Efficacy of neuromobilization in the treatment of low back pain: Systematic review and meta-analysis
Quanzheng Chen, Zhenshan Wang, Xian Chen, Jinchao Du, Shuna Zhang

TL;DR
This study reviews whether neuromobilization, a physical therapy technique, effectively reduces low back pain and disability.
Contribution
The study provides a systematic review and meta-analysis of neuromobilization's effectiveness for low back pain.
Findings
Neuromobilization improved Visual Analog Scale scores for pain in low back pain patients.
Neuromobilization improved Oswestry Disability Index scores in low back pain patients.
No significant improvement was found in straight leg raise outcomes with neuromobilization.
Abstract
Low back pain (LBP) is a leading cause of disability. Neuromobilization (NM) as a physical therapy technique, offers some degree of symptom improvement. However, some studies have shown that NM can significantly reduce the symptoms of LBP, while others have failed to find similar positive effects. This study aims to investigate the effectiveness of NM for LBP. A literature search was conducted across five databases (MEDLINE, Embase, Cochrane Library, PubMed, and Web of Science) from their inception to December 2023. Study main measures assessed pain, disability, and straight leg raise angle to determine the degree of improvement in patients. Seven randomized controlled trials were included in the analysis. The findings indicated that NM interventions in patients with LBP were more effective than control groups in improving Visual Analog Scale scores (mean difference = 0.62, 95% CI…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
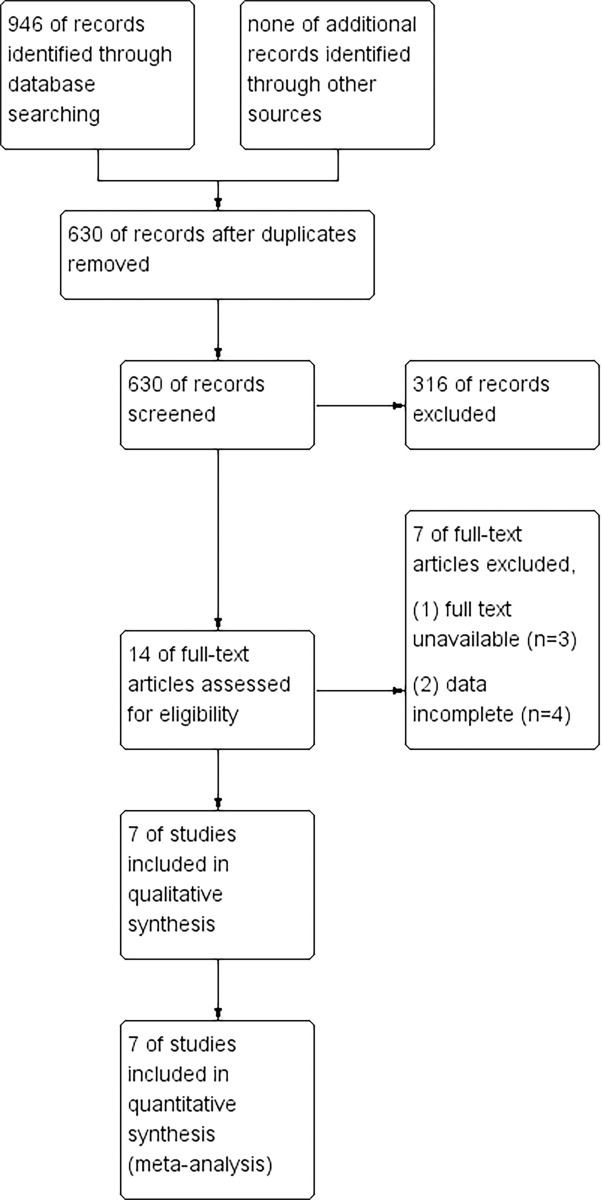 Fig 1
Fig 1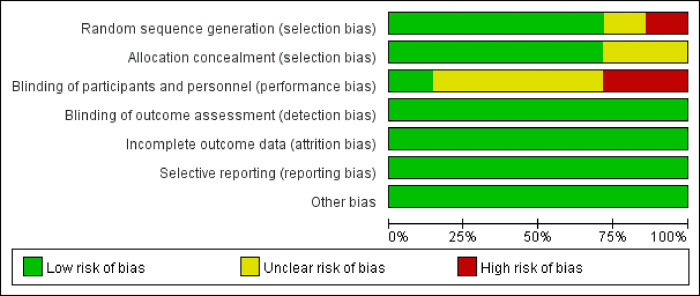 Fig 2
Fig 2 Fig 3
Fig 3 Fig 4
Fig 4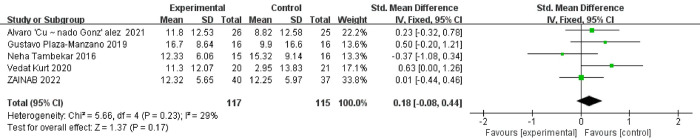 Fig 5
Fig 5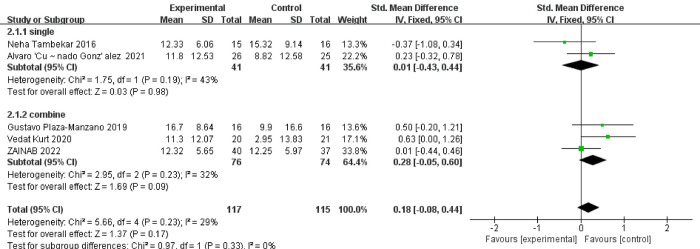 Fig 6
Fig 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal pain and rehabilitation · Spine and Intervertebral Disc Pathology · Myofascial pain diagnosis and treatment
Introduction
Low back pain (LBP), one of the main causes of disability [1], can be attributed to a variety of factors, including psychological and physical [2]. LBP is typically associated with degenerative lesions caused by various factors, such as sprains, sciatica, scoliosis, slipped discs, and radiculopathy and so forth [3]. Not only does it put economic pressure on the patients themselves [4], but it also adds a potential burden on society [5]. Research findings suggest that a substantial proportion of the adult population, potentially up to 84%, have encountered episodes of LBP at some point in their lifespan. Furthermore, these investigations elucidate a tendency for the expenditure on LBP treatment to increase progressively over time [6].
Exercise is often considered the best treatment for LBP [7]. A study documented the establishment of the Chronic Pain Management Guidelines Committee, tasked with addressing chronic pain. The committee observed that the potential adverse effects associated with the utilization of opioids and cannabinoids might surpass the therapeutic advantages across a majority, if not all, of the examined conditions. Consequently, pharmacotherapy might not represent the optimal approach. Furthermore, the committee advocates for exercise as the primary treatment in the management of chronic osteoarthritis and low back pain [8]. However, it is worth noting that medication is currently the preferred option for doctors [9]. Although medication, exercise therapy, and physical factor therapy are commonly used in clinical practice [10], there is an ongoing search for a more cost-effective treatment for LBP. Researchers have found that neuromobilization (NM) shows promise in relieving LBP [11]. NM is an intervention that aims to restore homeostasis of the nervous system or its surrounding structures through manipulation or exercise [12], it involves various techniques, including tension techniques and slider techniques [13]. Several studies have shown that the use of NM in the treatment of neurological diseases can improve joint range of motion better than other techniques in the long term [14]. NM can be applied to adjacent structures, and may through mechanical mechanism to improve symptoms including relieve pain, improve the disabled, reduce edema, and so forth [12].
Although NM is considered an effective treatment for LBP, previous clinical studies have shown inconsistent results. Some studies have shown that NM can significantly reduce the symptoms of LBP [15, 16], while others have failed to find similar positive effects [17]. Therefore, the main objective of this study is to analyze the existing evidence on the effectiveness of NM for the improvement of the syndromes (pain, disability, etc.) of LBP.
1 Materials and methods
1.1 Literature search strategy
This study has been registered with PROSPERO (CRD42023414200). Two researchers independently searched for randomized controlled trial articles published in the following databases: MEDLINE, Embase, Cochrane Library, PubMed, and Web of science [18]. Used 3 sets of keywords: (1) Random, control, Randomized control; (2) neuromobilization, Nerve mobilization, neural mobilization, NM; (3) Mechanical Low Back Pain, Lower back pain, Lumbago, LBP, low back pain. The search period and scope of this study included the period from the creation of the database until December 8, 2023. An example of the search in PubMed can be seen in supplementary material (S1 Checklist).
1.2 Inclusion and exclusion criteria
1.2.1 Inclusion criteria
The literature cited includes randomized controlled trials (RCTS). The subjects were LBP patients who received NM or NM combined with other treatment techniques. In addition, the literature included in this study should be in English. Evaluation measures for inclusion should include the Visual Analogue Scale (VAS) for pain intensity assessment or the Oswestry Disability Index (ODI) for functional impairment or the Straight Leg Raised (SLR) test for lumbar mobility and potential nerve root involvement.
VAS scale is a scale used to assess pain, usually on a scale of 1–10, with a lower score indicating less pain intensity, and conversely, a higher score indicating greater pain intensity [19]; ODI scale is a scale used to assess dysfunction and typically has 10 questions, each corresponding to a score of 0–5 on a 50-point scale, with a lower score representing better functioning and, conversely, a higher score representing a higher degree of dysfunction [20]. The straight leg raise is often used to check the patient’s sciatic nerve, when patients supine leg lifts, along with the rising of the leg Angle, such as patients with sciatic nerve problems, can appear the numbing pain (usually within 70°) [21].
1.2.2 Exclusion criteria
The criteria for excluding articles were non-English language, or the experimental data were not available.
1.3 Literature screening and data extraction
The literature retrieved from the database was amassed by two researchers employing EndNote X9 software. Initially, a process of duplicate identification was undertaken, followed by a comprehensive screening to ascertain the inclusion of pertinent literature. The final phase entailed meticulous data extraction from the selected literature, encompassing key details such as authorship, publication date, gender distribution, sample size, interventions employed, duration of interventions, and evaluation criteria. In the whole process, there are X.C, Z.W involved, if there is any disagreement about the same literature, the Q.C researcher acts as a mediator and makes the final decision [22].
1.4 Study quality evaluation and risk of bias assessment
The screened literature underwent rigorous assessment for quality and bias utilizing the Cochrane Library handbook tool. Six key domains were scrutinized, encompassing the random assignment sequence, concealed assignment scheme, blinding procedures, management of incomplete outcome data, selective reporting of results, and identification of any other potential biases, evaluation process is consistent with 1.3 [2].
1.5 Missing data processing
Incomplete or missing data within the literature significantly influenced research outcomes, underscoring the pivotal role of maintaining data integrity to enhance the reliability of research findings. In instances where data were deficient or incomplete, researchers prioritized strategies to mitigate these limitations. This involved potential outreach to authors via email or telephone during the data extraction phase to procure the absent information. However, in cases where contact with authors proved unfeasible or relevant data remained inaccessible, alternative methodologies were implemented. For instance, when standard deviations were absent from the literature, researchers resorted to utilizing analogous standard deviations from comparable studies or employed statistical methodologies to infer or interpolate missing values [23].
1.6 Bias report
If the number of included articles exceeded 10, publication bias would have been assessed using a funnel plot [24].
1.7 Data analysis
The data extracted from the encompassed literature underwent statistical scrutiny employing RveMan 5.4, a software resource facilitated by the Cochrane website. For continuous variables, statistical analyses were executed utilizing the mean difference (MD) alongside its corresponding 95% confidence interval (CI). For MD and standard deviation (SD) data extraction, this study was guided by the Cochrane Handbook of Systematic Reviews [25]. Heterogeneity was evaluated through the I^2^ statistic and chi-squared tests. Elevated I^2^ values suggested considerable heterogeneity across the included studies. Typically, if the number of studies exceeded five (n>5) and the I^2^ value surpassed 50%, a random-effects model was selected for the analysis. Conversely, when the number of studies amounted to five or fewer (n≤5), a fixed-effects model was applied. The statistical significance of the final outcomes was determined if the p-value fell below 0.05. However, in scenarios characterized by statistical heterogeneity between effect sizes, the appropriateness of the fixed-effect model was deemed inadequate. In such instances, where true homogeneity could not be presumed, the consideration of a random-effects model was warranted [26, 27]. In Meta analysis, if the number is too little, it is difficult to find the reasons of the asymmetric. Because too little number included in this study (< 10), so there is no bias assessment.
2 Results
2.1 Search result
As depicted in Fig 1, the initial stage of the study involved retrieving a total of 946 articles through the database search, with no additional literature acquired through alternative channels. Following this, a rigorous process of duplicate identification led to the removal of 316 redundant articles, thereby yielding a corpus of 630 unique articles. Subsequent screening of titles and abstracts resulted in the selection of 14 papers based on predefined inclusion and exclusion criteria. These selected papers underwent thorough evaluation through examination of their full text, culminating in the inclusion and analysis of 7 papers for data extraction purposes.
Flow chart.Note: MEDLINE (99), PubMed (139), Web of science (254), Cochrane (264), Embase (190).
2.2 Basic characteristics of the literature
Seven papers were screened according to the inclusion and exclusion criteria [17, 28–33], a total of 288 subjects were included, and the publication period of the included literature was 2012–2022. In the study, the experimental group received NM and combined protocols as the primary intervention. On the other hand, the control group was treated with either conventional treatment protocols or a placebo intervention. The basic information of literature is shown in Table 1.
Table 1: Basic information.
2.3 Evaluation of the quality of the included literature and risk bias assessment
Quality and risk of bias were meticulously evaluated for the seven included articles based on Cochrane criteria. The assessment revealed that the majority of the studies demonstrated satisfactory results in terms of bias, with most indicating low risk across various domains such as random assignment sequence, concealed assignment scheme, incomplete outcome data, selective reporting of results, and identification of potential biases. However, shortcomings were observed, particularly in the domain of blinding. Notably, two studies lacked pertinent information regarding blinding procedures, suggesting a potential high risk of bias and relatively lower quality. Additionally, four studies were noted to involve either single blinding or unclear reporting in their narratives, thereby warranting a medium quality rating. Furthermore, in the section pertaining to randomization, one study failed to specify the method of assignment, indicating a higher risk of bias and diminished quality. These findings are visually depicted in Fig 2.
Quality and risk bias assessment.
2.4 Meta-analysis results
2.4.1 Visual analog scale score
Three studies reported effects of NM on pain through the use of VAS [17, 29, 31]. The test of heterogeneity yielded the following results: χ^2^ = 0.82, I^2^ = 0%, P = 0.66, using a fixed-effects model. The meta-analysis results demonstrated a mean difference (MD) of 0.62, with a 95% confidence interval (CI) of (0.03, 1.21), and a corresponding p-value of 0.04. These findings indicate statistical significance and suggest that the improvement in VAS scores with NM was superior to that of the control group. Fig 3.
Comparison of VAS scores between experimental and control groups.
2.4.2 Oswestry disability index score
Three studies reported effects of NM on disability through the use of ODI [28, 30, 31]. The test of heterogeneity revealed the following results: χ^2^ = 0.46, I^2^ = 0%, P = 0.79, using a fixed effects model. The meta-analysis results indicated a mean difference (MD) of 7.54, with a 95% confidence interval (CI) of (4.98, 10.10), and a p-value less than 0.00001. These findings demonstrate statistical significance, suggesting that NM is superior to the control group in terms of improving ODI scores. Fig 4.
Comparison of ODI scores between experimental and control groups.
2.4.3 Degree of straight leg raise
Three studies have reported the effect of NM on SLR by using straight leg elevation after pain occurs at an angle [17, 29, 31–33]. The test for heterogeneity yielded the following results: χ^2^ = 5.66, I^2^ = 29%, P = 0.23, using a fixed effects model. The meta-analysis results indicated a mean difference (MD) of 0.18, with a 95% confidence interval (CI) of (-0.08, 0.44), and a p-value of 0.17. These results were not statistically significant, suggesting that there was no significant difference between NM and the control group in terms of the SLR improvement. Fig 5.
Comparison of degree of SLR between experimental and control groups.
2.5 Subgroup analysis
Although the above experimental results concluded that there was no significant difference in SLR improvement between the NM technology group and the control group, the included literature showed that the combination of NM technology and other technologies improved the SLR level. Considering this problem and the reasons for the heterogeneity, a subgroup analysis was performed. Sources of heterogeneity in this study include diverse populations, interventions, publication bias, and study design and methodological quality. For example, the inconsistent duration and frequency of intervention, the inconsistent intervention means, and the inconsistent level of interveners may lead to certain bias in the outcome indicators of different literatures, thus affecting the results of this study. The meta-analytical outcomes revealed the following: Within the NM-only subgroup, the obtained p-value of 0.98 indicated a lack of statistical significance. This suggests an absence of notable disparity in the efficacy of NM as a standalone intervention regarding SLR improvement. Similarly, within the combined treatment subgroup, the computed p-value of 0.09 also pointed towards a lack of statistical significance. This implies a comparable efficacy between the combined treatment regimen and NM-only intervention concerning their impact on SLR improvement. The graphical representation of these findings is presented in Fig 6.
Comparison of SLR subgroup analysis between experimental and control groups.Note: Single indicates nerve fixation only, combined indicates nerve fixation in combination with other treatments.
3 Discussion
3.1 Effect on pain
The meta-analysis of this study showed that the use of NM could effectively improve pain in patients with low back pain (P < 0.05). A study conducted by Kurt V et al. [31] supported this finding, demonstrating that the addition of NM to conventional treatment resulted in pain reduction and improved motor function among patients. Peacock M et al. [11] suggest that while NM is effective in reducing pain, its effects may be short-lived, and the long-term effectiveness remains uncertain. Several factors could potentially contribute to the variability in the long-term effectiveness of NM. These factors may include the strength and technique of the therapist’s manipulation, the type of manipulation employed, the duration of treatment, the patient’s tolerance, the duration of illness, and the severity of the disease. However, it is evident that NM plays a role in relieving nerve compression and improving nerve function, ultimately leading to the alleviation of symptoms [34]. Pain relief through NM may be attributed to the gate control theory. According to this theory, the activation of fine fibers (C-fibers) leads to the transmission of pain signals, while the activation of coarse fibers (A-β fibers) inhibits the activity of neurons, thereby reducing signal transmission and effectively closing the "gate" for pain information to reach the brain. This mechanism ultimately results in pain reduction [35–37].
NM distinctive slide and tension techniques have been shown to effectively enhance the flexibility of the musculoskeletal and peripheral nervous systems. These techniques can contribute to reducing the cross-sectional area of the nerves, minimizing peripheral and central sensory impairments. Furthermore, NM can help reduce the sensitivity of individuals with nervous system disorders to mechanical pressure and light touch [38]; NM can contribute to reducing neurogenic inflammation by diminishing the generation of anti-mechanical impulses in C fibers. By doing so, it reduces the input of sensory signals to the dorsal horn of the spinal cord [16]. When sensory information is insufficient, nerve impulses may not reach the pain threshold, resulting in the absence of pain sensation [36].
3.2 Effect on dysfunction and disability
This study found that NM could effectively reduce ODI scores [28, 30, 31], but it doesn’t necessarily improve quality of life. In a study conducted by Plaza Manzano et al. [32] on NM for lumbar spine disease, it was found that the addition of NM therapy to motor control did not result in a statistically significant change in patients’ function, as measured by the Rowland-Morris Disability Questionnaire (PMDQ), after a period of 2 months. As in the study of Kurt, V et al. [31] treatment with NM does not effectively improve the gait of patients, which is equivalent to failing to improve the disability level of patients. Dysfunction and its impact on quality of life are not always directly related. It is possible for dysfunction to occur without significantly affecting quality of life, or vice versa. NM, through its stimulation of nerves and soft tissues, promotion of blood circulation and material metabolism, and regulation of the nervous and immune systems, can improve the physical and psychological well-being of patients with LBP.
3.3 Effect on straight leg raise
The studies that participated in this subgroup analysis some suggest that NM could improve SLR in patients, but when these studies were included in the meta-analysis, results using NM alone (95%CI = -0.43 ~ 0.44, P = 0.98) were not found to improve SLR in patients and the results of using NM in combination with other treatments were contrary to the results of the investigators (95%CI = -0.05–0.60, P = 0.09), which may be the cause of insufficient sample size or large differences in sample size. Although a single study may show significant differences, when they are summarized, the combined results may no longer show significant differences due to heterogeneity, and there may be differences in the design, measurement methods and population characteristics of different studies due to methodological reasons. These differences may affect the consistency of the findings. Therefore, the effect of NM on SLR cannot be determined in this study, which needs to be further explored in prospective trials, although there are a few studies that suggest that NM is helpful in improving SLR. The SLR test is commonly utilized to evaluate the flexibility of the nerve structures in the lower limb [39]. The coordination and cooperation between the nervous system and the musculofemoral system play a crucial role in movement. The nervous system assists in generating muscle strength, while also influencing muscle balance and stability [40]. Interestingly, NM demonstrated comparable or even superior effectiveness in improving SLR levels when compared to other treatments. Three literature reports in the study [17, 29, 33], NM has been found to provide short-term improvements in SLR levels. However, its long-term efficacy is limited, and there is no significant advantage observed when combined with other treatment options. In a randomized controlled trial conducted by Kiran Satpute, clinically meaningful improvements were observed in SLR outcomes in the treatment of patients with radicular LBP. This improvement was achieved through two interventions over a 6-week period, involving spinal activity and leg exercises. Furthermore, the study demonstrated the long-term effects of these interventions [41]. The effectiveness of NM in improving outcomes may be attributed to the specific techniques used during treatment. Nerve Sliding can result in a bias of the nerve within adjacent tissues, while nerve tension may increase nerve pressure [42].
As mentioned above, although there are studies that believe that NM can improve the degree of SLR, there are also studies that believe that it is ineffective [31]. After analysis, this study found that the effectiveness is doubtful (P > 0.05), so it is not possible to determine its effectiveness at present, and more high-quality randomized controlled trial studies are needed to verify it in the future.
4 Limitations
There is a limited number of high-quality randomized controlled studies available on NM for the treatment of LBP, resulting in a smaller number of included literatures, this may compromise the reliability and generality of the results. Furthermore, some of the included literature may have a higher risk of bias. Additionally, most of the studies have small sample sizes and predominantly rely on subjective evaluation indicators such as scales, which may have reduced the statistical power of the experiments and increased the instability of the results. In the study of subjective evaluation indicators such as scale, there may be problems such as inconsistent evaluation criteria and subjective bias, which will affect the evaluation results. The lack of objective instruments and detailed experimental procedures is also notable, and some studies are not double-blind, which may introduce potential bias. Moreover, this study did not analyze factors such as safety, type of LBP, gender, and treatment duration. It is recommended that future researchers strive to enlarge the sample size to increase the representativeness and credibility of the study; Reduce the reliance on subjective evaluation and adopt objective quantitative methods as much as possible; At the same time, we advocate the pre-registration research plan, which is conducive to the repeatability of the experiment and improve the authenticity and reliability of the experiment.
5 Conclusions
NM demonstrated effectiveness in improving VAS and ODI outcomes in patients with LBP, but SLR outcomes are still uncertain and until more high-quality studies are included, the effectiveness of NM for SLR remains unknown.
Supporting information
S1 ChecklistSearch formula.Note: PubMed search formula.(PDF)
S1 Fig(TIF)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Coulombe BJ, Games KE, Neil ER, Eberman LE. Core Stability Exercise Versus General Exercise for Chronic Low Back Pain. J Athl Train. 2017;52(1):71–2. Epub 2016/11/17. doi: 10.4085/1062-6050-51.11.16 ; Pub Med Central PMCID: PMC 5293521.27849389 PMC 5293521 · doi ↗ · pubmed ↗
- 2Hayden JA, Ellis J, Ogilvie R, Malmivaara A, van Tulder MW. Exercise therapy for chronic low back pain. Cochrane Database Syst Rev. 2021;9(9):CD 009790. Epub 2021/09/29. doi: 10.1002/14651858.CD 009790.pub 2 ; Pub Med Central PMCID: PMC 8477273.34580864 PMC 8477273 · doi ↗ · pubmed ↗
- 3Hauser RA, Matias D, Woznica D, Rawlings B, Woldin BA. Lumbar instability as an etiology of low back pain and its treatment by prolotherapy: A review. J Back Musculoskelet Rehabil. 2022;35(4):701–12. Epub 2021/12/28. doi: 10.3233/BMR-210097 ; Pub Med Central PMCID: PMC 9398090.34957989 PMC 9398090 · doi ↗ · pubmed ↗
- 4Barrey CY, Le Huec JC, French Society for Spine S. Chronic low back pain: Relevance of a new classification based on the injury pattern. Orthop Traumatol Surg Res. 2019;105(2):339–46. Epub 2019/02/23. doi: 10.1016/j.otsr.2018.11.021 .30792166 · doi ↗ · pubmed ↗
- 5Corp N, Mansell G, Stynes S, Wynne-Jones G, Morso L, Hill JC, et al. Evidence-based treatment recommendations for neck and low back pain across Europe: A systematic review of guidelines. Eur J Pain. 2021;25(2):275–95. Epub 2020/10/17. doi: 10.1002/ejp.1679 ; Pub Med Central PMCID: PMC 7839780.33064878 PMC 7839780 · doi ↗ · pubmed ↗
- 6Pangarkar SS, Kang DG, Sandbrink F, Bevevino A, Tillisch K, Konitzer L, et al. VA/Do D Clinical Practice Guideline: Diagnosis and Treatment of Low Back Pain. J Gen Intern Med. 2019;34(11):2620–9. Epub 2019/09/19. doi: 10.1007/s 11606-019-05086-4 ; Pub Med Central PMCID: PMC 6848394.31529375 PMC 6848394 · doi ↗ · pubmed ↗
- 7Wang XQ, Wang YL, Witchalls J, Han J, Zhang ZJ, Page P, et al. Physical therapy for acute and sub-acute low back pain: A systematic review and expert consensus. Clin Rehabil. 2024:2692155241229398. Epub 2024/02/06. doi: 10.1177/02692155241229398 .38317586 · doi ↗ · pubmed ↗
- 8Korownyk CS, Montgomery L, Young J, Moore S, Singer AG, Mac Dougall P, et al. PEER simplified chronic pain guideline: Management of chronic low back, osteoarthritic, and neuropathic pain in primary care. Can Fam Physician. 2022;68(3):179–90. Epub 2022/03/17. doi: 10.46747/cfp.6803179 ; Pub Med Central PMCID: PMC 9833192.35292455 PMC 9833192 · doi ↗ · pubmed ↗