Vertical Fracture of the Medial Malleolus With Concurrent Ipsilateral Achilles Tendon Rupture in a Patient With Progressive Collapsing Foot Deformity: A Rehabilitation Dilemma
Hannah L Morley, Bawan Hama, Gary Hannant

TL;DR
A rare case of a vertical medial malleolus fracture and Achilles tendon rupture in a patient with flatfoot is reported, highlighting the challenges in treatment.
Contribution
This is the first documented case linking a medial malleolus fracture and Achilles tendon rupture with pes planus.
Findings
The patient was treated with surgical fixation of the fracture and functional rehabilitation for the tendon rupture.
The case highlights the lack of consensus on optimal management for this rare injury combination.
The report emphasizes the therapeutic dilemma in treating such complex, concurrent injuries.
Abstract
A male in his 40s presented with a vertical shear type medial malleolar fracture with an ipsilateral Achilles tendon rupture with a pes planovalgus deformity. Both injuries were diagnosed concurrently on presentation. This is a rare injury pattern with no consensus on optimum management. This is the first case report where pes planus is also described alongside the injuries. The medial malleolar fracture was successfully treated surgically with an open reduction and internal fixation (ORIF) with antiglide plating. Following ORIF, the patient underwent functional rehabilitation for the Achilles tendon rupture. The purpose of this case report is to highlight this infrequent injury pattern, which poses a great therapeutic dilemma. The therapeutic considerations regarding surgical and non-surgical approaches to management are thoroughly presented and discussed.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1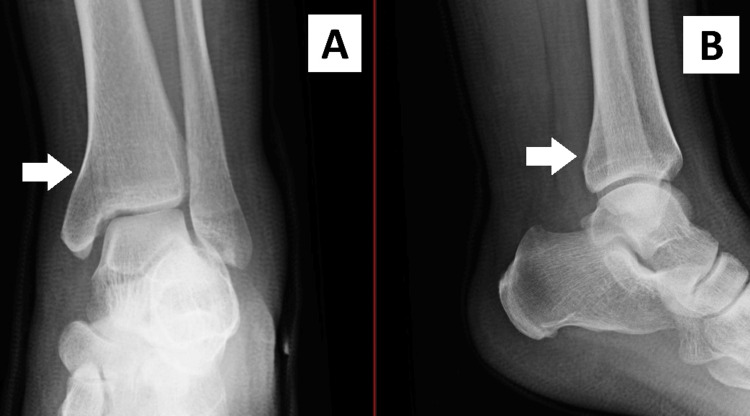 Figure 2
Figure 2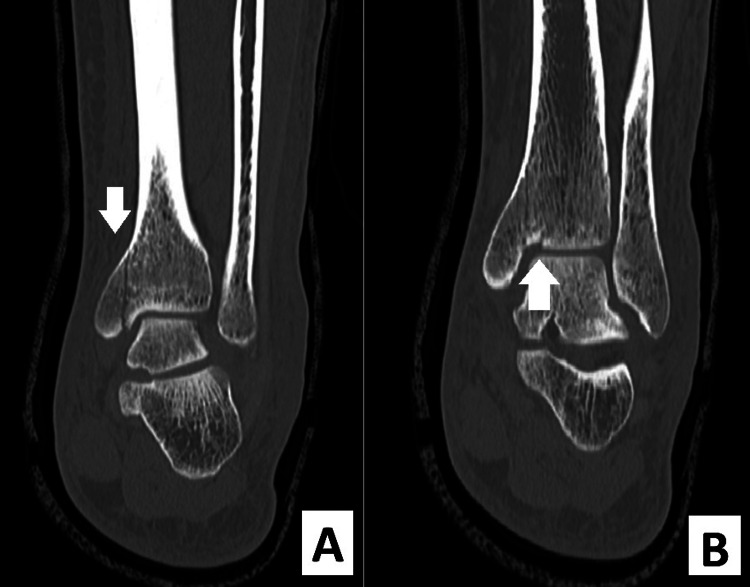 Figure 3
Figure 3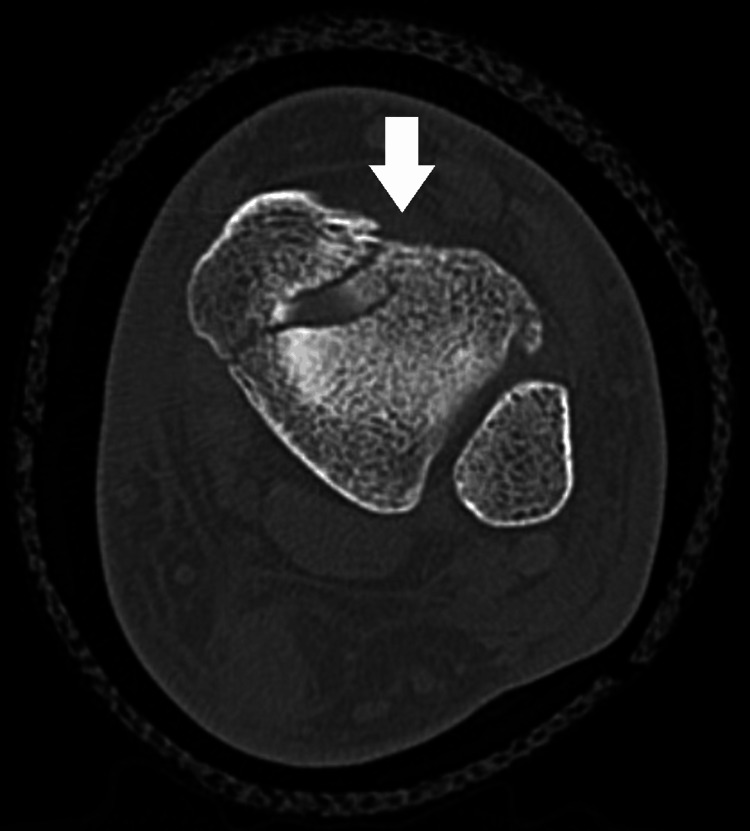 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6 Figure 7
Figure 7| Time in months post-injury | ATRS | EFAS |
| Pre-morbid (patient answered this upon diagnosis of injury) | 100 | 24 |
| 3 | 24 | 2 |
| 8 | 68 | 12 |
| 12 | 84 | 14 |
| Total score available | 100 | 24 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTendon Structure and Treatment · Foot and Ankle Surgery · Sports injuries and prevention
Introduction
Medial malleolus fractures combined with Achilles tendon ruptures are rare entities. There are few, sporadic case reports in the literature [1-7]. There is one published case series dating back to the 1970s detailing this injury pattern in skiers, but otherwise, to the best of our knowledge, no research exists. There is no internationally recognized consensus regarding the optimal treatment of such injury. Indeed, published case reports have either failed to define the management [1], elected to operate on the Achilles rupture but not the medial malleolus [2], or managed the cases non-operatively [3].
Additionally, the surgical planning in some cases is at the surgeon's preference, as delay in diagnosis is a common problem [1,3,5].
It is important to acknowledge the impact of functional rehabilitation on the management of Achilles tendon injuries [8]. First described in the early 1980s, this technique has grown in popularity since several randomized control trials were published in the early 2000s [9,10]. Various case reports regarding this injury pattern were published prior to functional Achilles rehabilitation being in regular use, and this may explain why the Achilles tendon is often reported as being managed operatively.
Case presentation
An otherwise healthy male in his 40s presented to the emergency department following an uncontrolled fall while walking downstairs. He was unable to tolerate weight-bearing on his injured lower extremity. On examination, a palpable gap was present at the Achilles tendon, and a Simmonds-Thompson test was positive. The injury was isolated and closed. The patient had no neurovascular abnormalities on presentation. The patient had bilateral pes planus deformities.
A clinical diagnosis of an Achilles tendon rupture was made. Plain radiographs of the patient's ankle were performed. A medial malleolus fracture on the ipsilateral leg was diagnosed. These radiographs are shown in Figure 1 and Figure 2. The patient was reevaluated in the fracture clinic the following day.
Rotated PA view of the left ankle on admission to the emergency department. The white arrow on the radiograph indicates the medial malleolar fracture.PA: posteroanterior
AP (A) and lateral (B) views demonstrating a nondisplaced medial malleolus fracture of the left ankle. The white arrows indicate the location of the fracture.AP: anteroposterior
An ultrasound demonstrated a full-thickness tear of the Achilles tendon with a gap of approximately 4.5 cm, 3 cm proximal to the insertion. A computed tomography (CT) of the ankle demonstrated a comminuted intra-articular fracture of the left distal tibia through the medial malleolus. There was also a 1-2 mm step at the articular surface of the tibial plafond. This is best visualized in Figure 3, as well as Figure 4. Although comminution was present on the CT, the fracture fragments remained nondisplaced. Furthermore, there was no posterior malleolus fracture or evidence of disruption of the syndesmosis on the CT scan.
Coronal CT views of the left ankle demonstrating the medial malleolar fracture with comminution into the tibial plafond. A and B demonstrate different coronal sections of the CT scan; this illustrates the fracture's relationship with the joint surface. The arrows indicate the location of the fracture.CT: computed tomography
Axial view on CT scan of the medial malleolar fracture with an arrow indicating the location of the fracture.CT: computed tomography
Surgery was performed eight days post-injury to account for soft tissue swelling. The patient was treated with an open reduction and internal fixation (ORIF) of the medial malleolus; this was performed under fluoroscopy and anesthesia. The vertical medial malleolar fracture was fixed with a 2.7 mm four-hole Synthes Variable Angle Cloverleaf Plate [11], in antiglide mode. Once the wounds were closed, the patient was placed in a front slab in equinus in theater to prevent dorsiflexion. Figure 5 demonstrates the intraoperative radiographs.
Intraoperative films demonstrating the antiglide plating.
The patient had functional rehabilitation using a Vacoped boot system [12] at one week postoperatively. Prophylaxis for venous thromboembolism was provided until the foot was in plantigrade. An example of our local functional Achilles rehabilitation protocol can be found in the Appendices [13].
The patient was discharged from face-to-face follow-up at 12 months post-injury and was assessed as being able to perform a single heel raise test prior to discharge and has since returned to manual work. Figure 6 and Figure 7 show the healed fracture on radiographs. We can provide a 24-month follow-up at the time of submission of this article.
Postoperative weight-bearing AP ankle view.AP: anteroposterior, WB: weight-bearing
Weight-bearing lateral view of the ankle.WB: weight-bearing
The patient agreed to have Achilles Tendon Total Rupture Score (ATRS) and European Foot and Ankle Score (EFAS) data collected throughout his care [14,15]. The final ATRS was 84 at 12 months. ATRS has not been validated on patients with concurrent injuries to Achilles tendon ruptures; however, we felt that it was a useful score to use in this case in the absence of another available score. The final EFAS was 12 at 12 months. The change in score is documented in Table 1.
Discussion
Combined Achilles tendon rupture and ankle fractures are rare occurrences. There are several reports of a vertical medial malleolar fracture associated with Achilles injury. Previous papers have hypothesized that such a fracture pattern results from sudden ankle hyperextension or hindfoot inversion [2,3]. Other authors have noted the lack of syndesmotic injury [2,3], which was also the case here.
With regard to foot and ankle morphology, the patient in this case had a pes planovalgus deformity. To the best of our knowledge, there are no published cases of pes planovalgus deformity associated with an Achilles tendon rupture and a concurrent medial malleolar fracture, thus making this case report unique. Indeed, literature relating to Achilles tendon rupture seems to refer to hyperpronation not being a risk factor for Achilles tendon rupture [16]. Indeed, in the current literature, there is a paucity of evidence to support the association of pes planovalgus deformity on any specific injury pattern [17,18].
Surgical consensus in the literature is lacking [1-7]. Lu et al. [5] described a case where the medial malleolus was fixated, and the Achilles rupture was non-operatively managed. This treatment approach is equivalent to our case. However, the Achilles rupture in the case of Lu et al. [5] was only identified following the medial malleolus fixation. In their case, the Achilles tendon rupture was managed non-operatively in a fixed cast, not with functional rehabilitation. We believe our case to be the first to describe the use of functional rehabilitation, as we are unable to find specific functional rehabilitation protocols used in the case reports in our literature review. In our case, the Achilles tendon healed without the need for surgery.
Some authors describe operatively managing both injuries [6,7]. However, these injuries are unlikely to be able to be accessed via the same incision, and therefore, there are additional risks associated with wound complications and damage to surrounding neurovascular structures. We would advocate fixing the medial malleolus to create a stable scaffold to rehabilitate the Achilles tendon. In consideration of future cases where there may be an indication for operative fixation of the Achilles tendon but with concern regarding wound healing, options could include the use of percutaneous Achilles repair or endoscopic flexor hallucis longus transfer [19], although this is yet to be described in relation to this injury pattern.
EFAS in this patient improved, but improvement in ATRS lagged. Although there is some overlap between the two patient-reported outcome measures (PROMS), the ATRS is specific to the Achilles tendon, and the EFAS is more generalized. Indeed, although this patient did manage to return to work, he was still in some pain 12 months following surgery. It is unknown whether the period away from the rehabilitation program affected these scores.
This is the first case report of this injury type to include patient-reported outcome measures (PROMS). We would advocate the use of PROMS to other surgeons dealing with this combination of injuries. This could be facilitated through a centralized database, such as the British Orthopaedic Foot and Ankle Society (BOFAS) registry [20]. An international database in foot and ankle surgery would facilitate further research into the management of these concurrent injuries.
Conclusions
Ipsilateral Achilles tendon rupture with medial malleolar fracture is rare but presents an interesting treatment conundrum. We have demonstrated that a mixed operative and non-operative approach is a viable option, supported by PROMS. Although there is currently no internationally recognized consensus on the management of this unique injury pattern, we present the case that there is no requirement to operate on a ruptured Achilles tendon just because the patient is anesthetized for a concurrent injury. The association between pes planovalgus and this injury pattern is unclear and requires further research. For rarer combination injuries, contributing to registry databases is a useful adjunct to publishing case reports and case series.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Unrecognized Achilles tendon rupture associated with ipsilateral medial malleolar fracture Am J Sports Med Barron JL Yocum LA 629631211993836842810.1177/036354659302100426 · doi ↗ · pubmed ↗
- 2Subcutaneous rupture of the Achilles tendon and ipsilateral fracture of the medial malleolus BMC Musculoskelet Disord Maffulli N Richards PJ 5972006 https://doi.org/10.1186/1471-2474-7-591687252110.1186/1471-2474-7-59PMC 1555578 · doi ↗ · pubmed ↗
- 3Fracture of the ankle associated with rupture of the Achilles tendon: case report and review of the literature J Orthop Trauma Assal M Stern R Peter R 358361162002 https://journals.lww.com/jorthotrauma/abstract/2002/05000/fracture_of_the_ankle_associated_with_rupture_of.13.aspx 1197208210.1097/00005131-200205000-00013 · doi ↗ · pubmed ↗
- 4[Rupture of the achilles tendon and eversion fracture of the inner malleolus - a typically combined injury in alpin skiing (author's translation)] (Article in German)Zentralbl Chir Lugger LJ Margreiter R Glötzer W 132013231021977 https://cir.nii.ac.jp/crid/1570854175279021312602490 · pubmed ↗
- 5Medial malleolus fracture of the ankle combined with rupture of the Achilles tendon J Surg Case Rep Lu J Maruo Holledge M 2016201610.1093/jscr/rjw 062PMC 485298427141047 · doi ↗ · pubmed ↗
- 6High-energy Achilles tendon rupture with associated medial malleolus fracture and traumatic peroneal dislocation: a case report Foot Ankle Spec Bowers M Hunt KJ Metzl J 4384441420213363199010.1177/1938640021997285 · doi ↗ · pubmed ↗
- 7Acute Achilles tendon rupture associated with medial malleolar fracture: is it still a rare injury? Case report and review of the literature Int J Foot Ankle Fontecilla N Hube M Bastías G Fuentes P Arancibia M 1722018 https://www.researchgate.net/profile/Gonzalo-Bastias/publication/329138861_Acute_Achilles_Tendon_Rupture_Associated_with_Medial_Malleolar_Fracture_Is_it_Still_a_Rare_Injury_Case_Report_and_Review_of_the_Literature/links/5bf 75f 77458515 a 69e 34b 0cf/Acute-Achilles-Tendon-Rupture-Associated-wit
- 8Functional rehabilitation of patients with acute Achilles tendon rupture: a meta-analysis of current evidence Knee Surg Sports Traumatol Arthrosc Mark-Christensen T Troelsen A Kallemose T Barfod KW 185218592420162505190910.1007/s 00167-014-3180-5 · doi ↗ · pubmed ↗