Paravertebral retroperitoneal ancient schwannoma mimicking irritable bowel syndrome
Venkiteswaran Muralidhar, Chandrasekaran Kundhavai, Ramvivek Modiem, Singaram Sowmya

TL;DR
A rare case of a spinal tumor caused symptoms like irritable bowel syndrome, which improved after surgery.
Contribution
This case is the first to report increased bowel frequency caused by retroperitoneal ancient schwannoma.
Findings
Symptoms resembling irritable bowel syndrome were caused by a paravertebral retroperitoneal ancient schwannoma.
Surgical resection of the tumor relieved the gastrointestinal symptoms.
This is a rare case linking retroperitoneal schwannoma with increased bowel activity.
Abstract
We report a case of paravertebral retroperitoneal ancient schwannoma (RPAS) with symptoms suggestive of irritable bowel syndrome that was relieved after resection. Very few cases have been reported of RPAS with gastrointestinal symptoms. Increased bowel activity associated with RPAS has not been reported. Our case report suggests that RPAS may present with increased bowel frequency that could be relieved after surgical resection.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1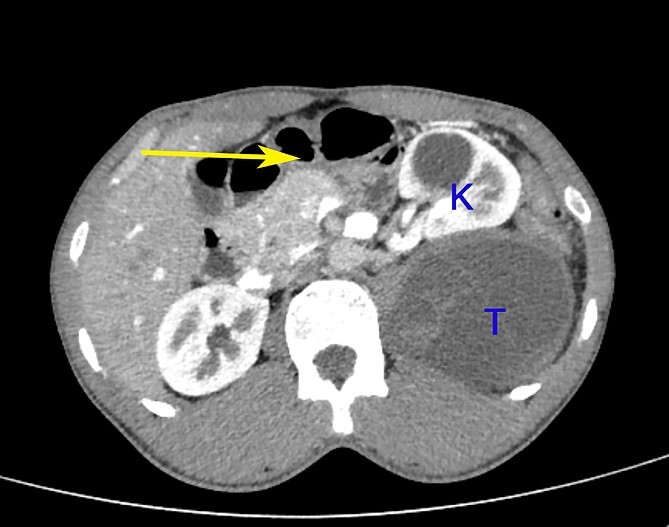 Figure 2
Figure 2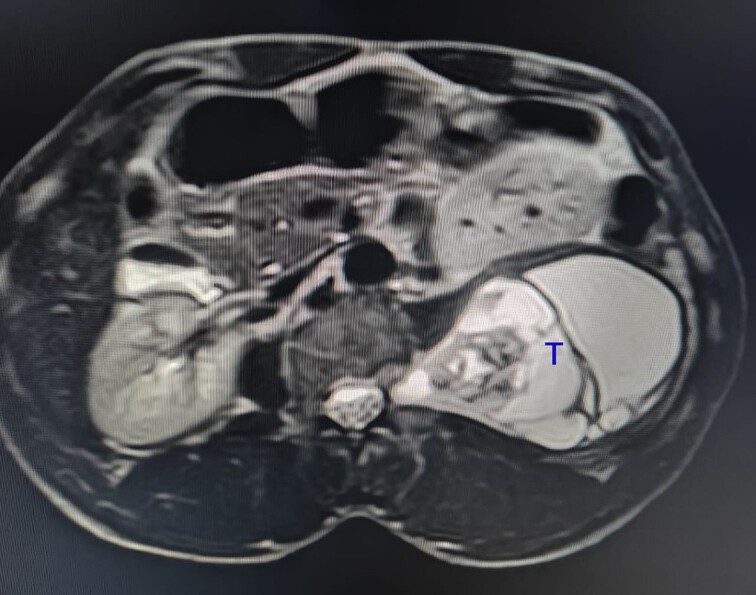 Figure 3
Figure 3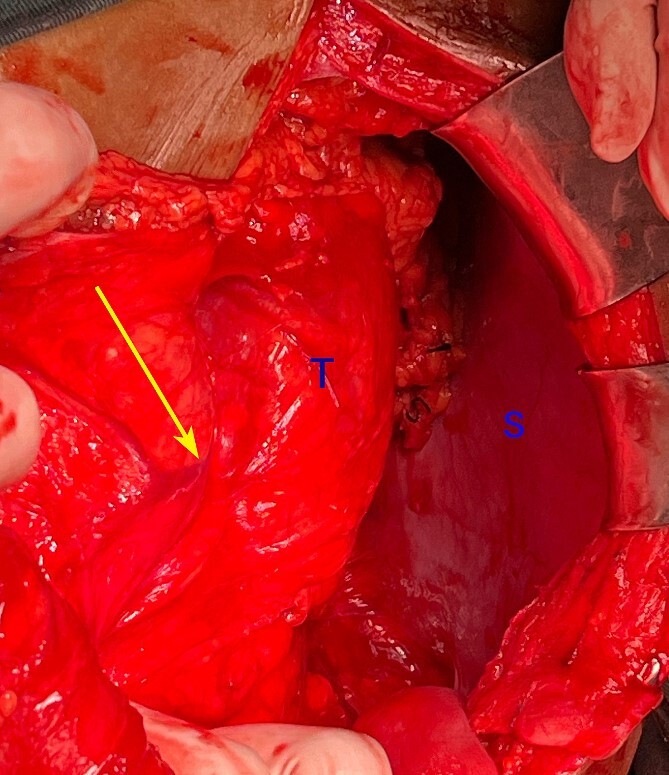 Figure 4
Figure 4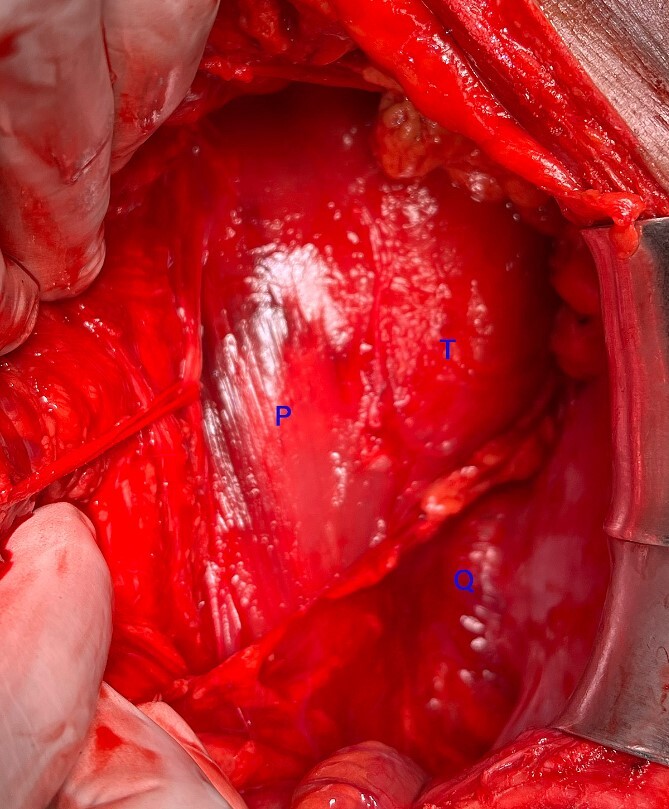 Figure 5
Figure 5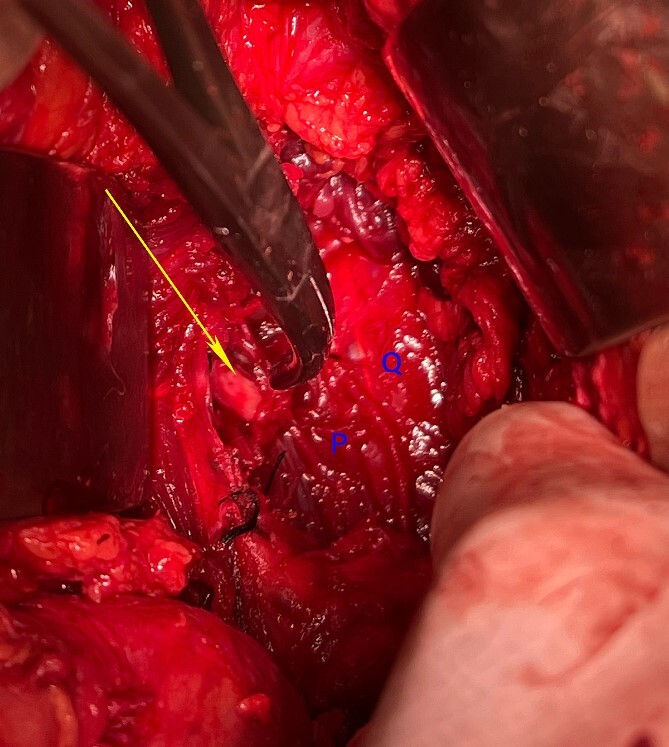 Figure 6
Figure 6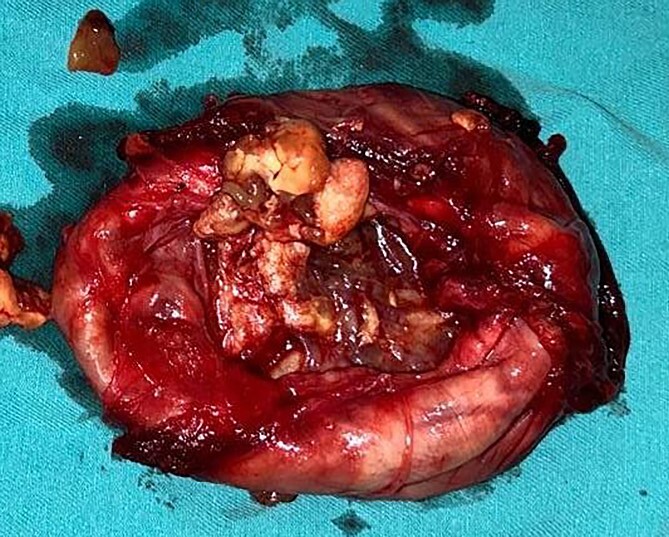 Figure 7
Figure 7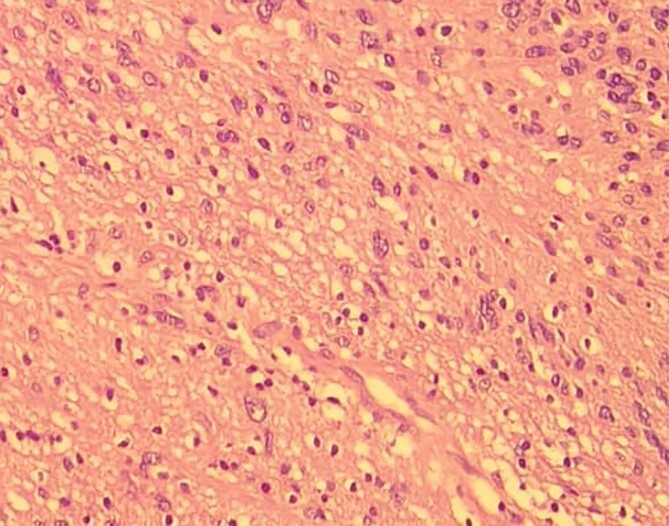 Figure 8
Figure 8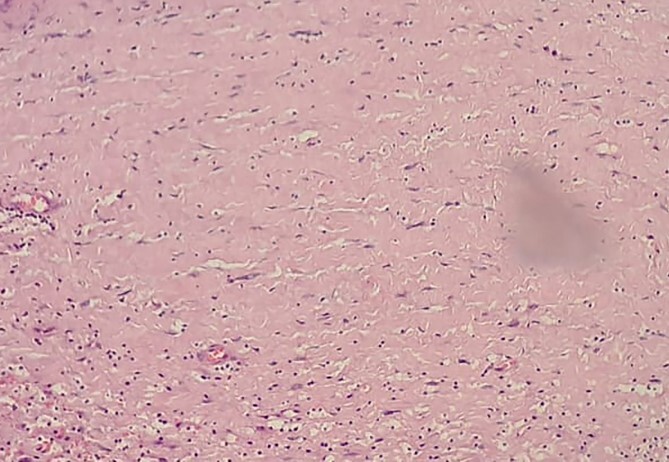 Figure 9
Figure 9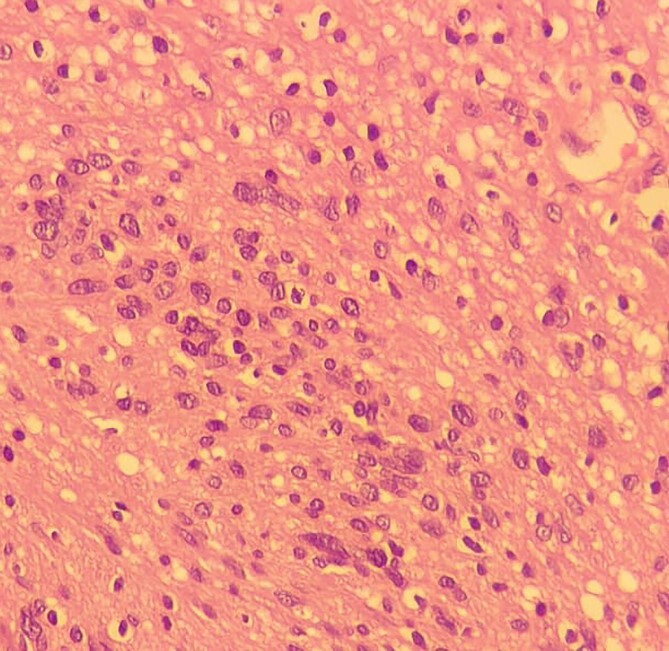 Figure 10
Figure 10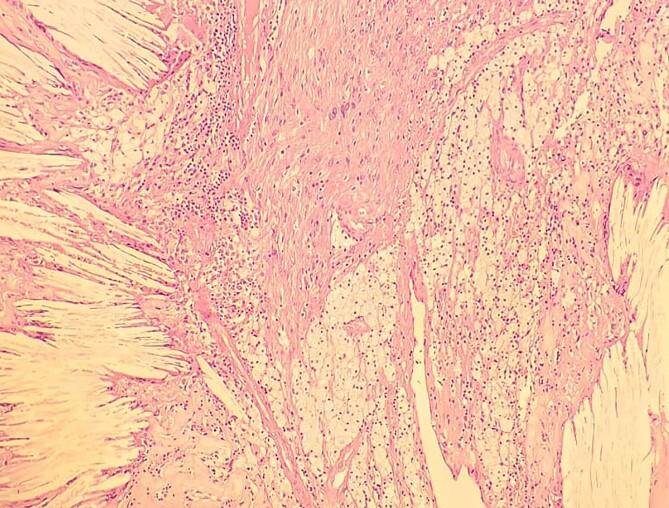 Figure 11
Figure 11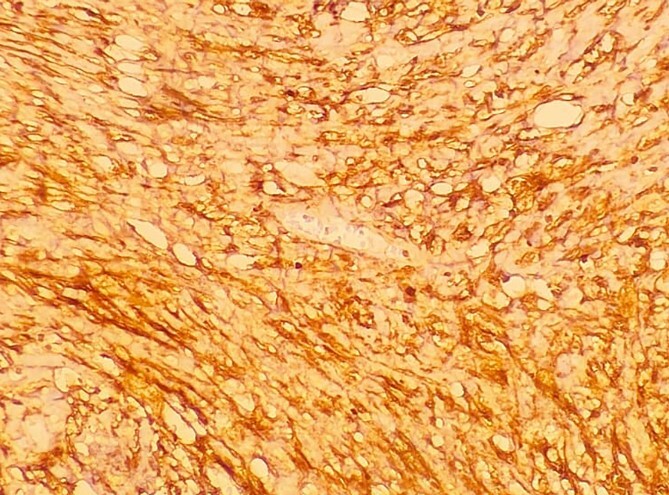 Figure 12
Figure 12| Neural Origin | Schwannoma |
| Gangioneuroma | |
| Meningioma | |
| Neurofibroma | |
| Ependymoma | |
| Neuroendocrine | Paraganglioma |
| Vascular | Arteriovenous Malformations |
| Aneurysms | |
| Malignancies | Soft tissue sarcomas |
| Secondary Metastasis | |
| Osteosarcoma | |
| Miscellaneous | Tuberculous Cold Abscess |
| Prolapsed Intervertebral disc | |
| Haematoma |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurofibromatosis and Schwannoma Cases
Introduction
We report a case of retroperitoneal ancient schwannoma (RPAS) arising paravertebrally from the ventral rami of the second lumbar nerve. The symptoms were mimicking that of an irritable bowel syndrome [1], which was relieved following resection of the tumour. There are many case reports and reviews of RPAS [2–6]. However, extremely few cases of RPAS that presented with gastrointestinal symptoms have been reported [2, 7–9]. Around 1% of schwannomas occur in the retroperitoneum and less than 1% of soft tissue tumours are ancient schwannomas [10]. Most RPAS are asymptomatic, have typical histopathology, are treated by resection and rarely become malignant [11, 12]. The differential diagnosis is listed in Table 1 [12].
Case report
A man in his 30s presented with symptoms suggestive of irritable bowel symptoms with increased bowel movements coinciding with the onset of colicky abdominal pain for the past 8 months. The bowel movements relived his pain and had no remission from his symptoms. He had no relevant medical comorbidities in the past. The patient had normal vitals. There were no physical exam abnormalities except for a slight fullness in the left renal angle (Fig. 1). There was nothing significant on a rectal examination. An X-ray of the chest showed normal findings. Blood investigations showed: haemoglobin 130 g/l, total leukocyte: 7.4 × 10^9^/l, serum creatinine 0.52 mg/dl, fasting blood sugar 90 g/dl, alanine transaminase 26 U/L, aspartate transaminase 42 U/L, alkaline phosphatase 32 U/L and total bilirubin 0.8 mg/dL. Ultrasonography showed a 10-cm mass, with mixed echogenicity. Posterior to the left kidney. Colonoscopy was normal. An abdominal CT scan showed a paravertebral tumour with peripheral enhancement and heterogenous contrast within the tumour (Fig. 2). The tumour showed high intensity on a T2-weighted MRI (Fig. 3). The left kidney and colon were displaced anteriorly. Fine-needle aspiration biopsy was inconclusive. The clinical diagnosis was a retroperitoneal schwannoma. On laparotomy, the left colic vessels appeared to be splayed by the tumour (Fig. 4). The tumour 11 × 6 × 3 cm^3^ (Fig. 5), which seems to be arising from the L2 nerve, was resected completely (Fig. 6). The patient had no sensory or motor loss postoperatively. He was discharged without complications on the 10th postoperative day. His colonic symptoms had disappeared after surgery. The gross appearance of the resected tumour showed cysts and haemorrhage patches (Fig. 7). Histopathology showed areas of hypercellularity (Antony A) and hypocellularity (Antony B) with degenerative changes leading to nuclear atypia and cystic spaces, typical of an ancient schwannoma ([Figs 8](#f8 f9 f10)–11). Immunohistochemistry with S-100 was positive (Fig. 12). He was devoid of digestive symptoms or radiological evidence of recurrence at 12 months.
Clinical photograph showing a fullness in the left loin (cross marked within an oval). The line on the right side shows the location of the 12th rib on that side.
A contrast-enhanced CT scan of the abdomen at the level of the L2 vertebra shows a paravertebral tumour (T) posterior to the kidney (K). The tumour shows peripheral enhancement and inhomogeneous intra-tumoural contrast enhancement. The left colon is pushed to the right and anteriorly (arrow).
The tumour (T) shows a high-intensity signal on a T2-weighted MRI.
Intraoperative photograph showing the left colic vessels are splayed (arrow) by the tumour (T). S: spleen.
Intraoperative photograph showing the paravertebral location of the tumour posterior to the sympathetic chain (looped with an umbilical tape). T: tumour, P: Psoas, Q: quadratus lumborum.
Intraoperative photograph after the tumour resection showing the cut end of the second lumbar nerve (arrow). P: Psoas Major, Q: quadratus lumborum.
Photograph of the excised tumour showing cystic areas and areas of haemorrhages.
Low-resolution 200x H&E histopathology image of the tumour showing hypercellular (Antony A) areas.
Low-resolution 200x H&E histopathology image of the tumour showing hypocellular (Antony B) areas.
High-resolution 400x H&E histopathology image of the tumour showing nuclear atypia suggestive of ancient schwannoma.
Low-resolution 200x H&E histopathology of the tumour showing foamy macrophages and cholesterol clefts suggestive of degenerative changes, suggestive of ancient schwannoma.
A low-resolution 200x S-100 immunostained histopathology image of the tumour showed strongly positive staining.
Discussion
There are three reports of RPAS who presented with constipation that were relieved after resection [2, 7, 9]. In another case, a patient presenting with endoscopically proven colitis had RPAS that was relieved after resection [8]. The authors’ hypothesized that vascular congestion of the colon could have been a reason for the association of colitis with RPAS [8]. Indeed, in our case, the colic vessels were splayed (Fig. 4). We report for the first time a case of increased bowel movements mimicking irritable bowel syndrome that was relieved after resection of the RPAS. The lack of remission of the patient’s lower abdominal symptoms precludes a definitive diagnosis of IBS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Enck P , Aziz Q, Barbara G, et al. Irritable bowel syndrome. Nat Rev Dis Primers 2016;2:16014. 10.1038/nrdp.2016.14.27159638 PMC 5001845 · doi ↗ · pubmed ↗
- 2Gross C , Lecocq J, Isner ME, et al. A rare cause of constipation: neurinoma of the fourth lumbar nerve. Case report and review of the literature. Ann Med Interne (Paris)2002;153:201–5.12218904 · pubmed ↗
- 3Horak S , Cierna Z, Kopecka I, et al. Ancient retroperitoneal schwannoma imitating seminoma recurrence: a case report. Urol Case Rep 2023;46:102304. 10.1016/j.eucr.2022.102304.36582515 PMC 9792343 · doi ↗ · pubmed ↗
- 4Levy AD , Arnáiz J, Shaw JC, Sobin LH. From the archives of the AFIP: primary peritoneal tumors: imaging features with pathologic correlation. Radiographics 2008;28:583–607. quiz 621-582. 10.1148/rg.282075175.18349460 · doi ↗ · pubmed ↗
- 5Saputra A , Sutikno J, Janitra R, et al. Giant lumbar schwannoma with retroperitoneal extension and vertebral body invasion: a case report. Pan Afr Med J Uganda 2023;44:140.10.11604/pamj.2023.44.140.37717 PMC 1027633237333785 · doi ↗ · pubmed ↗
- 6Zaresharifi N , Karimzadhagh S, Ebrahimian R, et al. Successful management of a giant retroperitoneal ancient schwannoma mimicking malignant tumors: a case report and literature review. Ann Med Surg (Lond)2023;85:6279–84.38098556 10.1097/MS 9.0000000000001445 PMC 10718353 · doi ↗ · pubmed ↗
- 7Gao C , Zhu FC, Ma BZ, et al. A rare case of giant retroperitoneal neurilemmoma. J Int Med Res 2020;48:030006052093530. 10.1177/0300060520935302.PMC 749325832924705 · doi ↗ · pubmed ↗
- 8Fass G , Hossey D, Nyst M, et al. Benign retroperitoneal schwannoma presenting as colitis: a case report. World J Gastroenterol 2007;13:5521–4. 10.3748/wjg.v 13.i 41.5521.17907300 PMC 4171291 · doi ↗ · pubmed ↗