Cancer of unknown primary derived from regressed breast cancer
Maria Pouyiourou, Theresa Mokry, Maximilian Feszler, Andrea Teifke, Andreas Kreft, Alwin Krämer

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
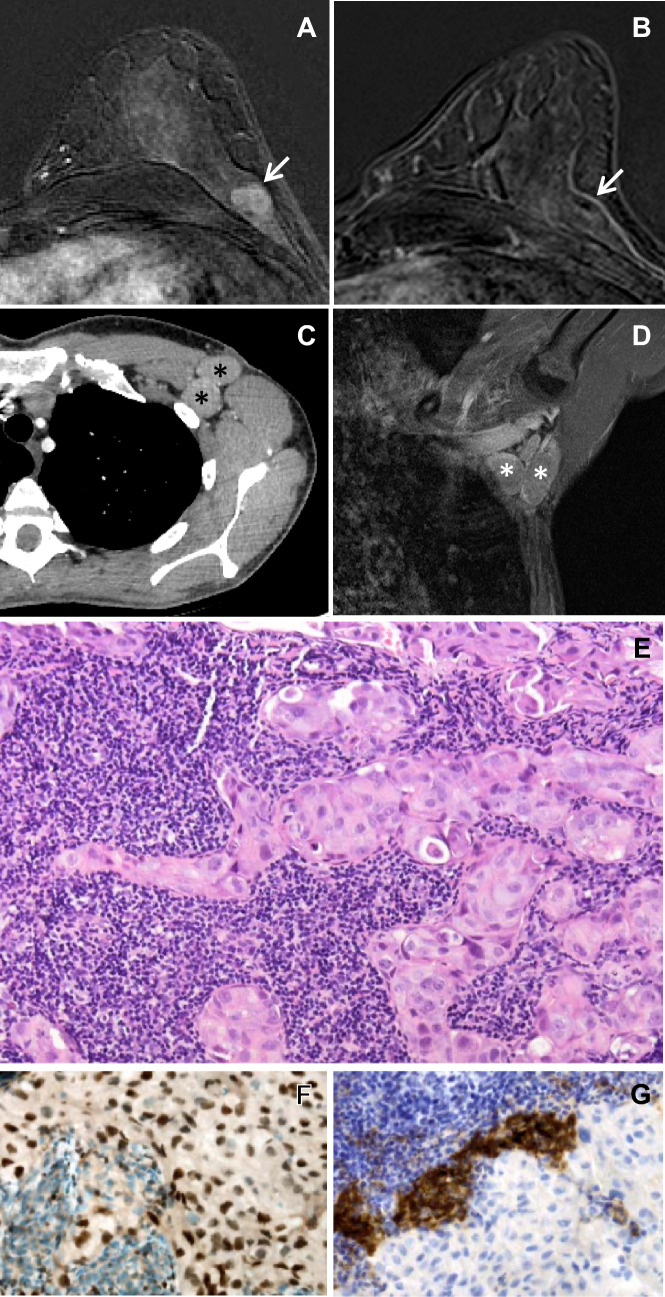 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Diagnosis and Treatment · Cancer and Skin Lesions · Tumors and Oncological Cases
To the editor
Cancer of unknown primary (CUP) is a heterogenous group of cancers for which the anatomical site of origin remains occult even after detailed investigations (Krämer et al. 2023). The unique biology of these tumors remains unknown. Distinct subsets of patients with CUP have been defined, with a minority of patients (15–20%) belonging to clinico-pathological subgroups with a more favorable prognosis, including women with isolated axillary lymph node metastases.
We here describe the case of a 46 year old, premenopausal woman, who was diagnosed with left-sided axillary lymph node metastases of a CK7 + , GATA3 + , Mammaglobin + , CK20-, ER-, PR-, HER2- adenocarcinoma with a proliferation rate of 30%, suggestive of triple-negative breast cancer, in August 2020 (Fig. 1). However, mammography, breast ultrasound and magnetic resonance imaging (MRI) of the breast did not show a breast tumor. Also, abdominal ultrasound, computed tomography of thorax and abdomen, MRI of pelvis, thorax and brain, and bone scintigraphy did not show signs of malignancy, leading to the diagnosis of favorable subtype breast-like CUP syndrome. Neither tumor cells nor blood-derived DNA revealed somatic or germline mutations predisposing to breast and ovarian cancer by whole exome sequencing.Fig. 1. Imaging and histology of left breast and lymph node metastases in the left axilla. Gadolinium-enhanced magnetic resonance imaging (MRI) of the breasts from July 2019 and August 2020 is shown in Panels A and B, respectively. Whereas a lobulated 1 cm tumor in the upper outer quadrant of the left breast is clearly visible in the image from July 2019 (Panel A, arrow), no tumor is found in the corresponding images from August 2020 (Panel B). Panels C and D depict computed tomography (CT) and MRI from August 2020 of lymph node metastases in the left axilla (asterisks), respectively. Panels E, F, and G show hematoxylin–eosin (H&E) staining (400x), and GATA3 and programmed death ligand 1 (PD-L1) (each 400x) immunostainings of a CT-guided core needle biopsy from a lymph node metastasis of the left axilla from August 2020, respectively
Because of microcalcification in the right breast the patient had received yearly screening including mammography, breast ultrasound and MRI since 2011. Retrospectively, in a breast MRI from July 2019 a lobulated, 1 cm tumor in the upper outer quadrant of the left breast with early intensive gadolinium enhancement and subsequent rapid washout (Fig. S1), strongly suggestive of breast cancer, that was no longer detectable in the breast MRI from August 2020, had been overlooked, a finding further corroborating the breast origin of the perceived CUP syndrome.
Due to the assumed origin of breast-like CUP from an occult primary breast cancer, patients with breast-like CUP syndrome are managed according to the treatment protocols for nodal positive breast cancer. Accordingly, the patient received neoadjuvant chemotherapy with epirubicin/cyclophosphamide followed by paclitaxel/carboplatin, and had left-sided axilla dissection plus bilateral mastectomy on her own discretion in 2021. The mastectomy sample revealed no signs of malignant lesions. However, one remaining positive axillary lymph node was detected. The patient then received radiotherapy of the left-sided chest wall and axillary region followed by post-neoadjuvant chemotherapy with capecitabine and has been in complete remission since completion of the treatment.
Although it remains unclear why no primary tumor can be detected in CUP syndrome, immunological rejection has been discussed as a potential mechanism. Tumor-infiltrating lymphocytes are frequently found and associated with smaller tumor size and better prognosis in triple-negative breast cancer, a molecularly heterogeneous disease with poor outcome (Loi et al. 2019; Schmid et al. 2020). Interestingly, triple-negative breast cancer primary tumors contain more tumor-infiltrating lymphocytes and express lower programmed death ligand 1 (PD-L1) levels than lymph node metastases derived thereof, which indicates that immune escape plays a role in tumor progression (Ogiya et al. 2016; Li et al. 2018). Accordingly, lymph node metastases of our patient contained only few, strongly PD-L1-expressing tumor-infiltrating lymphocytes with a combined positive score (CPS) of 20%.
Together, this case represents a rare occasion to document that favorable subtype CUP syndrome of women with isolated axillary lymph node metastases may indeed derive from adenocarcinoma of the breast.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 1340 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Krämer A Bochtler T Pauli C Cancer of unknown primary: ESMO clinical practice guideline for diagnosis, treatment and follow-up ☆Ann Oncol 20233422824610.1016/j.annonc.2022.11.01336563965 · doi ↗ · pubmed ↗
- 2Li M Li A Zhou S Heterogeneity of PD-L 1 expression in primary tumors and paired lymph node metastases of triple negative breast cancer BMC Cancer 201818410.1186/s 12885-017-3916-y 29291717 PMC 5748959 · doi ↗ · pubmed ↗
- 3Loi S Drubay D Adams S Tumor-infiltrating lymphocytes and prognosis: a pooled individual patient analysis of early-stage triple-negative breast cancers J Clin Oncol 20193755956910.1200/jco.18.0101030650045 PMC 7010425 · doi ↗ · pubmed ↗
- 4Ogiya R Niikura N Kumaki N Comparison of tumor-infiltrating lymphocytes between primary and metastatic tumors in breast cancer patients Cancer Sci 20161071730173510.1111/cas.1310127727484 PMC 5198965 · doi ↗ · pubmed ↗
- 5Schmid P Cortes J Pusztai L Pembrolizumab for early triple-negative breast cancer NEJM 202038281082110.1056/nejmoa 191054932101663 · doi ↗ · pubmed ↗