneous Pneumomediastinum, Superimposed Bacterial Pneumonia, and Bilateral Pneumothoraces
Kirstin Acus, Stephen Meigher, Vinay Saggar

TL;DR
A young man with no prior health issues developed severe complications from Influenza A, including lung and chest issues requiring urgent care.
Contribution
This case highlights under-recognized severe complications of Influenza A in young adults, emphasizing the need for thorough evaluation.
Findings
A 20-year-old male with Influenza A developed pneumomediastinum, bacterial pneumonia, and pneumothoraces.
Severe complications from Influenza A may be under-reported, especially in young adults and children.
Emergency providers should consider extensive testing for unstable Influenza A patients to detect life-threatening conditions.
Abstract
Influenza most often causes a febrile viral syndrome inclusive of pulmonary irritation with cough, shortness of breath, and congestion. However, severe infection can also occur, causing significant viral pneumonia with Type 1 respiratory failure. and rare but life-altering complications such as pneumomediastinum, secondary bacterial pneumonia, acute respiratory distress syndrome (ARDS), viremia, and death. This was a case of a 20-year-old male with no significant past medical history who presented to the emergency department with shortness of breath and chest discomfort and was found to have Influenza A with Type I respiratory failure requiring High Flow Nasal Cannula (HFNC) and extensive pneumomediastinum, superimposed bacterial pneumonia, and bilateral pneumothoraces. It is possible that complications secondary to influenza A infections could be under-reported due to the extremely…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
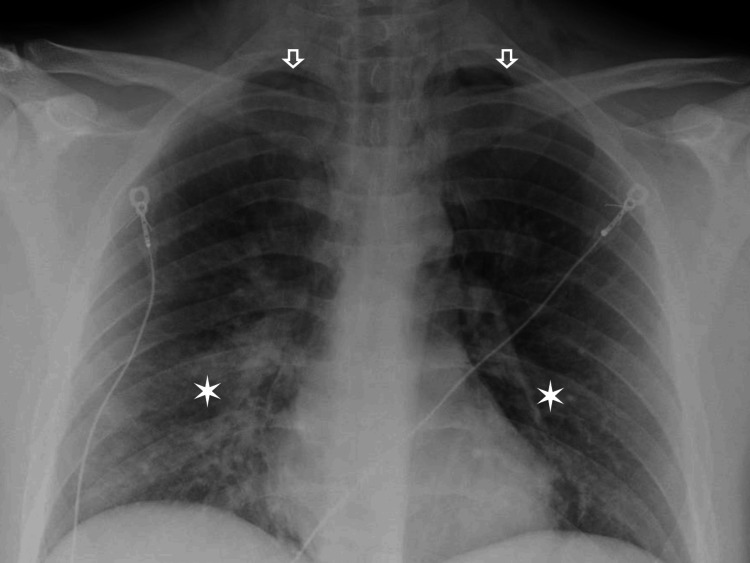 Figure 1
Figure 1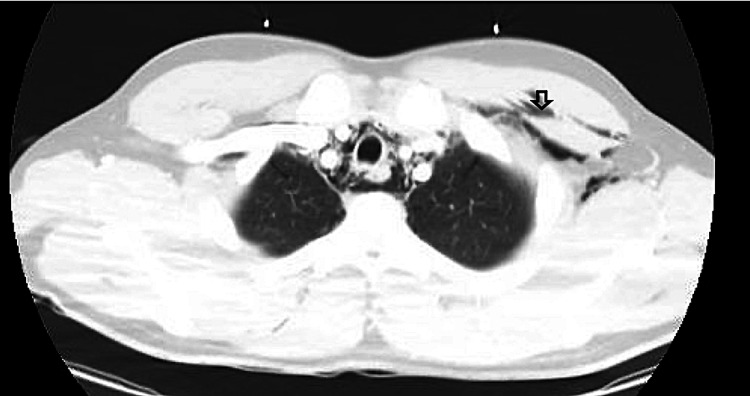 Figure 2
Figure 2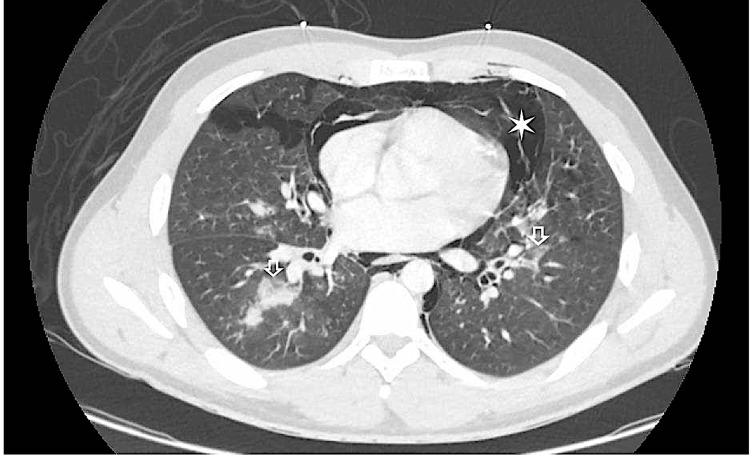 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumothorax, Barotrauma, Emphysema · Pneumonia and Respiratory Infections · Pneumocystis jirovecii pneumonia detection and treatment
Introduction
Annual seasonal influenza epidemics have caused a predictable morbidity and healthcare strain across the world every winter season for the majority of modern history. During the 2023-2024 influenza season, it is estimated that 25 to 50 million infections occurred with up to 24 million healthcare visits, 670,000 hospitalizations, and somewhere between 17,000 to 98,000 deaths in the United States alone [1]. Influenza most often causes a febrile viral syndrome inclusive of pulmonary irritation with cough, shortness of breath, chest pain or congestion, as well as myalgias, malaise, and fatigue. However, severe infection can also occur causing significant viral pneumonia with hypoxemic respiratory failure and complications such as pneumomediastinum, secondary bacterial pneumonia, ARDS, viremia, and death [2]. This was especially noted in case reports during the H1N1 Influenza A swine flu epidemic and while rare, has been documented in pediatric cases [3-6].
Although rare and sparsely documented, these complications can often be dramatic enough to include life-altering complications, especially complicated pneumomediastinum [7-9]. This was a case of a 20-year-old male with no significant past medical history who presented to the emergency department with shortness of breath and chest discomfort and was found to have Influenza A with Type I respiratory failure requiring high-flow nasal cannula (HFNC) and extensive pneumomediastinum, superimposed bacterial pneumonia, and bilateral pneumothoraces.
Case presentation
A 20-year-old male with no significant past medical history presented to the emergency department with the chief complaints of persistent dry cough, chest pressure, and shortness of breath. The patient reported that the symptoms first began as two days of a progressively worsening dry cough, as well as mild nasal congestion and isolated episodes of non-bloody, non-bilious emesis. The patient then awoke with severe chest discomfort and shortness of breath, after which he called emergency medical services (EMS). He reports not having received his influenza vaccine earlier in the year due to an unspecified allergy.
Vital signs were significant for the patient being febrile to 39.2 °C and tachycardic to 121 bpm. Pertinent physical exam findings included the patient seeming ill-appearing, diaphoretic, and selectively leaning forward in the stretcher throughout the evaluation. The patient was in mild respiratory distress with slight dyspnea while speaking and lung sounds were diminished in upper lung fields.
Labs were drawn and found to be significant for leukocytosis with a white blood cell count of 17 x 10^3^/uL, D-Dimer of 1,021 ng/ml DDU, a comprehensive metabolic panel within normal limits, and a respiratory panel positive for Influenza A. A portable chest x-ray showed bilateral opacities concerning for developing pneumonia (Figure 1), with a subsequent, emergent CT chest showed a large volume of pneumomediastinum, trace bilateral pneumothoraces, bilateral cervical and upper thoracic subcutaneous emphysema, and scattered opacifications (Figures 2, 3).
Upright Chest Xray The star notes the basilar opacities. The arrow indicates trace bilateral pneumothoraces
CT Chest with IV ContrastThe arrow on the figure illustrates examples of cervical/upper thoracic scattered emphysema
CT Chest with IV ContrastThe star on the figure illustrates large-volume pneumomediastinum. The arrow shows the scattered patchy ground-glass consolidative opacities throughout the bilateral lungs concerning for pneumonia.
The patient was started on ceftriaxone and azithromycin for community-acquired pneumonia along with Tamiflu and admitted to the medical step-down unit for close monitoring with thoracic surgery consultation. The day after the initial presentation, the patient acutely decompensated requiring supplementary oxygen, which eventually escalated to 15L non-rebreather mask (NRB) followed by HFNC 50L/90% FiO2. The patient had an esophagogram done during admission which was negative for esophageal perforation and eventually was weaned to room air before being discharged 6 days after initial presentation back to home with pulmonary follow-up.
Discussion
Influenza A represents the bulk of seasonal influenza infections during epidemics and thus the lion's share of morbidity, complications, and severity. Patients with severe influenza A infection develop lower respiratory illness syndromes with significant cough, dyspnea, and pain. Occasional case reports have documented severe and prolonged Influenza A infection causing bronchial obstruction or necrotizing pneumonia leading to small airway rupture and pneumomediastinum with ARDS in middle-aged and elderly adults [10]. Coughing may be severe and exertionally limiting, as well as lead to posttussive complications such as spontaneous pneumothorax, and rarely, spontaneous pneumomediastinum.
Spontaneous pneumomediastinum was first described in 1827 by Laennec and further described with subcutaneous emphysema in a postpartum patient by Hamman in 1939 with historical recognition of the condition and his eponymous moniker Hamman Sign, representing audible pericardial air ‘crunching’ with cardiac contractility on auscultation [11,12]. Pneumomediastinum occurs when intrathoracic pressure gathers significantly enough to rupture small airways and force pressurized air retrograde along the peribronchial and perivascular sheath to the mediastinum and the pericardial sac [13]. Pneumopericardium and pneumomediastinum are intra-thoracic diseases known to be more frequent in young and normally healthy patients, likely in part due to looser and more mobile peribronchial sheaths. Leading causes of rupture include severe coughing fits, bronchial obstruction, and necrotizing pneumonia, each leading to increased intrapulmonary pressure and small airway or alveolar rupture. Symptoms include persistent, severe cough, dyspnea, sharp chest pain, dysphonia, and neck swelling. Diagnosis may be captured on chest x-ray but the confirmatory study of choice is a non-contrast chest CT [13].
Supportive and conservative management is the mainstay of treatment in both severe influenza A and pneumomediastinum. Atmospheric air is absorbed from its small intrathoracic collections while ruptured small airways heal. Rarely, with high intrathoracic pressures or pericardial involvement, tension pneumomediastinum, pneumothorax, or tension pneumopericardium may develop. Treatment aims to resolve any life-threatening intrathoracic disease such as thoracostomy for a developing pneumothorax. Esophageal rupture should always be considered in cases of pneumomediastinum temporally related to vomiting. Very rarely, invasive procedures such as thoracostomy, sternotomy, and mediastinotomy are warranted [14]. The vast majority of the time, pneumomediastinum, subcutaneous emphysema, and pneumothoraces secondary to an influenza A infection are benign, self-limiting conditions. Appropriate treatment usually includes monitoring and supplementary O_2_ assistance as needed via nasal cannula or high-flow.
Conclusions
Our patient was a rare case of an otherwise healthy young male with no pulmonary disease who endured significant complications from an acute Influenza A infection. It is possible that complications secondary to influenza A infections could be under-reported due to the extremely high prevalence of the viral infection in this country. The degree of pneumomediastinum found in this patient, as well as the delayed sequela and acute decompensation the patient experienced, should serve as a reminder to all emergency medicine providers that when evaluating these patients, various tests should be considered on a case-by-case basis to risk-stratify the likelihood of an emergent pathology.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 12023-2024 U.S. flu season: preliminary in-season burden estimates 4 2024 2024 https://www.cdc.gov/flu/about/burden/preliminary-in-season-estimates.htm
- 2Complications of viral influenza Am J Med Rothberg MB Haessler SD Brown RB 25826412120081837468010.1016/j.amjmed.2007.10.040PMC 7172971 · doi ↗ · pubmed ↗
- 3Spontaneous pneumomediastinum: a complication of swine flu Asian Cardiovasc Thorac Ann Padhy AK Gupta A Aiyer P Jhajhria NS Grover V Gupta VK 99810002320152593991310.1177/0218492315585907 · doi ↗ · pubmed ↗
- 4Spontaneous pneumomediastinum in H 1N 1 infection: uncommon complication of a common infection J R Coll Physicians Edinb Chekkoth SM Supreeth RN Valsala N Kumar P Raja RS 2983004920193180845610.4997/JRCPE.2019.409 · doi ↗ · pubmed ↗
- 5Spontaneous pneumomediastinum in a child due to 2009 pandemic influenza A (H 1N 1) virus Turk J Pediatr Ozdemir H Kendirli T Dinçaslan HU Ciftçi E Ince E 648651522010 https://www.proquest.com/openview/0eb 51de 30297 e 76907 b 134ec 51d 373a 5/1?pq-origsite=gscholar&cbl=3523621428200 · pubmed ↗
- 6Pneumomediastinum associated with influenza A infection N Engl J Med Mansbridge CT Inada-Kim M 0378201810.1056/nejmicm 170284929298153 · doi ↗ · pubmed ↗
- 7Pneumothorax, pneumomediastinum, subcutaneous emphysema and pneumorrhachis as complications of common flu Am J Case Rep Patel V Raval G Gavadia K 1982011320122356952810.12659/AJCR.883332 PMC 3615911 · doi ↗ · pubmed ↗
- 8Spontaneous subcutaneous emphysema and pneumomediastinum associated with influenza B virus in a young male adult: a case report Cureus Alnofal WY Alshadely MR Khatib MA 013202110.7759/cureus.13077 PMC 793177733680617 · doi ↗ · pubmed ↗