ST-segment elevation myocardial infarction in Nail–Patella syndrome with anomalous coronary anatomy and aneurysms: a case report
Kyle Varkoly, Akarsh Parekh, Jason Kaplan, Michael Blair DeYoung

TL;DR
A rare case of heart attack in a patient with Nail–Patella syndrome shows unusual coronary artery issues and successful treatment.
Contribution
First reported case of coronary anomalies and successful revascularization in a Nail–Patella syndrome patient.
Findings
Patient with Nail–Patella syndrome had anomalous coronary anatomy and aneurysms leading to heart attack.
Successful stent placement in overlapping fashion resolved occlusion without complications.
Highlights potential for systemic vascular anomalies in Nail–Patella syndrome due to collagen alterations.
Abstract
Nail–Patella syndrome (NPS) is an autosomal-dominant pleiotropic condition characterized by pelvic and skeletal abnormalities and most commonly affecting a tetrad of nails, knees, elbows, and iliac horns, the iliac horns being pathognomonic for the condition. The most well-documented extra-skeletal manifestation is renal involvement with alteration in Type III collagen. No documented cases of NPS with anomalous coronary arteries or aneurysms, acute coronary occlusion, or successfully coronary interventions exist in the medical literature. A 62-year-old female with a medical history significant for NPS diagnosed 50 years ago presented to the emergency department with a chief complaint of chest pain. She recently developed end-stage renal disease managed with peritoneal dialysis within the last year. Angiography revealed 100% right coronary artery occlusion with an anomalous take-off…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1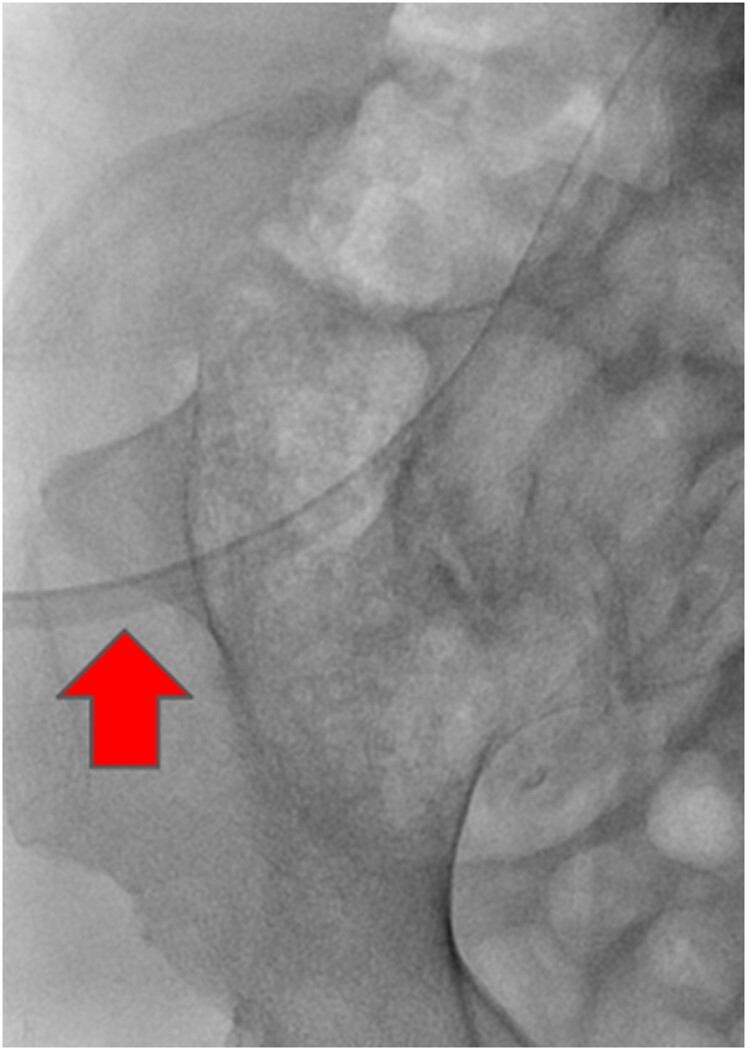 Figure 2
Figure 2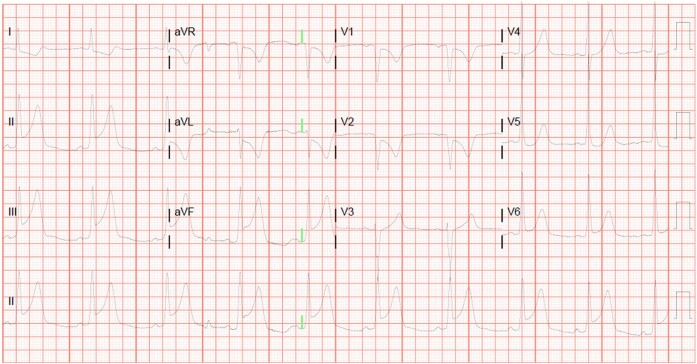 Figure 3
Figure 3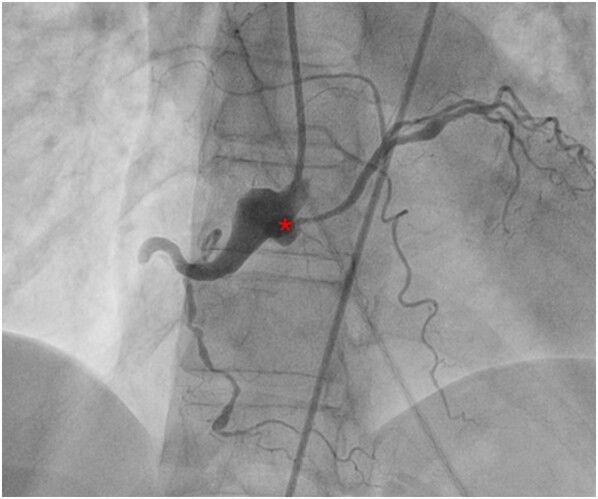 Figure 4
Figure 4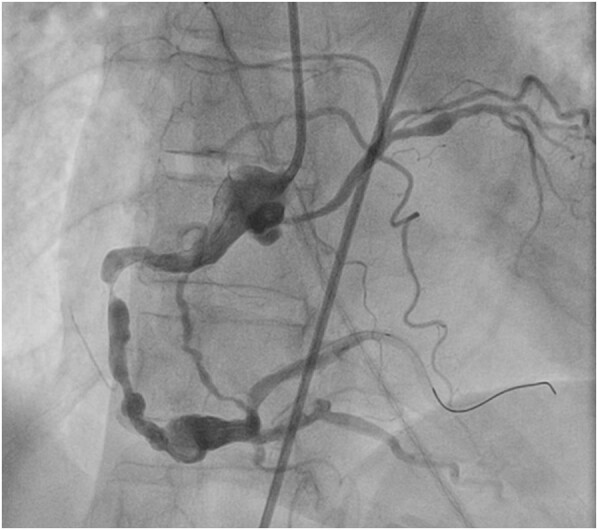 Figure 5
Figure 5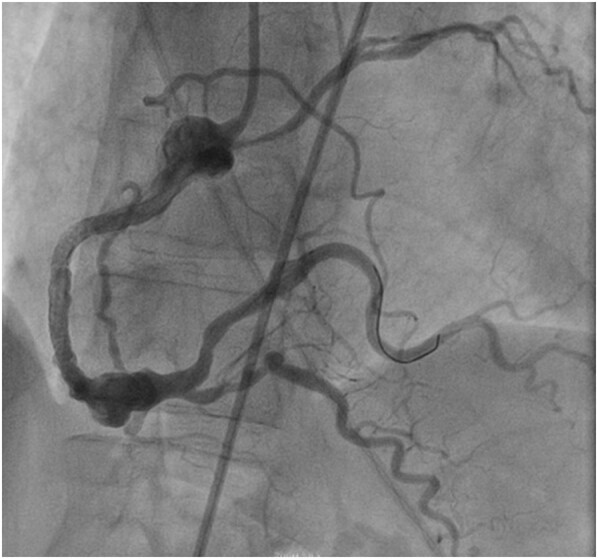 Figure 6
Figure 6| Day 0: Patient presentation | The patient presented with inferior STEMI with posterior extension on ECG |
| Day 0: Workup and treatment | The patient was given ACS medications and immediately sent to a cardiac catheterization laboratory |
| Day 0: Coronary angiography | Angiography revealed 100% RCA occlusion with an anomalous take-off of the LCx. Diffuse coronary aneurysms were demonstrated in the RCA, mid-LAD, proximal Cx artery arising from the RCA, and right obtuse marginal branch of the anomalous Cx artery |
| Day 0: Intervention #1 | RCA was successfully stented over the stenotic lesion. Grade III TIMI Flow was observed immediately after the procedure |
| Day 0: Intervention #2 | An additional DES was placed over the distal RCA segment to approximate the RCA aneurysm in overlapping fashion with the initial DES |
| Day 0: Intervention #3 | Following complete stent placement, our patient experienced hypotension with arrhythmias. Following brief use of an intra-aortic balloon pump (IABP) intraoperatively due to concerns over contributing to cardiogenic shock, the arrythmias and hypotension ceased and IABP was weened |
| Day 2: Patient discharge | The patient was successfully discharged 2 days later without further complication |
| Day 15: Outpatient follow-up | Our patient followed up without recurrence of chest pain and was compliant with medical therapy |
| Day 21: Intervention #4 | LCx was revascularized successfully without complication |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Vascular anomalies and interventions · Acute Myocardial Infarction Research
Introduction
Nail–Patella syndrome (NPS), also known as hereditary onycho-osteodysplasia or Fong disease, is a rare autosomal-dominant pleiotropic condition of pelvic and skeletal abnormalities. It more commonly affects a tetrad of nails, knees, elbows, and iliac horns, with the iliac horns being pathognomonic for the condition. The most well-documented extra-skeletal manifestation of NPS is renal involvement, affecting a rough estimate of 12–55% of patients with NPS.^1^ Nail–Patella syndrome is caused by mutations in the LX1B gene, which is associated with abnormal Type III collagen distribution.^1–4^
Summary figure
**: **
Coronary arterial aneurysms (CAAs) are greater than 1.5-fold local dilatations in coronary arteries. Their rate of incidence in the general population ranges from 0.3 to 5.3% with a mean pooled cohort analysis of 1.65%.^5^ Patients with NPS are presently not known to have inherent CAAs. Genetic studies have yet to identify coronary or vascular anomaly subtypes in patients with NPS.^1,3,4^ Coronary arterial aneurysms have a higher incidence in mixed connective tissue diseases (CTDs) affecting collagen distribution, such as the well-studied Ehlers–Danlos syndrome (EDS) and Marfan syndrome.^5–7^ Both EDS and NPS are a subtype of CTD affecting Type III collagen. Upon autopsy of a female patient with the vascular subtype of EDS who died of a splenic arterial aneurysmal rupture, it was found that the patient additionally had multiple right coronary arterial aneurysms, with no CAAs identified in the left coronary artery.^7^ Coronary aneurysms have also been reported in the left coronary artery in Loeys–Dietz syndrome, a lesser-known mixed CTD.^8^ Furthermore, atypical vascular malformations such as internal carotid artery aplasia have been reported in a patient with NPS.^9^
In this study, we present a case of a patient with NPS who arrived with an ST-segment elevation myocardial infarction (STEMI) and presented with an abnormal and challenging coronary anatomy. After studying the vascular nature of the genetic disorder and after careful stent apposition and deployment, we revascularized our patient without complication.
Case summary
A 62-year-old female presented to the emergency department with a chief complaint of chest pain, nausea, and vomiting. Her medical history included NPS diagnosed at age 12 and end-stage renal disease managed with peritoneal dialysis within the last year. Home medications at the time of presentation included carvedilol 25 mg twice a day, simvastatin 40 mg daily, calcitriol 0.5 mg daily, and sodium bicarbonate 650 mg three times a day. Past operations included a remote history of hysterectomy and peritoneal dialysis placement within the past year. Our patient had no known allergies. Social history included a remote history of cigarette smoking. Family history was unable to be obtained as our patient was an adopted case. Our patient’s known history of NPS was corroborated through characteristic physical examination findings (Figure 1A–C). Ultimately, radiographic imaging demonstrating iliac horns, which are pathognomonic for the syndrome, confirmed the diagnosis (Figure 2). She had no known history of Kawasaki disease in childhood.
The patient demonstrating phenotypic characteristics common in Nail–Patella syndrome. (A) Elbow deformity. (B) Fingernail dysplasia. (C) Abnormal patella.
An anteroposterior right pelvic radiograph demonstrating the presence of a triangular osseous protrusion from the posterior aspect of the right ilia, the right iliac horn.
On arrival, our patient presented with a chief complaint of chest pain. Pertinent positive and negative presenting physical examination findings include diaphoresis and stable vital signs without hypotension. She was found to have an inferior STEMI with posterior extension on initial electrocardiogram (ECG; Figure 3). Following this ECG, the differential broadened to spontaneous coronary artery dissection, aortic dissection, pulmonary embolism, pneumothorax, oesophageal rupture, cardiac tamponade, and an inferior infarction. Our patient’s maximum troponin level, the initial troponin level on admission, was 2679.9 ng/L. Brain natriuretic peptide levels (BNP) were elevated at 7595 pg/dL. A STEMI alert was activated, and the patient was emergently taken to the catheterization laboratory for coronary angiography for her probable inferior infarction. Bedside transthoracic echocardiography (TTE) was not performed in the interest of preserving myocardial tissue in the setting of STEMI requiring emergent revascularization. Coronary angiography revealed diffuse coronary aneurysms in the right coronary artery (RCA), a complete acute occlusion of the RCA, and an anomalous left circumflex (LCx) artery off the right coronary ostium (Figure 4; Supplementary material online, Video S1). A decision was made to intervene on the RCA. Additionally, coronary aneurysms were demonstrated in the RCA, mid-left anterior descending artery, proximal circumflex artery arising from the RCA, and right obtuse marginal branch of the anomalous circumflex artery. The anomalous LCx arising from the right coronary sinus coursed posterior to the aorta. The RCA was deemed to be the culprit lesion.
Twelve-lead electrocardiogram concerning for an inferior ST-elevated myocardial infarction with posterior extension.
*A right coronary angiography demonstrating a 100% occlusion of the proximal right coronary artery as well as an anomalous left circumflex artery off the right coronary ostium. Approximate origin of the anomalous left circumflex artery.
The aneurysmal appearance throughout the mid-to-proximal segments of the RCA created a challenge for proper stent apposition (Figure 5). Two 4.0 × 4.0 mm drug-eluting stents were placed in the proximal-to-mid RCA in an overlapping fashion, post-dilated with a 4.0 mm non-compliant balloon (Figure 6; Supplementary material online, Video S1). Our patient did require brief intraoperative use of an intra-aortic balloon pump for transient reduced cardiac output due to reperfusion arrhythmias contributing to hypotension and cardiogenic shock. She was started on a dual antiplatelet therapy of acetylsalicylic acid 81 mg daily and ticagrelor 90 mg twice a day. She was discharged home 2 days following intervention without complication. She continued her follow-up in the outpatient setting for revascularization of her left circumflex, which was completed successfully on another planned hospitalization. Following the above interventions and proper outpatient follow-up, our patient is now on clopidogrel 75 mg q.d., which she will take indefinitely. A follow-up TTE following her left circumflex intervention revealed no regional wall motion abnormalities.
A right coronary angiography after wiring demonstrating an aneurysmal right coronary artery.
A right coronary angiography demonstrating two 4.0 mm overlapping stents placed in the proximal-to-mid right coronary artery.
Discussion
Nail–Patella syndrome is a known autosomal-dominant pleiotropic disorder with concerns for vascular pathologies due to its effects on Type III collagen, particularly if renal involvement is present. Much like the nails, skeletal bones, and tendons, the vascular endothelial walls are made of collagen, particularly Types I and III. In pathologic skeletal conditions, there is an abnormally high collagen Type III/Type I ratio, as Type III collagen is known to have less tensile strength when compared with Type I collagen.^2^ Nail–Patella syndrome is known to lead to an irregular distribution of Type III collagen, particularly in phenotypes with renal involvement.^3^
Coronary arterial aneurysms are most commonly caused by atherosclerosis. Coronary arterial aneurysms have a higher rate of incidence in atherosclerotic males than in atherosclerotic females (2.2 vs. 0.5% at a single-centre study).^5^ Hereditary CTD, such as EDS and Marfan syndrome, have been shown to cause CAAs, driven by a gene mutation with resultant transforming growth factor-β (TGF-β) overactivity causing cystic medial necrosis.^5,6^ However, cystic medial necrosis has also been identified in patients with CAAs without Marfan syndrome, and in these patients, medial necrosis, fibrosis, and atherosclerosis also directly correlated with age.^6^
Type III collagen is implicated in the vascular subtype of EDS. Upon autopsy of a female patient with EDS who died of splenic arterial aneurysmal rupture, it was found that the patient was uncovered to have a right coronary aneurysm as well.^7^ Loeys–Dietz syndrome, another CTD affecting Type III collagen, has also been reported to have coronary aneurysms.^8^ Already, hereditary internal carotid artery aplasia has been reported as a vascular abnormality in a patient with NPS.^9^ Given the increased identification of anomalous vascular abnormalities in patients with CTDs, it is reasonable to identify other potential drivers in NPS potentially accelerating CAA formation.
An anomalous LCx take-off of the right coronary sinus is classified as a coronary artery anomaly, which are anomalies identified in <1% of the general population.^10^ The anomalous course usually continues posterior to the aorta and is considered benign. The rate of incidence of an anomalous LCx is overall rare, which approached 0.26% in a single-centre retrospective observational study of 2684 coronary angiography procedures, which was corroborated through other observational coronary angiography studies.^11,12^ Identification of this anomalous coronary artery is important to avoid selective atherosclerosis of this or nearby arteries due to nearby mechanical forces that could possibly invoke spontaneous coronary artery dissection. Such an anomalous take was identified in our patient.
No studies have formally examined NPS and its effects on vascular or coronary malformations. Additionally, no gene mutations have been identified as drivers of vascular or coronary malformations in patients with NPS.^1,3,4^ Due to its known effects on collagen, it is reasonable for interventionists to have concerns for vascular pathology in NPS. Although rare, when managing patients with NPS, physicians should now be aware of a potentially complex anatomy, making routine procedures extensively more difficult, as seen in our patient. Given our limited insights into the vasculature of these patients, additional recommendations for the management of these patients include a full body computed tomography with brain to pelvis imaging, substantially improving outcomes in patients with known aneurysmal non-atherosclerotic vascular disease.^13^
Our patient case shows a rare anatomical variant of coronary aneurysm and anomalous take of LCx, and is the first reported case showing coronary aneurysms in a patient with NPS in the medical literature, a potential association not appreciated in prior genetic reviews of the syndrome.^1,3,4^ Our patient with NPS had a rare coronary anomaly of coronary aneurysm, presenting with a complete occlusion, and was successfully revascularized without intra-hospital complication following additional stent apposition and deployment. No formal guidelines from the European Society of Cardiology exist for revascularization strategies in patients with CTD.^14^ However, time is of the essence in preserving myocardial tissue in the context of STEMI.^15^ Thus, initial revascularization in the case of our patient was reasonable. Ideally, intravascular ultrasound would have been employed prior to stent deployment. However, given the patient’s haemodynamic instability, this was not feasible.
Conclusion
This is the first reported case of coronary vascular anomalies seen in a patient with NPS and is the first successful coronary revascularization in a patient with NPS in the medical literature. Given the potential vascular abnormalities and need for cardiac intervention in patients with NPS, it is reasonable for future studies to examine vascular malformations in this patient population.
Supplementary Material
ytae188_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sweeney E , Fryer A, Mountford R, Green A, Mc Intosh I. Nail Patella syndrome: a review of the phenotype aided by developmental biology. J Med Genet 2003;40:153–162.12624132 10.1136/jmg.40.3.153PMC 1735400 · doi ↗ · pubmed ↗
- 2Kuivaniemi H , Tromp G. Type III collagen (COL 3A 1): gene and protein structure, tissue distribution, and associated diseases. Gene 2019;707:151–171.31075413 10.1016/j.gene.2019.05.003PMC 6579750 · doi ↗ · pubmed ↗
- 3Andeen NK , Schleit J, Blosser CD, Dorschner MO, Hisama FM, Smith KD. LMX 1B-associated nephropathy with type III collagen deposition in the glomerular and tubular basement membranes. Am J Kidney Dis 2018;72:296–301.29246420 10.1053/j.ajkd.2017.09.023 · doi ↗ · pubmed ↗
- 4Marini M , Bocciardi R, Gimelli S, Di Duca M, Divizia MT, Baban A, et al A spectrum of LMX 1B mutations in Nail-Patella syndrome: new point mutations, deletion, and evidence of mosaicism in unaffected parents. Genet Med 2010;12:431–439.20531206 10.1097/GIM.0b 013e 3181 e 21afa · doi ↗ · pubmed ↗
- 5Abou Sherif S , Ozden Tok O, TaşköylüÖ, Goktekin O, Kilic ID. Coronary artery aneurysms: a review of the epidemiology, pathophysiology, diagnosis, and treatment. Front Cardiovasc Med 2017;4:24.28529940 10.3389/fcvm.2017.00024 PMC 5418231 · doi ↗ · pubmed ↗
- 6Klima T , Spjut HJ, Coelho A, Gray AG, Wukasch DC, Reul GJ Jr, et al The morphology of ascending aortic aneurysms. Hum Pathol 1983;14:810–817.6885038 10.1016/s 0046-8177(83)80303-7 · doi ↗ · pubmed ↗
- 7Imahori S , Bannerman RM, Graf CJ, Brennan JC. Ehlers-Danlos syndrome with multiple arterial lesions. Am J Med 1969;47:967–977.5362873 10.1016/0002-9343(69)90210-1 · doi ↗ · pubmed ↗
- 8Jost ZT , Sang CJIII, Lertwilaiwittaya P, Chapman GD. Coronary artery aneurysm in Loeys-Dietz syndrome: a case report. Eur Heart J Case Rep 2022;6:ytac 204.35668844 10.1093/ehjcr/ytac 204PMC 9161713 · doi ↗ · pubmed ↗