Integrated Yoga and Naturopathy Interventions to Modify Functional Disability in Patients With Spinal Cord Injury: A Randomized Controlled Trial
Sujatha KJ, Manjunath N K, Prashanth Shetty

TL;DR
This study found that combining yoga and naturopathy with routine care improves functional independence in spinal cord injury patients.
Contribution
The study introduces integrated yoga and naturopathy as effective adjuvant therapies for spinal cord injury rehabilitation.
Findings
Integrated yoga and naturopathy significantly improved functional independence (SCIM) in spinal cord injury patients.
The intervention group showed significant improvements in muscle strength, balance, and mobility compared to routine care.
Results were measured using standardized tests like TUG, BBS, and 10MWT, showing consistent improvements.
Abstract
Objective: This study aimed to evaluate the use of integrated yoga and naturopathy intervention to modify functional disability and improve independence in patients with spinal cord injury. Materials and methods: In this randomized controlled trial, 48 spinal cord injury patients receiving residential rehabilitation, aged between 23 and 57 years (37.9±11.8) of both genders, were randomly allocated to two groups: (i) experimental group (naturopathy and yoga) and (ii) control group (waitlist with routine care). Subjects were assessed on day 1 (baseline), day 30 (intense phase), and day 90 (follow-up). Assessments were done using the Spinal Cord Independence Measure (SCIM), handheld myometry (HHM), time up and go (TUG), Berg Balance Scale (BBS), and 10-meter walk test (10MWT). Results: There were no significant differences at baseline between groups for all the variables (p>0.05) through…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
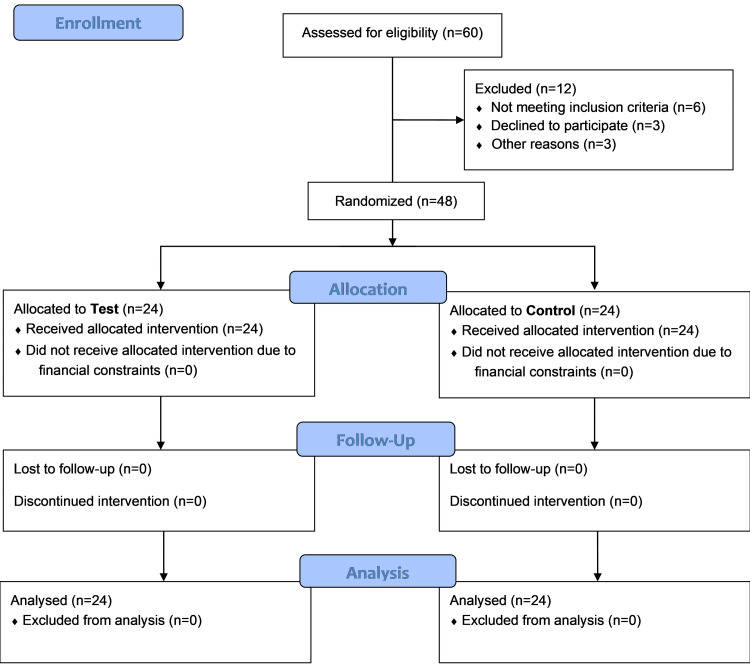 Figure 1
Figure 1| Type of practice | Name of the practice | Duration (frequency) practice |
| Loosening exercises (Sukshma Vyayama) of the upper limb | Finger movements | Five minutes (five rounds for each movement) |
| Wrist movements | ||
| Elbow movements | ||
| Shoulder movements | ||
| Loosening exercises (Sukshma Vyayama) of the lower limb | Toe movements | Five minutes (five rounds for each movement) |
| Ankle movements | ||
| Knee movements | ||
| Hip movements | ||
| Asanas (with support or props) | Utkatasana | Two minutes (two repetitions) |
| Ardha Chakrasana | ||
| Ardhakati Chakrasana | ||
| Vakrasana | ||
| Pranayamas | Vibhagiya Pranayama (sectional breathing) | Six rounds (three minutes) |
| Nadi Shuddhi Pranayama | Nine rounds (five minutes) | |
| Bhramari Pranayama | Nine rounds (five minutes) | |
| Relaxation | DRT | 10 minutes |
| Variable | Test | Control | ||||
| Day 1 | Day 30 | Day 90 | Day 1 | Day 30 | Day 90 | |
| Self-care | 8.25±1.36 | 10.5±1.22*** | 13.4±1.69***, † † † | 8.71±1.20 | 9.96±1.23*** | 10.8±1.36***, † † † |
| RSM | 34.7±1.2 | 35.8±1.17*** | 36.6±0.83***, † † † | 34.8±1.38 | 35.5±1.32*** | 35.9±1.14***, † † † |
| Mobility | 21.2±2.57 | 24.6±2.52*** | 28.1±2.34***, † † † | 21.3±2.58 | 22.7±2.54*** | 23.9±2.52***, † † † |
| Variables | Test | Control | ||||
| Day 1 | Day 30 | Day 90 | Day 1 | Day 30 | Day 90 | |
| Right hand (N) | 18.2±5.75 | 19.9±4.74*** | 21.9±4.31***, † † † | 15.9±5.08 | 16.9±4.95*** | 18.6±4.31***, † † † |
| Left hand (N) | 19±5.94 | 21.2±5.55*** | 23.1±4.74***, † † † | 18.1±4.74 | 19.4±4.47*** | 21.4±4.03***, † † † |
| Variables | Test | Control | ||||
| Day 1 | Day 30 | Day 90 | Day 1 | Day 30 | Day 90 | |
| TUG (s) | 87.5±16.7 | 78.4±15.3*** | 66.5±14.4***,† † † | 88±16.8 | 82.3±16.3*** | 77.1±15.8***,† † † |
| 10MWT (m/s) | 0.0779±0.0118 | 0.0856±0.0140*** | 0.0979±0.0166***,† † † | 0.0801±0.0169 | 0.0872±0.0197*** | 0.0930±0.0265***,† † † |
| BBS | 33.8±4.49 | 37.2±3.27*** | 40.7±1.99***,† † † | 33.6±4.54 | 35.0±4.15*** | 36.5±3.67***,† † † |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpinal Cord Injury Research · Cerebral Palsy and Movement Disorders · Stroke Rehabilitation and Recovery
Introduction
Functional disability often ensues from spinal cord injury (SCI). The impairment is visible in the ability to execute activities of daily living (ADL). The assessment of ADLs or functional disabilities considers limitations in activities including walking, climbing stairs, grooming, going to the toilet, getting out of bed, and shifting into a chair [1]. Functional impairments with activity restrictions and limitations related to mobility as well as self-care can result in difficulty in pursuing employment, sustaining social relationships, participating in leisure activities, and engaging as a member of the community [2]. The degree of motor function, age of the patient, length of therapy, existence of pressure sores or spasticity, site of the injury, and severity of the damage are all associated with functional disability in SCI [3]. Globally, 2-5 lakh people suffer from SCI, with a male-to-female ratio of 2:1 among adults. Up to 90% of these cases are due to traumatic causes, though the proportion of nontraumatic spinal cord injuries appears to be growing [4]. According to the Rehabilitation Council of India, 15,000 cases of SCI are reported on average every year, with 0.15 million cases occurring annually. India is among the developing nations where SCI is becoming more common, and the associated healthcare burden is predicted to be comparable to that of the developed world [5]. Complementary and integrative medicine are growing in popularity in the United States, reducing the healthcare burden. In 2012, 33.2% of adult US citizens said they had used alternative therapy at some point in the past year. The most common practices were deep breathing exercises, yoga, tai chi, and chiropractic adjustments; nevertheless, the use of qi gong, yoga, and dietary supplements increased linearly between 2002 and 2012. The reported usage of complementary therapies varies widely among individuals with SCI, ranging from 14% to 73%. Studies that focused on individuals with both SCI and chronic pain showed higher rates. However, most of the samples have been tiny, and prior research has concentrated on the consequences of SCI as well as the initial weeks of inpatient rehabilitation for patients who have recently received a diagnosis of SCI and who have been informed about its potential impact on physical or psychological outcomes [6].
This study is designed to assess the use of integrated yoga and naturopathy intervention to modify functional disability and improve independence in patients with SCI.
Materials and methods
Ethical consideration
The study protocol was approved by the Institutional Ethics Committee of Swami Vivekananda Yoga Anusandhana Samsthana (approval number: RES/IEC-SVYASA/202/2021) and was registered in the Clinical Trials Registry-India (CTRI/2021/10/037130).
Participants
The sample size was calculated using the G*Power software by fixing the alpha at 0.05, the power at 0.8, and the effect size at 0.92 based on the mean and standard deviation of low frequency (%) from a previous study [7]; considering 20% attrition rate, the optimal sample size was 24 in each group. The subjects were recruited from the spinal rehabilitation center as per the diagnostic criteria of the American Spinal Injury Association (ASIA) scoring system [8]. Recruits included 48 subjects of both genders (males: 95.64%, females: 4.16%), ranging in age from 37.9±11.8 years to 7 years, with varying injury durations while hospitalized for rehabilitation. The inclusion criteria were the ability to engage in mild physical activity, participate in the intervention safely, and receive SCI grades between B and D in the ASIA scoring system. The study was explained to the participants, whose signed informed consent was taken. Institutional ethics committee approval was obtained.
Data
The design of the study was a randomized controlled trial. Subjects were recruited on a prospective basis and were randomly allocated to two groups by using computer-generated randomization: (i) the experimental group and (ii) the control group. The subjects of the experimental group received an integrated yoga and naturopathy intervention as an adjuvant therapy to routine medical care including physiotherapy for three months as prescribed by the consulting physician, whereas the control intervention group received only routine medical care with physiotherapy for three months. Subjects from both groups were assessed on day 1, day 30, and day 90. The intervention was provided in two phases: intense treatment (30 days) and follow-up (60 days). The time of day was kept constant for both sessions; individual sessions were 22:30 minutes in duration.
Assessments were done by using a 10-meter walk test (10MWT), handheld myometry (HHM), time up and go (TUG), Berg Balance Scale (BBS), and the Spinal Cord Independence Measure (SCIM).
Intervention
Intervention was provided in two phases: the intense treatment phase (30 days) and the follow-up phase (60 days). The assessments were done on the first, 30th, and 90th days. The wait-list control group received the same treatments after three months. The subjects received naturopathy intervention such as a cold and revulsive (three minutes hot and one minute cold) spinal compress for 30 minutes of five rounds along with yogic intervention [9] according to the protocol shown in Table 1.
Both groups underwent physiotherapy intervention as routine care. The physiotherapy exercises were (1) proprioceptive neuromuscular facilitation, (2) slow and sustained stretching, (3) strengthening of antigravity muscles, (4) functional electrical stimulation, and (5) gait training. All these lasted for 60 minutes, six days a week for one month. Later, the participants were asked to follow up for the next 60 days.
Statistical analysis
Data were represented in mean±standard deviation. Repeated measures analysis of variance (RM-ANOVA) followed by post hoc Bonferroni's correction was performed for all the variables, with the level of significance at p<0.05. Data were analyzed using Jamovi 2.4.8.
Results
Initially, 60 patients in total were contacted. The study participants' flowchart is shown in Figure 1.
Illustration of study plan
A total of 48 patients who agreed to participate fulfilled the requirements for inclusion, provided written informed consent, and were assigned to either the yoga and naturopathy group (n=24) or the control group (n=24).
The baseline values of both the groups for all the variables were compared using separate one-way ANOVAs, and the results suggested that there were no significant differences at baseline between the groups (p>0.05).
RM-ANOVAs were performed to compare the differences among the assessments (baseline, first month, and three months or baseline and three months as within-subject factors) and between the two groups. We also performed a post hoc subgroup analysis to compare results at baseline and then after the first month and after three months.
SCIM
Self-Care
An RM-ANOVA was done on the self-care score in the SCIM. Results showed significant group-by-time interaction effects (F=65.5, MS=29.88, p<0.001) and between-subject effects (F=6.21, MS=28.44, p<0.016). However, there was a significant within-subject difference (F=338.1, MS=154.15, p<0.001). Post hoc tests using Bonferroni's correction showed significant differences between the yoga and control groups in post1 and post2 after yoga (p<0.05) as shown in Table 2.
Table 2: SCIM score recorded on days 1, 30, and 90 in both test and control: p<0.01, : p<0.001, †: p<0.05, † † †: p<0.001, repeated measures ANOVA with post hoc analysis: comparing the day 1 values with respective day 30 and day 90 values; †: comparing day 30 and day 90 valuesRSM: respiratory and sphincter management; SCIM: Spinal Cord Independence Measure; ANOVA: analysis of variance
Respiratory and Sphincter Management (RSM)
An RM-ANOVA was done on the RSM score in the SCIM. Results showed significant group-by-time interaction effects (F=3.17, MS=1.896, p<0.047) but not between-subject effects (F=0.983, MS=3.06, p<0.32.7). However, there was a significant within-subject difference (F=47.24, MS=28.25, p<0.001). Post hoc tests using Bonferroni's correction showed significant differences between the yoga and control groups in post1 and post2 after yoga (p<0.05) as shown in Table 2.
Mobility
An RM-ANOVA was done on the mobility score in the SCIM. Results showed significant group-by-time interaction effects (F=82.5, MS=55.39, p<0.001), between-subject effects (F=8.17, MS=144, p<0.006), and a within-subject difference (F=399.9, MS=268.39, p<0.001). Post hoc tests using Bonferroni's correction showed significant differences between the yoga and control groups in post1 and post2 after yoga (p<0.05) as shown in Table 2.
Handgrip
An RM-ANOVA was performed on the handgrip score in SCIM. On the right hand, results showed significant group-by-time interaction effects (F=3.3, MS=3.4, p<0.04), between-subject effects (F=4.24, MS=297.6, p<0.04], and a significant within-subject difference (F=122.52, MS=126.22, p<0.001). On the left hand, results showed significant group-by-time interaction effects (F=4.47, MS=2.5, p<0.01), nonsignificant between-subject effects (F=4.47, MS=2.5, p<0.3), and a significant within-subject difference (F=291.5, MS=163.3, p<0.001). Post hoc tests using Bonferroni's correction showed significant differences between the yoga and control groups in post1 and post2 after yoga (p<0.05) as shown in Table 3.
Table 3: Handgrip score recorded on days 1, 30, and 90 in both test and control: p<0.01; : p<0.001; †: p<0.05; † † †: p<0.001, repeated measures ANOVA with post hoc analysis: comparing the day 1 values with respective day 30 and day 90 values; †: comparing day 30 and day 90 valuesANOVA: analysis of variance
TUG
An RM-ANOVA was performed on the TUG score in the SCIM. Results showed significant group-by-time interaction effects (F=68.1, MS=322.9, p<0.001), nonsignificant between-subject effects (F=1.19, MS=895, p<0.28), and a significant within-subject difference (F=68.1, MS=322.9, p<0.001). Post hoc tests using Bonferroni's correction showed significant differences between the yoga and control groups in post1 and post2 after yoga (p<0.05) as shown in Table 4.
Table 4: TUG, 10MWT, and BBS scores recorded on days 1, 30, and 90 in both test and control: p<0.01; : p<0.001; †: p<0.05; † † †: p<0.001, repeated measures ANOVA with post hoc analysis: comparing the day 1 values with respective day 30 and day 90 values; †: comparing day 30 and day 90 valuesTUG: time up and go; 10MWT: 10-meter walk test; BBS: Berg Balance Scale; ANOVA: analysis of variance
10MWT
An RM-ANOVA was done on the BBS score in SCIM. Results showed significant group-by-time interaction effects (F=21.6, MS=1.87, p<0.001), nonsignificant between-subject effects (F=0.006, MS=5.87, p<0.93), and a significant within-subject difference (F=376.5, MS=0.003, p<0.001). Post hoc tests using Bonferroni's correction showed significant differences between the yoga and control groups in post1 and post2 after yoga (p<0.05) as shown in Table 4.
BBS
An RM-ANOVA was done on the BBS score in the SCIM. Results showed significant group-by-time interaction effects (F=39.5, MS=49.01, p<0.001), between-subject effects (F=4.11, MS=166.8, p<0.04), and a significant within-subject difference (F=235.7, MS=296.2, p<0.001). Post hoc tests using Bonferroni's correction showed significant differences between the yoga and control groups in post1 and post2 after yoga (p<0.05) as shown in Table 4.
Discussion
The results of this trial indicated that modified autonomic dysfunction and improvement in functional outcomes were seen more often in the individuals with SCI who participated in structured yoga and naturopathy interventions with physical rehabilitation compared to physical rehabilitation alone. The results are concurrent with previous mind-body interventions like yogasana, pranayama, and meditation that have helped reduce pain and enhance functional independence and quality of life in SCI patients [9,10]. Although there was a significant improvement in both groups, the group that practiced yoga and naturopathy demonstrated a greater magnitude of change (mean difference) than the group that only received physical rehabilitation. The goal of the current study was to close the knowledge gap regarding potential mechanisms to enhance the functional outcomes of SCI. In addition to yoga, the subjects received naturopathy, which modifies autonomic dysfunction and helps in the control of vascular physiology [11], thermoregulation [12], splanchnic outflow, and adrenaline outflow in SCI patients [13]. Naturopathy interventions like revulsive compresses, when used in conjunction with other interventions, have been shown to improve functional outcomes and reduce pain. These findings are in line with earlier research on cervical spondylosis by Sujatha and Manjunath [14].
In the present study, the improvement in functional outcomes, pain, and quality of life could be due to a profound modification of autonomic dysfunction and a reduction of pain that leads to better functional independence. The ANS's supraspinal influence is disturbed following an SCI, which results in parasympathetic dominance and sympathetic blunting. This causes cardiac dysrhythmias, systemic hypotension, bronchoconstriction, copious respiratory secretions, and uncontrollably high blood pressure, bowel, and bladder functions [15]. The results of the present study are encouraging, in that the yoga and naturopathy interventions along with physical rehabilitation helped improve functional independence. The conclusive evidence derived from the long-term follow-up of three months reinforces previous studies using a short-term follow-up [16-18].
One strength of the present study was that all the participants stayed in the same rehabilitation center for a period of three months, which helped the subjects adhere to the interventions.
Future trials could focus more on early interventions for individuals suffering from SCI, which may result in better and earlier improvement in autonomic dysfunction, functional outcomes, and quality of life.
Conclusions
The present study shows that there was a significant improvement in functional outcomes in both the yoga and naturopathy group and the control group. So, we can include yoga and naturopathy function as adjuvant alongside routine care of physical therapy in a SCI rehabilitation program.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Disability in activities of daily living: patterns of change and a hierarchy of disability Am J Public Health Dunlop DD Hughes SL Manheim LM 378383871997909653710.2105/ajph.87.3.378PMC 1381008 · doi ↗ · pubmed ↗
- 2Health conditions: effect on function, health-related quality of life, and life satisfaction after traumatic spinal cord injury. A prospective observational registry cohort study Arch Phys Med Rehabil Rivers CS Fallah N Noonan VK 4434519920182873268610.1016/j.apmr.2017.06.012 · doi ↗ · pubmed ↗
- 3Factors that influence functional ability in individuals with spinal cord injury: a cross-sectional, observational study S Afr J Physiother Hastings BM Ntsiea MV Olorunju S 2357120153013587310.4102/sajp.v 71i 1.235PMC 6093142 · doi ↗ · pubmed ↗
- 4Do elderly women have more physical disability than men do?Am J Epidemiol Oman D Reed D Ferrara A 83484215019991052265410.1093/oxfordjournals.aje.a 010088 · doi ↗ · pubmed ↗
- 5Spinal cord injury prevalence and treatment modalities Spinal Cord Injury - Current Trends in Acute Management, Function Preservation and Rehabilitation Protocols Ara Z Singh A Raj S London, England Intech Open 2023
- 6Complementary alternative medicine practices and beliefs in spinal cord injury and non-spinal cord injured individuals J Spinal Cord Med Rudra RT Farkas GJ Haidar S Slavoski KE Lokey NE Hudson TR 6596664120182878243110.1080/10790268.2017.1360831 PMC 6217471 · doi ↗ · pubmed ↗
- 7Effects of compression stockings on sympathetic activity and heart rate variability in individuals with spinal cord injury J Spinal Cord Med Rimaud D Calmels P Pichot V Bethoux F Roche F 81883520122233373410.1179/2045772311 Y.0000000054 PMC 3304561 · doi ↗ · pubmed ↗
- 8Classifications in brief: American Spinal Injury Association (ASIA) impairment scale Clin Orthop Relat Res Roberts TT Leonard GR Cepela DJ 1499150447520172781568510.1007/s 11999-016-5133-4PMC 5384910 · doi ↗ · pubmed ↗