Is Extracorporeal Membrane Oxygenation a Panacea?
Selen Karaoğlanoğlu, Metin Akgün

TL;DR
This paper reviews ECMO's role in critical care, highlighting its life-saving potential and the need for careful patient selection.
Contribution
The paper provides an updated overview of ECMO applications and patient selection criteria post-pandemic.
Findings
ECMO serves as a life-support technique for severe cardiac or respiratory failure.
Veno-arterial and veno-venous ECMO have distinct roles in patient care.
ECMO requires careful evaluation due to its cost and resource demands.
Abstract
Extracorporeal membrane oxygenation (ECMO) has emerged as a vital life-support technique in critical care medicine, providing temporary circulatory and/or respiratory support for patients with severe cardiac or respiratory failure unresponsive to conventional therapies. This review aims to outline the importance of ECMO and provide a comprehensive overview of its main applications. Two primary types of ECMO, veno-arterial extracorporeal membrane oxygenation and veno-venous extracorporeal membrane oxygenation, serve distinct functions in supporting patients with cardiac or pulmonary dysfunction, respectively. While ECMO offers life-saving potential, its utilization requires careful consideration due to its cost and resource-intensiveness. Thus, a comprehensive evaluation of an individual patient’s clinical condition, prognosis, and potential for recovery is crucial. Ongoing research and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1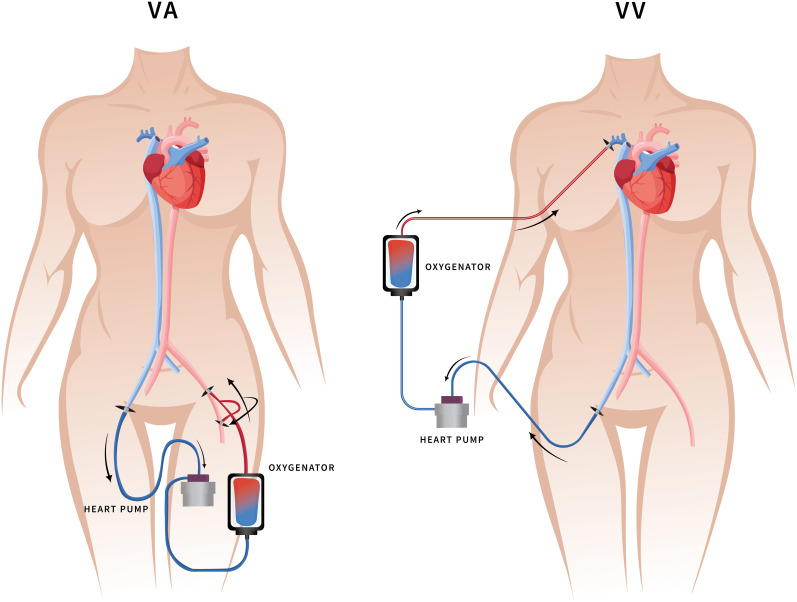 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMechanical Circulatory Support Devices · Cardiac Arrest and Resuscitation · Cardiac Structural Anomalies and Repair
Introduction
Mechanical cardiopulmonary support is commonly employed during both intraoperative and intensive care settings, particularly in cardiac surgery. However, sometimes cardiopulmonary support may be required in the intensive care unit. Extracorporeal membrane oxygenation (ECMO) or extracorporeal lung support (ECLS) serves as a life support system for providing prolonged cardiopulmonary assistance. Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) and veno-venous extracorporeal membrane oxygenation (VV-ECMO) are 2 primary types of ECMO, offering respiratory support, with VA-ECMO additionally providing hemodynamic support. Since its inception in 1970, the ECMO experience has progressively expanded, gaining significant recognition.^1,2^ In this review, we comprehensively discuss the clinical advantages of ECMO, patient selection criteria, indications, contraindications, and its specific role in managing respiratory failure associated with viral pneumonia, which has become increasingly prevalent during the coronavirus disease 2019 (COVID-19) pandemic.^3^ Key studies are summarized in Table 1, and by incorporating an extensive review of available literature, our aim is to provide valuable insights and guidance for clinical practice in this evolving field.
Notably, neonates and children generally exhibit high survival rates following ECMO support for respiratory failure.^4^ Nevertheless, accurately estimating patient survival poses a challenge, as the mortality risk associated with this procedure is estimated to be approximately 50%. Typically, ECLS is considered when the risk of mortality reaches around 80%. To ensure a precise evaluation, the severity of the disease, likelihood of death, and organ failure are meticulously assessed, considering patient age and other factors.^5^ Complications may arise, some of which may result in significant morbidity. Extracorporeal membrane oxygenation-associated complications can be categorized as either device related, encompassing issues such as oxygenator malfunction, pump failure, circulatory blockages, and cannulation problems, or physiological, including bleeding, hemolysis, and infection.^6-9^ Initiation of ECMO triggers an inflammatory response akin to systemic inflammatory response syndrome.^10^ The interaction between patient blood and the extracorporeal space initiates coagulation and inflammatory cascades, rapidly elevating proinflammatory cytokine levels and activating leukocytes.^11-14^ This innate immune response ultimately leads to endothelial damage, impaired microcirculation, and subsequent end-organ dysfunction.^10-15^ Despite the escalating use of ECMO, our current understanding of the elicited inflammatory response remains limited. Patients supported with ECMO frequently exhibit an inflammatory response; however, a comprehensive understanding of the severe patient reactions to inflammation and their clinical trajectory is currently lacking. Further insight into this complex phenomenon is necessary to explore potential treatments and novel therapeutic strategies.
Techniques of Extracorporeal Membrane Oxygenation
Two ECMO techniques are commonly used (Figure 1):
Veno-venous ECMO: It provides respiratory support by removing deoxygenated blood from a vein, oxygenating it, and returning it to a vein. This configuration bypasses the heart and supports the lungs.^5^
- Cannulation: In VV-ECMO, 2 cannulas are typically inserted into a large central vein, such as the femoral vein or internal jugular vein. The venous cannula drains deoxygenated blood from the patient, which is then advanced into the right atrium or superior vena cava. Oxygenated blood is returned to the patient via a second cannula, usually placed in a central vein, such as the internal jugular vein or subclavian vein.
- Circuit: The cannulas are connected to the ECMO circuit, which includes a pump, a membrane oxygenator, and tubing. The pump propels blood through the circuit, while the membrane oxygenator removes carbon dioxide and adds oxygen. Prior to returning it to the patient, the oxygenated blood is warmed to body temperature. Veno-arterial ECMO: It provides both respiratory and cardiac support by bypassing both the heart and lungs.Cannulation: Similar to VV-ECMO, 2 cannulas are used in VA-ECMO. The arterial cannula is inserted into a large artery, such as the femoral artery, to withdraw deoxygenated blood from the patient. The cannula is advanced to a site distal to the heart. Oxygenated blood is then returned to the patient via a venous cannula, as in VV-ECMO.Circuit: The ECMO circuit for VA-ECMO is similar to VV-ECMO, consisting of a pump, a membrane oxygenator, and tubing. The pump propels blood through the circuit, providing oxygenation and mechanical support to both the heart and lungs. The oxygenated blood is warmed to body temperature and returned to the patient via the venous cannula.^16,17^
Hemostasis of Extracorporeal Membrane Oxygenation
Effective hemostasis management is a crucial aspect of ECMO therapy, as the use of anticoagulation to prevent clot formation within the circuit presents challenges in maintaining hemostasis. Achieving the delicate balance between preventing bleeding and minimizing thrombotic complications remains a constant concern. Close monitoring of coagulation parameters, such as activated clotting time or activated partial thromboplastin time, is essential for guiding anticoagulation therapy and detecting early signs of bleeding or clotting. Collaborative efforts among the ECMO team, hematologists, and other specialists are vital to develop personalized hemostasis management strategies. These strategies may involve adjusting anticoagulation levels, employing antithrombotic agents, and implementing techniques to minimize circuit-related factors that contribute to coagulation activation. The goal is to maintain optimal hemostasis, prevent both bleeding and thrombotic complications, and ultimately improve patient outcomes during ECMO therapy.^18^
Selecting the Perfect Candidate for Extracorporeal Membrane Oxygenation
Extracorporeal membrane oxygenation, a transformative technology with immense potential to save lives, necessitates cautious implementation to prevent additional harm to patients. Integration of ECMO within comprehensive clinical strategies, such as long-term platforms like ventricular assist devices and transplantation, becomes imperative, as it is not a viable standalone solution.^19^ The survival rates for patients who suffer out-of-hospital cardiac arrest (OHCA) remain alarmingly low. However, the use of ECMO in cases of cardiac arrest, known as extracorporeal cardiopulmonary resuscitation (ECPR), has demonstrated promising results in enhancing patient survival while preserving favorable neurological outcomes.^20^ A Danish study revealed a substantial failure rate, with only a minority of patients undergoing ECPR treatment achieving successful outcomes. Factors contributing to the avoidance of ECPR encompass prolonged prehospital low-flow duration, metabolic abnormalities, and diminished end-tidal carbon dioxide (ETCO_2_) levels.^21^
Indications
Patient selection and timing are crucial considerations in ECMO, with mortality rates rising with age and concomitant diseases.^22,23^ The use of scoring systems such as Respiratory ECMO Survival Prediction (RESP) and Murray scores can assist in the assessment. The RESP score predicts survival for ECMO patients, while the Murray score predicts mortality rates in the absence of ECMO. If ECMO is deemed necessary, prompt transfer to a specialized medical facility should be arranged.^24^ Clinical guidelines for Acute Respiratory Distress Syndrome (ARDS) recommend considering ECMO in adult patients with severe ARDS, supported by a moderate level of evidence (GRADE rating 2B). There are many experimental studies in the treatment of ARDS.^25,26^ Patients with severe hypoxemia or hypercapnia who do not respond to conventional lung-protective ventilation or adjunctive therapies should be referred to experts for guidance on ECMO indications and patient transport.^27^ Survival rates range from 50% to 71%.^28-33^ The CESAR study compared ECMO with standard ventilatory support in severe acute respiratory failure, revealing significantly higher 6-month survival without sequelae (63% vs. 47%) with ECMO, despite certain methodological limitations, including the study being conducted at a single center with specialized expertise in ECMO use.^34^ In the EOLIA study, early VV-ECMO versus delayed intervention in ARDS showed no statistically significant difference in 60-day mortality rates.^35^ While the appropriateness of ECMO in ARDS remains debated, studies suggest potential benefits despite challenges in conducting controlled studies in critically ill patients.^34-36^ Veno-venous ECMO is recommended for adult patients with severe ARDS due to sepsis and failed mechanical ventilation, although quality of the evidence is low. Studies in England^37^ and France^38^ reported varied mortality rates for severe acute respiratory failure associated with influenza H1N1 patients transferred to ECMO centers. Extracorporeal membrane oxygenation may serve as a bridge to transplantation, benefiting some patients with chronic respiratory failure from interstitial lung disease.^39^ Evidence supporting VA-ECMO use for circulatory assistance in cardiogenic shock remains inadequate, as the ECMO-CS trial found no significant differences in clinical outcomes between immediate initiation and a conservative approach with delayed use.^40^
Recent randomized trials suggest potential benefits of ECPR, yet evidence certainty is modest, and patients’ selection criteria remain undetermined.^41^ Extracorporeal cardiopulmonary resuscitation in intra-hospital cardiac arrest (IHCA) shows low survival rates but favorable neurological outcomes at 1 year.^42^ Variables such as age, time of day, initial rhythm, medical history of renal failure, patient type (cardiac versus noncardiac and medical versus surgical), and duration of cardiac arrest influence IHCA causes and survival rates.^43^ Extracorporeal cardiopulmonary resuscitation is more effective in OHCA,^44^ with early chest compression initiation improving pre-discharge rates.^45^ Implementing transportable VA-ECMO programs in hospitals allows treatment of critically ill patients with comparable survival rates.^46^ Predictors of survival in OHCA patients include initial cardiac rhythm, short symptom onset-to-arrival duration, and age below 75 years.^47-49^ Out-of-hospital ECPR has been shown to be an effective^50^ and economically acceptable pacing strategy.^51^ Accidental cardiac arrest (AHCA) is another indication for ECLS.^52-56^ Extracorporeal membrane oxygenation improves outcomes in AHCA cases, especially in acute hypothermia-induced cardiac arrest.^57^ Veno-arterial ECMO and endovascular therapy are rescue strategies for massive pulmonary embolism (PE) when thrombolysis is contraindicated, potentially aiding resuscitation in high-risk PE-related cardiac arrest.^58,59^ Immediate initiation of ECMO can potentially aid in resuscitation of patients with cardiac arrest due to high-risk PE.^60,61^ Veno-arterial ECMO and endovascular therapy are rescue strategies for massive PE when thrombolysis is contraindicated, potentially aiding resuscitation in high-risk PE-related cardiac arrest (57, 58). Successful VA-ECMO use has been reported in amniotic fluid embolism cases.^62,63^ Extracorporeal cardiopulmonary resuscitation indications in cancer patients are unclear, but understanding IHCA outcomes in this population is essential due to the incidence of cancer and improved survival rates.^64^ Veno-arterial ECMO is a suitable treatment option for poisoning cases complicated by refractory cardiogenic shock or cardiac arrest, offering high survival rates with low complications.^65^ Extracorporeal membrane oxygenation may be indicated in severe status asthmaticus,^66^ pheochromocytoma-induced cardiomyopathy,^67,68^ fulminant myocarditis,^69^ ANCA-associated vasculitis,^70^ and refractory thyroid storm.^71^
Contraindications
Relative contraindications to ECMO include age older than 65 years, body mass index greater than 40, suppressed immunity, lack of a relative who can make medical decisions, and severe chronic systolic heart failure. There are certain contraindications to ECMO that should be considered, such as disseminated malignancy, severe deconditioning, uncontrolled bleeding, inability to receive blood products, ongoing CPR, third-stage chronic renal disease, severe peripheral vascular disease, uncontrolled diabetes with chronic end-organ dysfunction, cirrhosis, advanced lung disease, dementia, other preexisting life-limiting conditions, a clinical frailty scale of category 3 or higher, underlying neurologic disease affecting rehabilitation potential, severe multiorgan failure, and advanced age.^5,72,73^
Complications of Extracorporeal Membrane Oxygenation
Complications of ECMO are significant, as observed in an analysis of the Extracorporeal Life Support Organization (ELSO) involving 7579 VV-ECMO patients. Among them, 40.2% experienced bleeding and thrombotic events, with thrombosis in the ECMO circuit being predominant. Hospitalized patients had a reported mortality rate of 34.9%. Thrombotic events (adjusted OR 1.23; 95% CI, 1.08-1.41; P < .01) and bleeding events (adjusted OR 1.69, 95% CI, 1.49-1.93; P < .01) were differentially associated with in-hospital mortality. Ischemic stroke, intracranial hemorrhage, pulmonary hemorrhage, and gastrointestinal hemorrhage were strongly linked to mortality (adjusted ORs ranging from 2.02 to 5.71, all P < .01). Bleeding and thrombosis were associated with prolonged ECMO duration, younger age, elevated pH levels, and earlier years of support.^74^ Disseminated intravascular coagulation has been reported in adult ECMO patients, often related to preexisting conditions such as liver failure, poor anticoagulation mechanisms, and increased fibrinolysis.^75^
Extracorporeal Membrane Oxygenation and Coronavirus Disease 2019
In March 2020, the World Health Organization (WHO) declared the COVID-19 pandemic, which has had a widespread global impact, affecting over 180 million people and resulting in approximately 6 million deaths.^76-79^ During the pandemic, many studies were conducted to early determine the prognosis and intensive care needs of patients.^80-89^ In response to the escalating pandemic, ECMO use has substantially increased. As of the time of writing this review, approximately 6390 COVID-19 patients were reported to have received ECMO assistance.^90^ Guidelines from the Chinese National Health Commission recommended the use of ECMO in the prone position when necessary and respiratory support for the treatment of severe and critically ill patients with lung healing status.^91^ Transitional guidelines by ELSO for COVID-19 state that as the burden of disease increases, ECMO capacity will expand to benefit those who can regain an acceptable quality of life. In regions with crowded hospitals, early transfer of appropriate ECMO candidates, particularly young individuals with single organ failure and no preexisting health conditions, to ECMO centers is prudent. Specific criteria, such as the PaO_2_/FiO_2_ ratio, pH level, and PaCO_2_ values, help determine ECMO indications.^92^ Extracorporeal membrane oxygenation may also be indicated for COVID-19-related cardiogenic shock and refractory cardiac arrest due to myocarditis.^93^ In cases of refractory cardiogenic shock characterized by persistent tissue hypoperfusion and inadequate cardiac function, the timely initiation of VA-ECMO before multiorgan failure occurs is recommended. The need for VA-ECMO is generally uncommon but may be considered as an adjunct treatment for failed cardiogenic/obstructive shock in patients with ARDS, acute stress/septic cardiomyopathy, or in cases of massive PE.^92^ A systematic review examining the use of mechanical circulatory support (MCS) in COVID-19 patients revealed that out of 4218 individuals, 92.7% received VV-ECLS, 4.7% received VA-ECLS and/or Impella, and 2.6% received other forms of ECLS. Conversion from VV-ECLS to MCS was necessary for 3.1% of patients due to heart failure, myocarditis, or myocardial infarction. Survival rates for VV-ECLS and MCS were reported as 54.6% and 28.1%, respectively.^94^ Another study evaluated the effectiveness of the RESP score (Table 2) in predicting in-hospital survival in COVID-19 patients receiving VV-ECMO. However, the exclusive use of the RESP score was deemed insufficient for accurately predicting survival in COVID-19 patients requiring VA-ECMO treatment. Further investigation is needed to determine the most appropriate timing and indication for MCS in COVID-19 patients based on survival reports.^95^ Considering the potential for neurological injury, additional research is necessary to explore neuromonitoring protocols to enhance personalized anticoagulation management and improve survival rates in COVID-19 patients on ECMO.^96^ Given resource limitations, ECMO should be reserved for extremely severe cases of COVID-19 during a global pandemic.^97^ The utility of ECMO should be evaluated based on current circumstances, considering the need for specialized patient care and the capacity to manage a high volume of patients through centralization.^98^
Conclusion
The utilization of VV-ECMO in the adult population has witnessed a significant global increase. Careful patient selection is paramount, ensuring that the etiology of respiratory failure in ARDS is reversible and unresponsive to conventional treatments while also considering formal contraindications to ECMO initiation. Furthermore, patients with irreversible diseases, such as end-stage lung disease, may be considered viable candidates for ECMO therapy, particularly when bridging toward lung transplantation. The employment of ECMO in the management of ARDS patients has demonstrated superior survival rates when compared to patients of similar age and disease severity who did not receive this advanced intervention. Nevertheless, it is noteworthy that the current body of literature addressing the use of VA-ECMO to support COVID-19 patients is sparse, necessitating further investigation to optimize its application and elucidate its potential benefits in this specific context.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hill JD O’Brien TG Murray JJ , et al. Prolonged extracorporeal oxygenation for acute post-traumatic respiratory failure (shock-lung syndrome). Use of the Bramson membrane lung. N Engl J Med. 1972;286(12):629 634. (10.1056/NEJM 197203232861204)5060491 · doi ↗ · pubmed ↗
- 2Lorusso R Whitman G Milojevic M , et al. 2020 EACTS/ELSO/STS/AATS expert consensus on post-cardiotomy extracorporeal life support in adult patients. J Thorac Cardiovasc Surg. 2021;161(4):1287 1331. (10.1016/j.jtcvs.2020.09.045)33039139 · doi ↗ · pubmed ↗
- 3Schmidt M Hajage D Landoll M , et al. Comparative outcomes of extracorporeal membrane oxygenation for COVID-19 delivered in experienced European centres during successive SARS-Co V-2 variant outbreaks (ECMO-SURGES): an international, multicentre, retrospective cohort study. Lancet Respir Med. 2023;11(2):163 175. (10.1016/S 2213-2600(22)00438-6)36640786 PMC 9889098 · doi ↗ · pubmed ↗
- 4Gray BW Haft JW Hirsch JC Annich GM Hirschl RB Bartlett RH . Extracorporeal life support: experience with 2,000 patients. ASAIO J. 2015;61(1):2 7. (10.1097/MAT.0000000000000150)25251585 PMC 4280306 · doi ↗ · pubmed ↗
- 5ELSO Guidelines for Cardiopulmonary Extracorporeal Life Support. Available at: https://www.elso.org.
- 6Kim JH Pieri M Landoni G , et al. Venovenous ECMO treatment, outcomes, and complications in adults according to large case series: a systematic review. Int J Artif Organs. 2021;44(7):481 488. (10.1177/0391398820975408)33259258 · doi ↗ · pubmed ↗
- 7Xiong J Zhang L Bao L . Complications and mortality of venovenous extracorporeal membrane oxygenation in the treatment of neonatal respiratory failure: a systematic review and meta-analysis. BMC Pulm Med. 2020;20(1):124. (10.1186/s 12890-020-1144-8)32380985 PMC 7204219 · doi ↗ · pubmed ↗
- 8Jia D Yang IX Ling RR , et al. Vascular complications of extracorporeal membrane oxygenation: a systematic review and meta-regression analysis. Crit Care Med. 2020;48(12):e 1269 e 1277. (10.1097/CCM.0000000000004688)33105148 · doi ↗ · pubmed ↗