Adenosine Deaminase (ADA)-Deficient Severe Combined Immunodeficiency Unmasked by Persistent Lymphopenia and Prolonged Severe SARS-CoV-2 Infection in a Three-Week-Old Neonate
Zaineb Benslimane, Funda Cipe, Khurshid Khan, Maged N Nabawi, Anasalwogud Abdelmogheth

TL;DR
A three-week-old neonate with a severe and prolonged SARS-CoV-2 infection was diagnosed with ADA-deficient SCID, highlighting the importance of recognizing immunodeficiencies in infants with persistent lymphopenia.
Contribution
This case report emphasizes the diagnostic value of persistent lymphopenia in identifying ADA-deficient SCID in regions without newborn TREC screening.
Findings
A neonate with prolonged SARS-CoV-2 infection and lymphopenia was diagnosed with ADA-deficient SCID.
Lymphopenia can serve as a cost-effective screening marker for SCID in regions without TREC newborn screening.
Early recognition of primary immunodeficiencies is critical to prevent severe infections and complications.
Abstract
Adenosine deaminase (ADA) deficiency, an autosomal recessive variant, is the second most common form of severe combined immunodeficiency (SCID). We report a unique case of a three-week-old neonate who presented with prolonged and severe SARS-CoV-2 infection associated with persistent lymphopenia, subsequently revealing ADA-deficient SCID. He presented with mild and insidious symptoms, and then his clinical condition rapidly deteriorated. He required ICU admission and mechanical ventilation and developed multiple co-infections including opportunistic pathogens. Flow cytometry and whole exome sequencing diagnosed ADA-deficient SCID. This case highlights the importance of recognizing primary immunodeficiency disorders in children who consistently display lymphopenia and experience prolonged opportunistic and viral infections. Detecting lymphopenia should prompt consideration of SCID,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
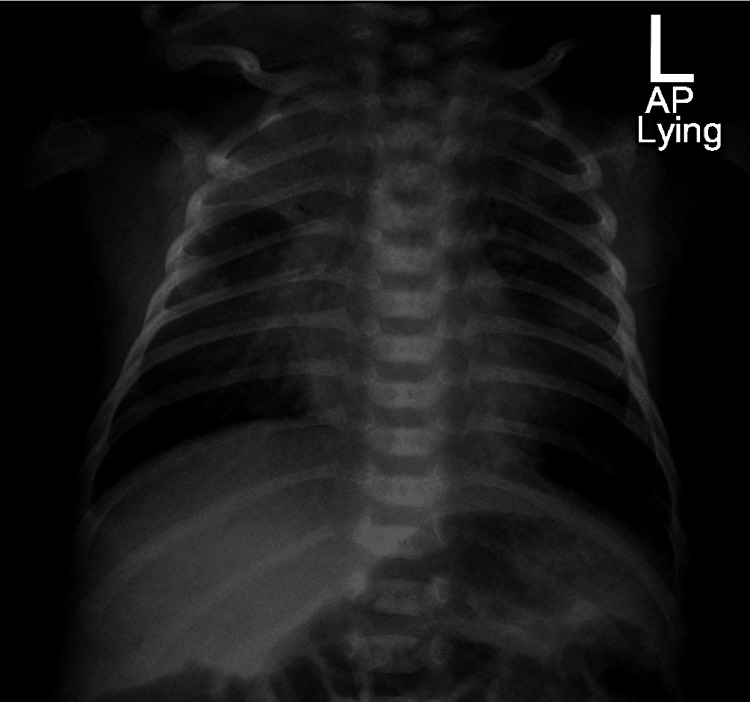 Figure 1
Figure 1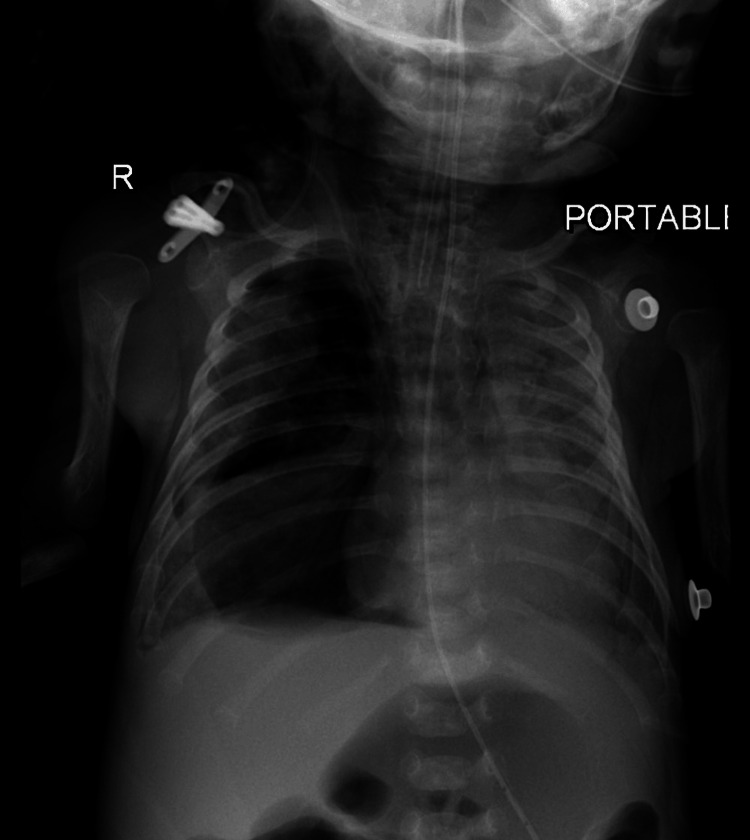 Figure 2
Figure 2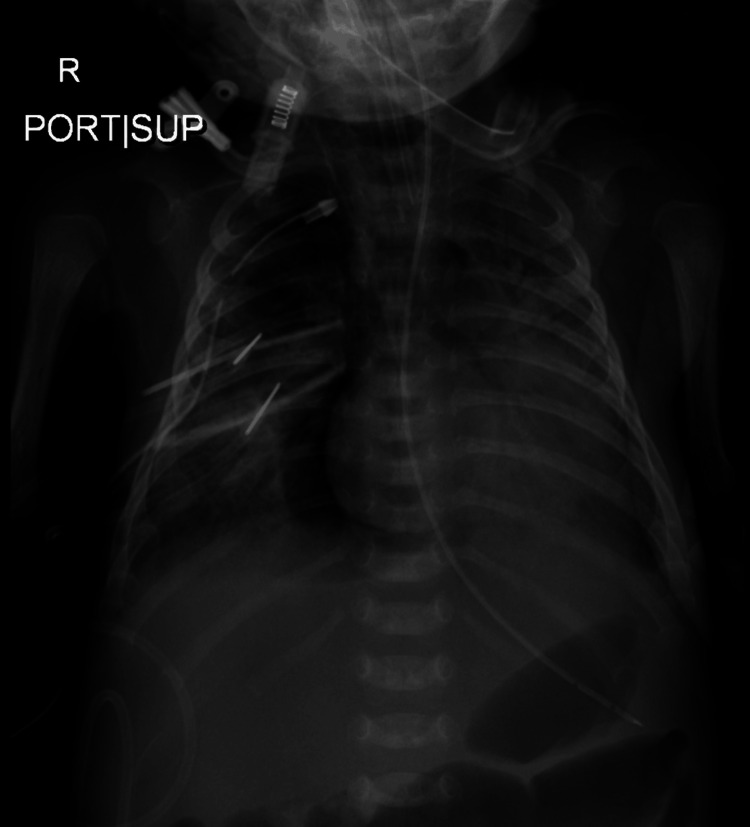 Figure 3
Figure 3| Result | Normal values | |
| White Blood Cell Count | 2250/mcL | 4500-11000/mcL |
| Absolute Neutrophil Count | 1330/mcL | 1000-5000/mcL |
| Absolute Lymphocyte Count | 250/mcL | 4000-10000/mcL |
| CRP | 3.50 mg/dL | < 3.50 mg/dL |
| Results | Normal values | |
| Lymphocytes, total | 0.07 tsd/uL | 3.50-13.10 tsd/uL |
| CD3 | 43% | 60-85% |
| T-lymphocytes (CD3+) | 30/uL | 2300-7000/uL |
| CD4 | 17% | 41-68% |
| T-helper cells (CD3+/CD4+) | 12/uL | 1700-5300/uL |
| CD8 | 10% | 9-23% |
| T-suppressor cells (CD3+/CD8+) | 7/uL | 400-1700/uL |
| CD19+ | 1% | 4-26% |
| B-lymphocytes (CD19+) | 1/uL | 600-1900/uL |
| NK-cells (CD56+) | 22% | 3-23% |
| NK-cells (CD16+/CD56+) | 15/uL | 200-1400/uL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsImmunodeficiency and Autoimmune Disorders · Respiratory viral infections research · Parvovirus B19 Infection Studies
Introduction
Severe combined immunodeficiency (SCID) is a rare life-threatening primary immunodeficiency disorder (PID) that causes early death due to profound impairment of T and B cell functions. Adenosine deaminase (ADA) deficiency, an autosomal recessive variant, is the second most common form of SCID. Typical clinical presentation includes infants with failure to thrive and severe or opportunistic infections [1,2]. We report a unique case of a three-week-old neonate who presented with insidious initial symptoms and then developed prolonged and severe SARS-CoV-2 infection associated with persistent lymphopenia, subsequently revealing ADA-deficient SCID.
Case presentation
Patient information
A three-week-old term male neonate from Afghanistan presented to the Emergency Department with complaints of mild dry cough and nasal congestion for two weeks, associated with decreased oral intake for one day. There was no history of sick contact, fever, dyspnea, diarrhea, or dermatitis. He was born to a mother who had six pregnancies out of which four live births (G6P4) at 37 weeks + 4 days after an uncomplicated pregnancy and a normal delivery with a birth weight of 3.16 kg. His parents were first-degree relatives. Although no immunodeficiency was documented in the family, two male siblings born at full term without complications succumbed to fatal respiratory problems at the age of three months. He was exclusively breastfed and up to date in his vaccination. He received the mandatory hepatitis B and BCG vaccines after birth as per the local immunization program in the United Arab Emirates (UAE).
Clinical findings
On admission, the baby was hemodynamically stable and afebrile. He only displayed mild tachypnea and mild subcostal retractions. He was maintaining saturation on room air and his chest auscultation revealed few conductive sounds. His CBC showed leukopenia and lymphopenia while his CRP was 3.50 mg/dL (Table 1). A SARS-CoV-2 nasopharyngeal swab for PCR was collected.
A chest X-ray showed a consolidation in the right upper lung, diffuse interstitial infiltrates, and bilateral accentuated broncho-vascular markings (Figure 1). He was initially admitted to the pediatric ward as a case of pneumonia and to rule out neonatal sepsis. Cerebrospinal fluid, blood culture, and urine culture were collected and he was started on intravenous cefotaxime and penicillin. Cultures were later reported negative; however, his SARS-CoV-2 PCR came back positive and he was diagnosed with COVID pneumonia. On the second day of admission, his clinical condition started to deteriorate. He developed moderate respiratory distress and required oxygen via nasal cannula but remained afebrile. He was transferred to the Pediatric ICU where he was connected to a high-flow nasal cannula.
Chest X-ray (anterioposterior view) on admission showing right upper lung zone consolidation, diffuse interstitial infiltrates, and accentuated bronchovascular markings bilaterally.
Timeline of the current episode
Throughout his five weeks hospital course, his SARS-CoV-2 PCRs were persistently positive, he exhibited persistent lymphopenia with an absolute lymphocyte count reaching 250/mcL but had near-normal serum immunoglobulin levels. He suffered from progressive left lung pneumonia and infiltrative lung disease (Figure 2) and required mechanical ventilation. Microbiological investigations revealed multiple co-infections including Enterococcus feacalis pneumonia, Enterobacter cloacae urosepsis, and methicillin-resistant Staphylococcus aureus infection in the eyes and throat. There was no oral thrush, and no signs of BCGitis, but he exhibited a very poor weight gain of 240 grams over five weeks.
Chest X-ray (anteroposterior view) done two weeks after admission showing infiltrative lung disease and a progressive course of left lung inhomogeneous opacities.
Diagnostic assessment
In front of this clinical picture, SCID was suspected. Flow cytometry revealed severely diminished NK-cells and T-lymphocytes while B-lymphocytes were almost not detectable (Table 2), thus diagnosing SCID T- B- NK-.
Therapeutic interventions
On admission, he was started on cefotaxime and penicillin in view of pneumonia and possible neonatal sepsis. Antimicrobials were then upgraded to Ertapenem as treatment and Trimethoprim/Sulfamethoxazole, Acyclovir, and Fluconazole as prophylaxis. His treatment also included regular intravenous immunoglobulin replacement, Remdesivir, and Dexamethasone for COVID-19 infection.
Follow-up and outcome interventions
His condition rapidly declined, leading to multi-organ dysfunction syndrome marked by acute respiratory distress syndrome (Figure 3), septic shock, and liver dysfunction. Unfortunately, he succumbed at the age of two months.
Chest X-ray (anteroposterior view) on the day of death showing pneumomediastinum and bilateral diffuse airspace shadowing.
Bone marrow transplantation, the method of choice in SCID treatment [2], could not be done in view of the patient’s critical condition. Whole exome sequencing was sent and ADA-deficient SCID was genetically confirmed post-mortem. It identified a pathogenic autosomic recessive homozygous variant c.704G>Ap.(Arg235Gin) chr20/43251546 (MIM: 102700).
Discussion
SCID is a pediatric emergency, the diagnosis starts with suspicion and the treatment should be initiated promptly, otherwise, survival beyond one-year-old is unlikely [2].
In our case, the persistent lymphopenia even with normal immunoglobulin levels, the persistent COVID-19 PCR positivity, the development of opportunistic co-infections, and the rapid clinical deterioration were all suggestive of SCID. This case shows that absolute lymphopenia can be used as a simple and inexpensive screening method for SCID in newborns and children in general [3], especially in countries where T-cell receptor excision circles (TRECs) are not included in newborn screening like the UAE. Moreover, it shows that normal immunoglobulin levels do not rule out immunodeficiency in infants less than 6 months of life as maternal immunoglobulins are still not weaned.
A systematic review of 116 articles about the severity of SARS-CoV-2 infection in children with PID involving 710 pediatric cases including 42 patients with SCID found that these children may have higher rates of prolonged infections, disease severity, ICU admission, use of mechanical ventilation, acute respiratory distress syndrome and mortality. These findings highlight the importance of preventing infections like COVID-19 in children with PID [4].
For ADA-deficient SCID, allogeneic hematopoietic stem cell transplant or autologous hematopoietic stem cell and ADA gene therapy are the only curative treatments. Enzyme replacement therapy can be used as a bridge therapy until stem cell transplantation is available [2]. Unfortunately, these therapies couldn’t be initiated for our patient as he was unstable clinically.
Conclusions
This case highlights the importance of considering underlying PID in children exhibiting prolonged opportunistic and viral infections, such as SARS-CoV-2, particularly when accompanied by a significant family history. Absolute lymphopenia should raise the suspicion of SCID in children. This point holds great importance especially in countries where TRECs are not included in the newborn screening. Early diagnosis and treatment are crucial in improving outcomes of bone marrow transplant and saving the life of SCID patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Severe combined immunodeficiency Stat Pearls [Internet] Vaillant AA Mohseni M Treasure Island (FL)Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 539762/30969584 · pubmed ↗
- 2Adenosine deaminase deficiency Gene Reviews® [Internet] Hershfield M Tarrant T Seattle (WA)University of Washington, Seattle 2006 https://www.ncbi.nlm.nih.gov/books/NBK 1483/20301656 · pubmed ↗
- 3Neonatal lymphopenia screening is important for early diagnosis of severe combined immunodeficiency Am J Perinatol Poyraz A Cansever M Muderris I Patiroglu T 7487524020233411658310.1055/s-0041-1731044 · doi ↗ · pubmed ↗
- 4Severity of SARS-Co V-2 infection in children with inborn errors of immunity (primary immunodeficiencies): a systematic review Allergy Asthma Clin Immunol Alhumaid S Al Mutared KM Al Alawi Z 691920233755915310.1186/s 13223-023-00831-1PMC 10413516 · doi ↗ · pubmed ↗