Late Onset Hypercalcemia in an HIV Patient as a Manifestation of Immune Reconstitution Inflammatory Syndrome (IRIS)
Mallak Zatreh, Betty Drees, Jignesh Shah

TL;DR
An HIV patient developed late-onset hypercalcemia due to immune reconstitution inflammatory syndrome (IRIS) triggered by a granulomatous infection.
Contribution
This case highlights IRIS as a novel cause of hypercalcemia in HIV patients with granulomatous infections.
Findings
Hypercalcemia occurred in an HIV patient with Mycobacterium avium-intracellulare (MAI) infection.
Normal levels of vitamin D metabolites were unexpectedly found to be the cause of hypercalcemia.
Treatment with steroids successfully managed the hypercalcemia linked to IRIS.
Abstract
Hypercalcemia in human immunodeficiency virus (HIV) patients can be challenging due to various underlying mechanisms. 1,25- dihydroxycholecalciferol (1,25 (OH)2 vitamin D)-mediated hypercalcemia due to increased activity of extrarenal 1-alpha hydroxylase is one of the well-known mechanisms of hypercalcemia described in HIV patients. Mycobacterium avium-intracellulare (MAI) is a granulomatous disease that can cause hypercalcemia due to ectopic production of alpha -1 hydroxylase and result in increased levels of 1,25 (OH)2 vitamin D. Herein, we present a case of “late-onset” hypercalcemia in a patient with HIV/AIDS and MAI infection in the setting of suspected immune reconstitution inflammatory syndrome (IRIS). The hypercalcemia workup showed an inappropriately average level of 1,25 (OH)2 vitamin D while the rest of the workup was unrevealing. Unusually normal levels of vitamin D…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
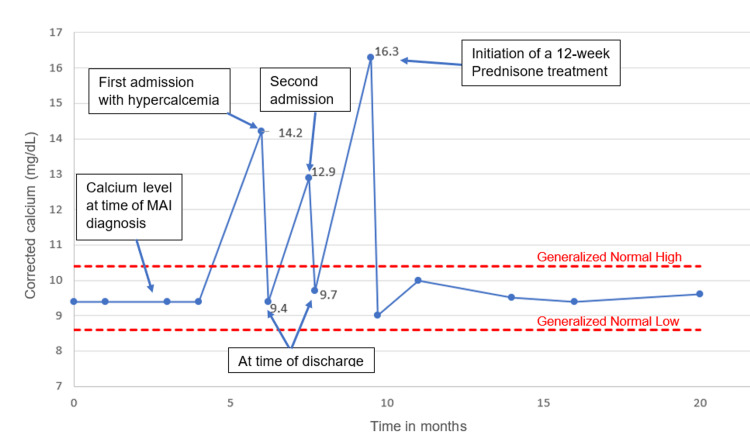 Figure 1
Figure 1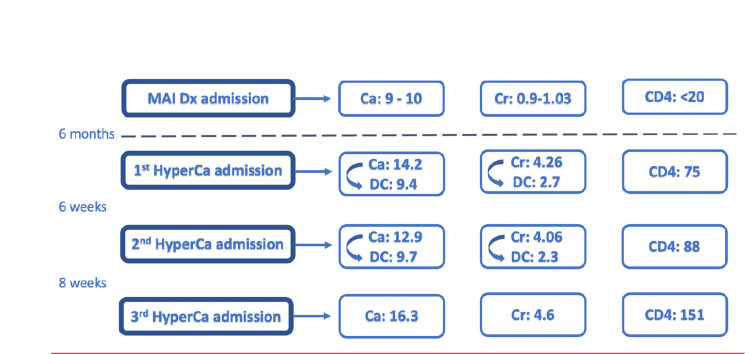 Figure 2
Figure 2| First hypercalcemia presentation | Second presentation | Third presentation | Reference range | |
| Corrected calcium | 14.2 | 12.9 | 16.3 | 8.4-10.4 mg/dL |
| Creatinine | 4.26 | 4.06 | 4.6 | 0.8-1.2 mg/dL |
| Phosphorus | 3.1 | - | - | 2.3-5.6 mg/dL |
| CD4 level | 75 | 88 | 151 | 500-1500 cells/mm3 |
| PTH | 11.8 | - | - | 12-88 pg/mL |
| 25 (OH) vitamin D | 13.1 | - | - | 30-100 ng/mL |
| 1,25 (OH)2 vitamin D | 52 | - | - | 18-72 pg/mL |
| PTHrP | 25 | - | - | 10-27 pg/mL |
| Author | Diagnosis | PTH | PTHrP | 25-(OH) Vit D | 1,25 (OH)2 Vit D |
| Parsons CE et al., 2017 [ | MAI | Low | Normal | Normal | Normal: 27 pg/mL (Ref 18-78) |
| Chatterjee T et al., 2021 [ | MAI | Low | Normal | Normal | Low: 11 pg/mL (Ref 18-78) |
| Shrayyef MZ et al., 2011 [ | Sarcoidosis | Low | Normal | Normal | Normal |
| Kallas M et al., 2010 [ | Granulomatous myositis | Low | Low | Normal | Normal: 64.9 pg/mL (Ref 22–79) |
| Nielsen CT et al., 2009 [ | Mycobacterium Marinum | Low | Not measured | Low | Low: 17.49 pg/mL (Ref 25-75) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Sarcoidosis and Beryllium Toxicity Research · Pneumocystis jirovecii pneumonia detection and treatment
Introduction
Hypercalcemia is associated with granulomatous disease. Both tuberculous and non-tuberculous Mycobacterium are associated with hypercalcemia. Mycobacterium avium-intracellulare (MAI) is a non-tuberculous mycobacterium that can cause hypercalcemia. The mechanism of hypercalcemia in granulomatous diseases is due to excessive production of 1,25 (OH)2 vitamin D by activated macrophages that produce alpha-1 hydroxylase enzyme [1]. One unique mechanism of hypercalcemia in HIV patients is through granuloma formation where the ectopic production of alpha -1 hydroxylase is unmasked after initiation of antiretroviral therapies (ART) as a manifestation of immune reconstitution inflammatory syndrome (IRIS) [2]. Although the mechanism of hypercalcemia in granulomatous disease is thought to be related to vitamin D dysregulation, this does not always correlate with vitamin D metabolite levels [3]. Below, we describe a disseminated MAI infection with severe hypercalcemia and an inappropriately normal 1,25-(OH)2 vitamin D without any other standard or uncommon causes of hypercalcemia.
Case presentation
A 55-year-old male with a past medical history of HIV presented to the hospital with recurrent fever. Workup was significant for an undetectable CD4 count, a viral load of 3,000,000 copies/mL, and a positive acid-fast bacilli blood culture that eventually grew MAI. As a result, ethambutol, rifabutin, and azithromycin were started. Two weeks after the initiation of MAI treatment, antiretroviral therapy (ART) was started, and the patient was eventually discharged. Six months after initiating ART, the patient was rehospitalized with nausea, dizziness, and abdominal discomfort, which all began on the day of presentation. This patient denied any excessive milk intake, vitamin D, calcium, or multivitamin supplements; no recent thiazide diuretics or non-steroidal anti-inflammatory drugs use was noted. The infectious disease clinic notes indicated nonadherence to ART, with the most recent CD4 count after initiation of ART for at least 5 months being 64 cells/mm3 (reference 500-1500 cells/mm^3^).
On physical examination, the patient was cachectic with a temperature of 36.3°C, blood pressure of 132/83 mmHg, heart rate of 83 beats/min, respiratory rate of 15/min, and an oxygen saturation of 98% on room air. The initial workup showed a low CD4 count and elevated levels of serum creatinine, calcium, and ionized calcium. A hypercalcemia workup revealed decreased parathyroid hormone (PTH) levels, a low level of 25-hydroxycalciferol, normal upper limit of 1,25 (OH)2 vitamin D level, and a normal PTH-related peptide (PTHrP). The laboratory work-up is summarized in Table 1. Urine calcium was high at 498 mg/24 hours. Further investigations, including serum protein electrophoresis, urine protein electrophoresis, Kappa and Lambda free light chain, and skeletal survey, did not show monoclonal gammopathy, elevated levels, or osteolytic lesion, respectively.
The kidney and abdominal ultrasound were normal except for nonobstructive renal calculi. The hypercalcemia was treated with intravenous fluids, calcitonin, and pamidronate, with normalization of serum calcium and improvement in the patient’s condition and symptoms within 48 hours. Renal function improved with hydration and improvement of hypercalcemia but did not return to normal, and serum creatinine remained at 2.7 mg/dL. The patient declined further workup and was discharged after normalization of serum calcium level. However, six weeks later, the patient presented again with similar symptoms and similar lab results of hypercalcemia and acute kidney injury, for which the patient received intravenous fluids and calcitonin. Additional workup was pursued during this admission. Computed tomography (CT) scan of the chest revealed a soft tissue density in the right perihilar region posterior to the superior vena cava, for which endobronchial ultrasound (EBUS) was recommended. Abdominal MRI showed diffuse lymphadenopathy. A kidney biopsy was performed, which showed calcium-related deposits with tubular injury, suggesting hypercalcemia-related kidney injury, with no granulomatous interstitial inflammation noted. The patient was discharged after further diagnostic evaluation was declined, with plans to follow up in the outpatient setting.
Eight weeks after discharge, the patient was seen in the clinic where serum calcium and creatinine were found to be elevated. As a result, the patient was admitted for the third time and treated with intravenous fluids and calcitonin. Given the patient's reluctance to undergo invasive workup, including biopsy, malignancy, particularly lymphoma, remained a differential diagnosis. Despite the absence of a definitive diagnosis, empiric treatment with glucocorticoids was implemented.
After finishing a 12-week course of prednisone therapy with tapering, calcium levels stabilized between 9-10 mg/dL and serum creatinine between 1.2-1.4 mg/dL. Subsequent follow-up visits demonstrated sustained normocalcemia without the recurrence of hypercalcemia. Notably, even after discontinuation of prednisone, the patient has remained normocalcemic for nearly two years, as illustrated in Figure 1.
Trends in calcium levels before and after initiating prednisone therapy. Image Credits: Mallak Zatreh
Discussion
Hypercalcemia in HIV-infected patients is rare but has been reported since the 1980s [4]. The reported mechanisms of hypercalcemia in HIV patients include increased osteoclastic activity due to infection (e.g., Cytomegalovirus infection), hypercalcemia of malignancy due to increased PTHrP (HTLV-1 infection causing T-cell Lymphoma), ectopic 1,25 (OH)2 vitamin D due to granulomatous diseases or lymphoma, and/or unknown mechanisms.
The most severe cases of hypercalcemia in HIV are most often seen with lymphomas [5]. Hypercalcemia has been well-described in granulomatous diseases. Both tuberculous and non-tuberculous mycobacterial (NTM) infections have been associated with hypercalcemia. The exact mechanism of hypercalcemia in NTM infections is not fully understood. It may be related to excessive production of 1,25 (OH)2 vitamin D by activated macrophages, despite the high levels of serum calcium. Interestingly, elevated 1,25 (OH)2 vitamin D levels are not always seen in hypercalcemia associated with granulomatous disorders in the setting of HIV infections. A review of the literature yielded a few cases of MAI-associated hypercalcemia in the setting of normal 1,25 (OH)2 vitamin D levels [3,6,7]. Table 2 lists some reported cases of hypercalcemia in patients with granulomatous disease where 1,25 (OH)2 vitamin D levels are not elevated. Parsons et al. described one case of MAI infection in an immunocompetent patient without HIV or malignancy who had hypercalcemia with normal 1,25 (OH)2 vitamin D levels [6]. Another case report by Chatterjee et al. reported a patient with MAI infection and hypercalcemia in the presence of low 1,25 (OH)2 vitamin D levels [7]. This observation of hypercalcemia in the setting of granulomatous disease and normal 1,25 (OH)2 vitamin D levels has led to the suggestion of other alternate mechanisms of hypercalcemia in granulomatous diseases, such as elevated calcitonin levels, increased bone resorption, or increased levels of free 1,25 (OH)2 vitamin D secondary to hypoalbuminemia [3, 8].
Another interesting aspect of this case is the timing of hypercalcemia in relation to MAI diagnosis. Our patient presented with hypercalcemia approximately six months after initiating MAI therapy and ART. This late onset of hypercalcemia could have been due to intermittent adherence to ART therapy, causing “late-onset” IRIS. After adherence to MAI and HIV treatment, the immune system was restored, and hypercalcemia developed. Figure 2 demonstrates the relationship between the onset of hypercalcemia and CD4 count improvement.
The temporal relationship between the onset of hypercalcemia and improvement in CD4 count, suggesting the possibility of IRIS presenting as hypercalcemia. MAI Dx: Mycobacterium Avium Intracellulare diagnosis. HyperCa: hypercalcemia. Ca: Calcium level (ref 8.4–10.4 mg/dL). Cr: serum creatinine level (ref 0.8-1.2 mg/dL). DC: Calcium/ Creatinine level at the time of discharge. CD4: CD4 count (ref 600-1500 cells/mm3).Image Credits: Mallak Zatreh
The suggested treatment of hypercalcemia in granulomatous disease, as well as in the setting of IRIS, is glucocorticoids. One of the mechanisms by which glucocorticoids reduce calcium levels in granulomatous diseases is through downregulating 1,25 (OH)2 vitamin D production by macrophages [10].
As shown in Figure 2, our patient had multiple recurrences of hypercalcemia, which in turn led to acute kidney injury (AKI) as well. This vicious cycle stopped after treatment with high-dose prednisone for 12 weeks, followed by tapering.
The decision to forgo invasive workup posed significant challenges in determining the underlying cause of hypercalcemia. While malignancy, particularly lymphoma, remained a primary concern, the sustained normocalcemia without recurrence post-steroid discontinuation suggested a less likely malignant etiology. The absence of hypercalcemia recurrence for an extended period supports the notion of hypercalcemia secondary to IRIS as the most likely underlying etiology.
Conclusions
HIV patients who are infected with granulomatous infections may or may not develop hypercalcemia. Hypercalcemia can develop early in the course of granulomatous infections or as a late manifestation, as shown in our case. The exact risk factors for hypercalcemia in these patients are still unknown. Genetic, environmental, and immunological factors have been suggested.
Although the known mechanism of hypercalcemia in HIV patients with granulomatous infections is due to increased activity of extrarenal 1-alpha hydroxylase with resultant increased levels of 1,25 (OH)2 vitamin D, there are a few case reports where hypercalcemia was found in the setting of normal or low 1,25 (OH)2 vitamin D and no other explanations for hypercalcemia. Although the exact mechanism for hypercalcemia in granulomatous infections with normal 1,25 (OH)2 vitamin D is still unknown, it is important to remain vigilant for this life-threatening complication and to treat patients appropriately.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Identification of 25-hydroxyvitamin D 3 1alpha-hydroxylase gene expression in macrophages Kidney Int Monkawa T Yoshida T Hayashi M Saruta T 5595685820001091607910.1046/j.1523-1755.2000.00202.x · doi ↗ · pubmed ↗
- 2Hypercalcemia during initiation of antiretroviral therapy in human immunodeficiency virus and Leishmania coinfection: a case report Medicine (Baltimore) Yu T Tang J 0102202310.1097/MD.0000000000033848 PMC 1027049737327295 · doi ↗ · pubmed ↗
- 3Hypercalcemia in two patients with sarcoidosis and Mycobacterium avium intracellulare not mediated by elevated vitamin D metabolites Am J Med Sci Shrayyef MZ De Papp Z Cave WT Wittlin SD 33634034220112176047510.1097/MAJ.0b 013e 31822224 c 3 · doi ↗ · pubmed ↗
- 4The acquired immunodeficiency syndrome and hypercalcemia West J Med Jacobs MB 4694711441986 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 1306675/3487172 PMC 1306675 · pubmed ↗
- 5Rapid onset of hypercalcemia from high-grade lymphoma in the setting of HIV-related immune reconstitution inflammatory syndrome Bone Rep Kim SJ Peluso MJ Wang Y Bikle D Shoback D Kim S 1001941020193062759910.1016/j.bonr.2018.100194 PMC 6319307 · doi ↗ · pubmed ↗
- 6A case of hypercalcaemia in an immunocompetent patient with Mycobacterium avium intracellulare JRSM Open Parsons CE Singh S Geyer HL 2054270417716614820172874810010.1177/2054270417716614 PMC 5507386 · doi ↗ · pubmed ↗
- 7Mycobacterium avium complex: an unusual cause of hypercalcemia ID Cases Chatterjee T Reddy YP Kandula M 026202110.1016/j.idcr.2021.e 01317 PMC 857748134786338 · doi ↗ · pubmed ↗
- 8Rare causes of calcitriol-mediated hypercalcemia: a case report and literature review J Clin Endocrinol Metab Kallas M Green F Hewison M White C Kline G 311131179520102042750110.1210/jc.2009-2673 · doi ↗ · pubmed ↗