Ichthyosiform Lichen Planus Pigmentosus in a 19-Year-Old Male Patient: Case Report
Audi Sugiharto, Julius Gatmaitan, Johannes Dayrit

TL;DR
A 19-year-old male with a rare skin condition showing pigmented patches and thick scales is reported, suggesting a new variant of lichen planus pigmentosus.
Contribution
The paper introduces 'ichthyosiform lichen planus pigmentosus' as a new clinical variant of LPP confirmed by histopathology.
Findings
Histopathological analysis confirmed LPP in both macular and ichthyosiform lesions.
CD68 staining showed similar macrophage density in different lesion types.
The case suggests altered keratinization mechanisms in ichthyosiform LPP lesions.
Abstract
Lichen planus pigmentosus (LPP) is a condition characterized by persistent and asymptomatic brownish-black–to-blue or purple-gray pigmentation, predominantly in the face and sun-exposed areas, commonly in dark-skinned individuals. Several clinical variants of LPP have been reported. However, the ichthyosiform type of LPP has not been reported. We present a 19-year-old male patient who presented with a 7-year history of asymptomatic grayish macules; patches with fine scales on the face, trunk, and upper extremities; and grayish plaques with thick “ichthyosiform” scales on the lower extremities. The diagnosis of LPP was proven by histopathological findings on both the macular and ichthyosiform plaques. Cluster differentiation (CD) 68 stain highlights the same density of pigment-laden macrophages in both the gray macule and the ichthyosiform plaque. The cause of LPP is unknown.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
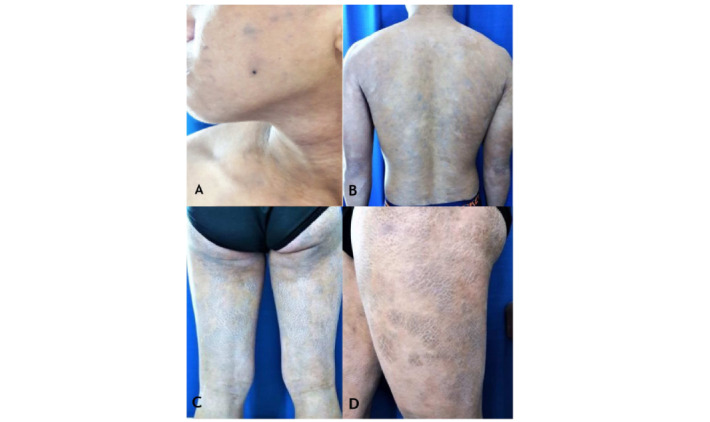 Figure 1
Figure 1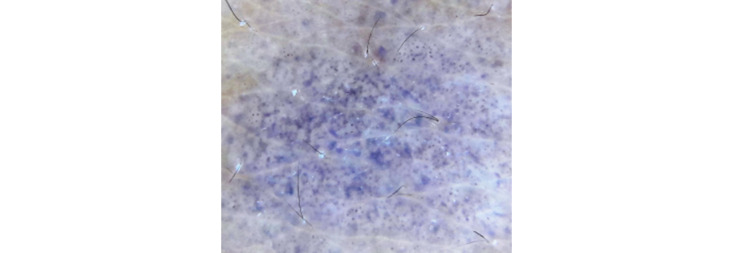 Figure 2
Figure 2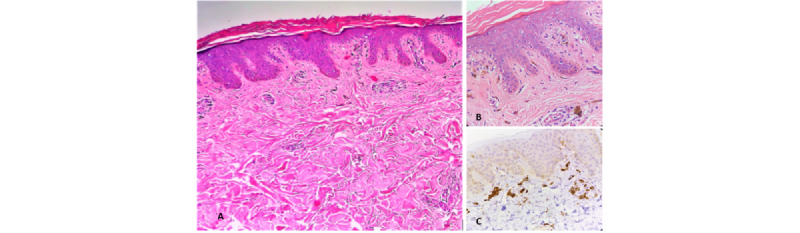 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral Health Pathology and Treatment · melanin and skin pigmentation · Genetic and rare skin diseases.
Introduction
Lichen planus (LP) is an inflammatory disorder affecting skin, mucous membranes, nails, and hair with prototypic “lichenoid” papules. LP has a worldwide distribution with incidence varying from 0.22% to 1% depending on the geographic location [1]. LP can involve the skin or mucous membranes (oral, vulvovaginal, esophageal, laryngeal, and conjunctival mucosa). This condition has different variants based on the morphology of the lesions and the site of involvement [2].
Subtypes based on the configuration or morphology of the lesions include the following: popular (classic), hypertrophic, vesiculobullous, actinic, annular, atrophic, linear, follicular, and LP pigmentosus (LPP) [2]. LPP is a variant of LP characterized by hyperpigmented macules in sun-exposed areas and flexures of dark-skinned individuals [3]. The pigmentation is dermal and occurs without any clinical evidence of inflammation [3].
The cause of LPP is unknown. The diffuse and symmetric classical type, linear unilateral hyperpigmentation in the extremities (Blaschkoid), and segmental patterns on the trunk have been documented. Reticular, blotchy, perifollicular, annular, and gyrate patterns are also encountered [4]. Another rare variant of LPP, that is, LPP inversus located on skinfold areas, has also been reported [5]. However, ichthyosiform variant of LPP has not been reported.
Case Report
A 19-year-old Filipino male patient presented with a 7-year history of asymptomatic grayish macules; patches with fine scales on the face, trunk, and upper extremities (Figure 1A and 1B); and grayish plaques with “ichthyosiform” scales on the lower extremities (Figure 1C and 1D).
We used a manual polarized light device (Dermlite DL3x10, 3Gen). The dermoscopic finding shows dots and globules in a “hem-like” and reticular pattern, which spares the follicular opening (Figure 2).
A 4-mm skin punch biopsy was performed on 2 separate sites (the macule and the ichthyosiform plaque). Histopathology of the ichthyosiform plaque revealed hyperkeratosis and hypergranulosis of the stratum corneum with acanthosis and multifocal areas of vacuolar alteration of the basal cell layer. Histopathology results of both specimens presented with numerous pigment-laden macrophages and mild perivascular inflammatory infiltrate of lymphocytes in the dermis (Figure 3A and 3B). Cluster differentiation (CD) 68 immunostaining highlights the same density of pigment-laden macrophages in both the gray macule and the ichthyosiform plaque (Figure 3C). Definitive diagnosis of LPP was proven by histopathological findings on both the macule and ichthyosiform plaque.
Direct immunofluorescence of the 4-mm skin punch biopsy from the lesional area of the right arm revealed negative results. Serial sections showed no immunofluorescence for immunoglobulin (Ig) A, IgG, IgM, and complement C3 and fibrinogen for epidermis, basement membrane zone, and vascular areas.
Clinical findings: “asymptomatic grayish macules; patches with fine scales on the face (A), trunk, and upper extremities (B); and grayish plaques with thick “ichthyosiform” scales on the lower extremities (C and D).
Dermoscopy shows black dots and globules in a “hem-like” and reticular pattern (Dermlite DL3 polarized dermoscopy).
Histopathology of the ichthyosiform gray plaque shows (A) epidermal hyperkeratosis and hypergranulosis with acanthosis and multifocal areas of vacuolar alteration of the basal cell layer (H&E×100). (B) Numerous pigment-laden macrophages and mild perivascular inflammatory infiltrate of lymphocytes can be appreciated from the dermis (H&E×400). (C) CD68 immunostaining highlights the large pigment-laden macrophages on the biopsy of the ichthyosiform plaque (CD68×400). CD: cluster differentiation; H&E: hematoxylin and eosin.
Discussion
LPP is a rare variant of LP that is seen in individuals with darker pigmented skin [3,4]. The etiology of this condition still remains unknown, but a number of agents have been reported to act as predisposing factors [4]. In 2014, a global consensus statement on acquired macular pigmentation of uncertain etiology concluded that LPP is unlikely to be caused by sociocultural practices or particular dietary ingredients [6].
The occurrence of this condition primarily in sun-exposed areas in numerous patients has led to the proposition that sunlight may be a principal etiological agent [4]. Clinical manifestations of LPP lesions can be found in sun-exposed areas as well as non–sun-exposed areas [6]. For the sites of predilection, LPP involves the head and neck region in most cases followed by the involvement of flexural area, particularly the axillae [6]. Although rare, the involvement of sun-protected areas such as trunk and thigh has also been reported [3,7], similar to our patient.
A number of other variants such as localized LPP (on thigh), segmental LPP, LPP inversus at the skinfold area, linear LPP, LPP in zosteriform distribution, LPP along lines of Blaschko, and LPP of oral mucosa have been reported [4]. Reticular, blotchy, perifollicular, annular, and gyrate patterns were also encountered [4]. LPP with an ichthyosiform pattern similar to our patient has not been reported.
LPP manifests as pigmentation of insidious onset without any features of inflammation or preceding raised lesions. It is typically asymptomatic and may occasionally be accompanied by mild pruritus. The course is variable, with some cases showing spontaneous resolution within weeks to months. It may be persistent over the years in many [3].
Dermoscopy of LPP lesions revealed pigmentation in different nonspecific patterns. These dotted patterns described as fine or coarse blue-gray dots correspond to melanophages in the dermis. Mixed patterns correspond to lesions showing both epidermal and dermal components. In our case, dermoscopy shows dots and globules in a “hem-like” and reticular pattern similar to the findings of Mathews et al [3].
Histologic features of LPP and LP are similar [3,8]. LPP is characterized by interface dermatitis with dense lichenoid reaction in the dermis with pigmentary incontinence and the presence of melanophages [3,7]. The inflammatory phase is characterized by a dense band of lymphohistiocytic inflammatory infiltrate in the upper dermis with prominent basal vacuolar degeneration. Some melanin incontinence is seen with scattered dermal melanophages [3]. These findings are compatible with our patient’s histopathological findings that are more compatible with LPP. In classic LP, additional findings of wedge-shaped hypergranulosis, saw-toothing of the rete ridges, colloid bodies, and a more prominent lichenoid inflammatory infiltrate of lymphocytes are further observed [9].
LPP is considered as a variant of LP [3]. It has a well-described association with classical lesions of LP [3,8]. The pathogenesis of LPP is not yet widely known but postulated to be secondary to type IV hypersensitivity reaction or T-lymphocyte–mediated cytotoxic activity against basal keratinocytes [3,5]. It has been proposed that barrier impairment may be a preceding event in the pathogenesis of LP, or it may occur as a secondary effect resulting from a disturbance in keratinocyte differentiation. A number of studies also revealed that certain transcription factors in LP increased expression of the differentiation-related genes involucrin, filaggrin, and loricrin, which play a role in the keratinization of cutaneous LP lesions [10]. Altered distribution of filaggrin was also observed in patients with LP in other cited literatures [11]. Taking into consideration all the possible pathogenesis of the condition, it is safe to assume that the mechanism of the altered distribution of keratinization in ichthyosiform LPP is similar to what we found in this patient.
The complex relationship between keratinization abnormalities and cutaneous inflammatory illnesses is highlighted by the appearance of ichthyosiform plaques in LPP lesions. Rigid clinicopathological connection and increased dermatologist awareness of this rare clinical presentation are necessary for an accurate diagnosis. In conclusion, the terminology “ichthyosiform lichen planus pigmentosus” is hereby proposed to be added to the clinical variants of LPP. A case series of ichthyosiform LPP is further recommended to confirm this new terminology.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Parihar A Sharma S Bhattacharya SN Singh URA clinicopathological study of cutaneous lichen planus J Dermatol Dermatol Surg 2015011912126 10.1016/j.jssdds.2013.12.003 · doi ↗
- 2Gorouhi F Davari P Fazel N Cutaneous and mucosal lichen planus: a comprehensive review of clinical subtypes, risk factors, diagnosis, and prognosis Scientific World Journal 2014201474282610.1155/2014/74282610.1155/2014/7428262467236224672362 PMC 3929580 · doi ↗ · pubmed ↗
- 3Mathews I Thappa DM Singh N Gochhait D Lichen planus pigmentosus: a short review Pigment Int 201831510 10.4103/2349-5847.184265 · doi ↗
- 4Ghosh A Coondoo A Lichen planus pigmentosus: the controversial consensus Indian J Dermatol 2016615482486 10.4103/0019-5154.19010827688435 IJD-61-48227688435 PMC 5029231 · doi ↗ · pubmed ↗
- 5Barros H Rde Almeida JRP Mattos e Dinato SL Sementilli A Romiti N Lichen planus pigmentosus inversus An Bras Dermatol 2013886 Suppl 1146149 10.1590/abd 1806-4841.2013259924346904 S 0365-0596201300080014624346904 PMC 3876001 · doi ↗ · pubmed ↗
- 6Kumarasinghe SPW Pandya A Chandran V Rodrigues M Dlova NC Kang HY Ramam M Dayrit JF Goh BK Parsad DA global consensus statement on ashy dermatosis, erythema dyschromicum perstans, lichen planus pigmentosus, idiopathic eruptive macular pigmentation, and Riehl's melanosis Int J Dermatol 201958326327210.1111/ijd.141893017605530176055 · doi ↗ · pubmed ↗
- 7Hong S Shin JH Kang HY Two cases of lichen planus pigmentosus presenting with a linear pattern J Korean Med Sci 2004191152154 10.3346/jkms.2004.19.1.1521496636120040215214966361 PMC 2822256 · doi ↗ · pubmed ↗
- 8Bhat RM Mathanda TR Jayaprakash CS Dandakeri S Clinical, histopathological characteristics and immunohistochemical findings in lichen planus pigmentosus Indian J Dermatol 2017626612617 10.4103/ijd.IJD_148_1729263535 IJD-62-61229263535 PMC 5724309 · doi ↗ · pubmed ↗