Successful transcatheter mitral paravalvular leak closure complicated with stuck mechanical valve and device migration
Kenta Yoshida, Shunsuke Kubo, Takeshi Maruo, Kazushige Kadota

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
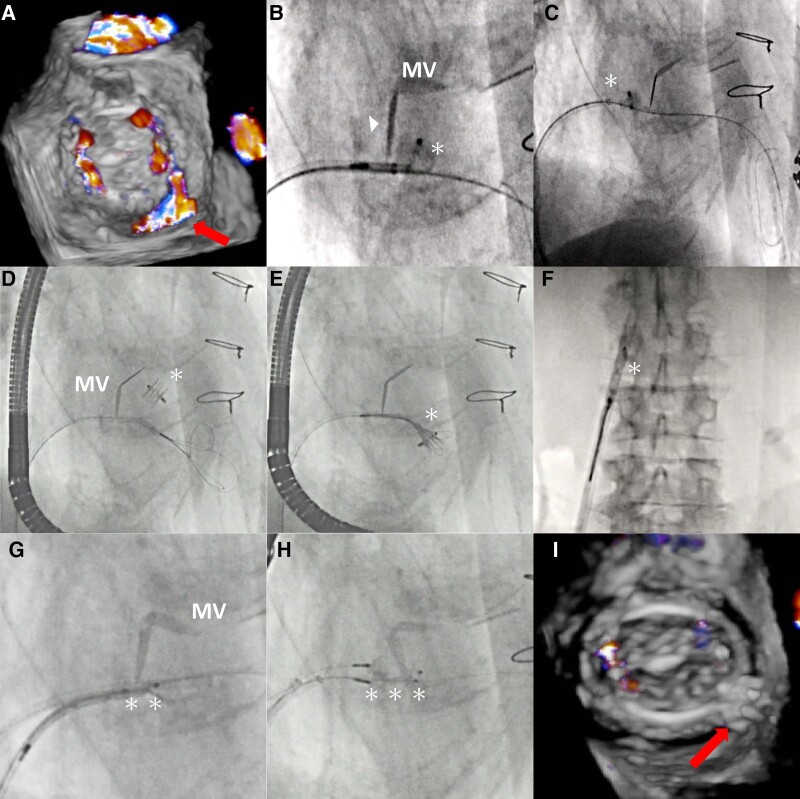 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management · Atrial Fibrillation Management and Outcomes
An 80-year-old man who underwent mitral and aortic mechanical valve replacement 27 years ago presented with haemolytic anaemia and heart failure. Transoesophageal echocardiogram (TEE) confirmed severe eccentric mitral paravalvular leak (PVL) (Figure 1A, Supplementary material online, Video S1). We performed transcatheter PVL closure using Amplatzer Vascular Plug II (AVP II, Abbott Vascular, IL).
Using the retrograde transseptal approach, a 10 mm AVP II was implanted in the PVL through a 6 Fr Destination sheath (Terumo, Japan). Because the device interfered with the mechanical valve leaflet, it was deployed more proximally (Figure 1B and C). After the PVL decreased to moderate, another device was tried to be added. When the sheath was re-advanced to the left ventricle (LV), the first device dislodged and moved to the LV (Figure 1D, Supplementary material online, Video S2). Then, a 7 Fr JR 4.0 guide catheter with an EN snare (Merit Medical, UT) was inserted into the LV through the PVL. After several attempts, the device was successfully snared and retrieved (Figure 1E and F). Using a 12 mm AVP II was difficult as it caused a stuck mechanical valve (Figure 1G). Therefore, two downsized 8 mm AVP II devices were deployed after the insertion of two 6 Fr Destination sheaths. The device’s distal disk interfered the mechanical valve leaflet, but it partially opened (Figure 1H, Supplementary material online, Video S3). With a mean mitral valve pressure of 4 mmHg, TEE didn’t display significant mitral stenosis, and the PVL had nearly disappeared (Figure 1I, Supplementary material online, Video S4). After confirming stability, the devices were released. The patient was uneventfully discharged 8 days following the procedure.
Device migration and stuck mechanical valve are important complications of PVL closure.^1^ Learning points of this case are follows: (1) the device migrated to the LV can be retrieved through the mitral PVL; and (2) when the device interferes the mechanical valve leaflet, the mechanical valve function can be preserved if the leaflet partially opens.
Supplementary Material
ytae187_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.