A Systematic Review and Meta-Analysis of the Cancer-Related and Functional Outcomes of High-Intensity Focused Ultrasound, Open Radical Prostatectomy, Robot Assisted Radical Prostatectomy, and External Beam Radiation Therapy in Primary Treatment of Localized Low- or Intermediate-Risk Prostate Cancer
Bassem Toeama, Emmanuel Papadimitropoulos, Nathan Perlis, Paul Grootendorst, Bassem Hamandi

TL;DR
This study compares the effectiveness and side effects of four prostate cancer treatments for localized low- or intermediate-risk cases.
Contribution
The paper provides a systematic review and meta-analysis comparing HIFU, ORP, RARP, and RT for prostate cancer treatment.
Findings
ORP showed better 5-year failure-free survival than RT.
ORP had lower urinary incontinence rates than RARP at 1 year.
RARP had better erectile function outcomes than ORP at 1 year.
Abstract
Prostate cancer is the second- leading cause of cancer death among men. We aimed to evaluate high-intensity focused ultrasound (HIFU), open radical prostatectomy (ORP), robot-assisted radical prostatectomy (RARP), and external beam radiation therapy (RT) in the treatment of localized low- and intermediate-risk prostate cancer. We searched bibliographic databases for case–control, cohort, and randomized controlled studies. We used MeSH subject headings and free text terms for prostate cancer, HIFU, ORP, RARP, RT, failure-free survival (FFS), biochemical disease-free survival (BDFS), urinary incontinence (UI), and erectile dysfunction (ED). Fourteen studies were included in the review, for a total of 34 927 participants. Among the 8 studies of HIFU as the primary treatment of localized low- and intermediate-risk prostate cancer, 4 studies reported 5-year FFS rates ranging from 67.8% to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1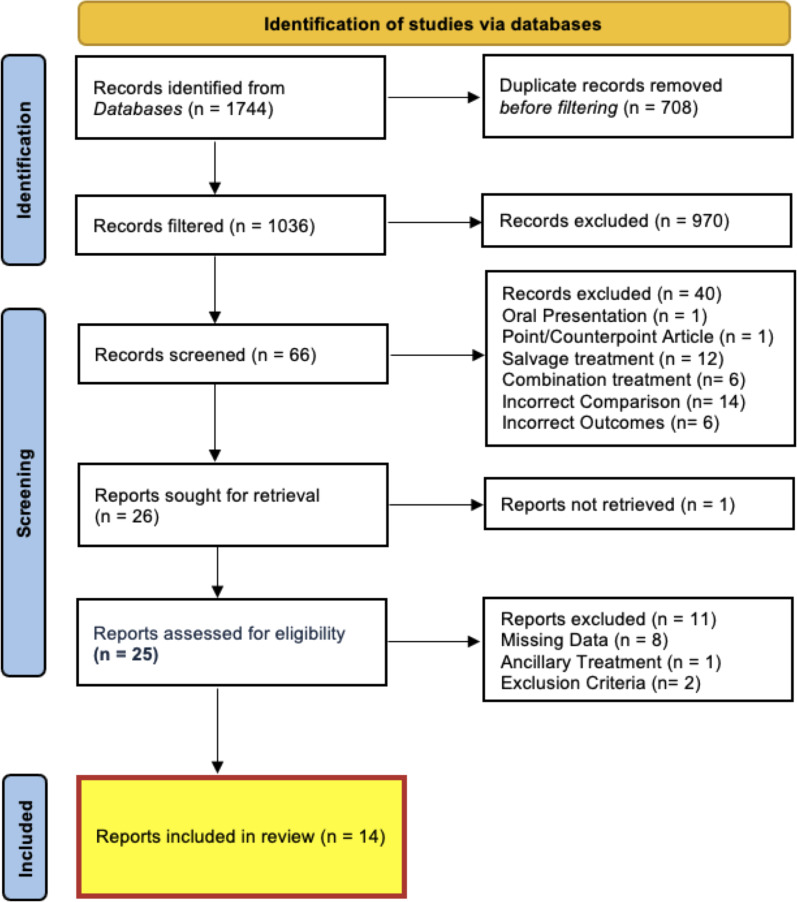 Figure 2
Figure 2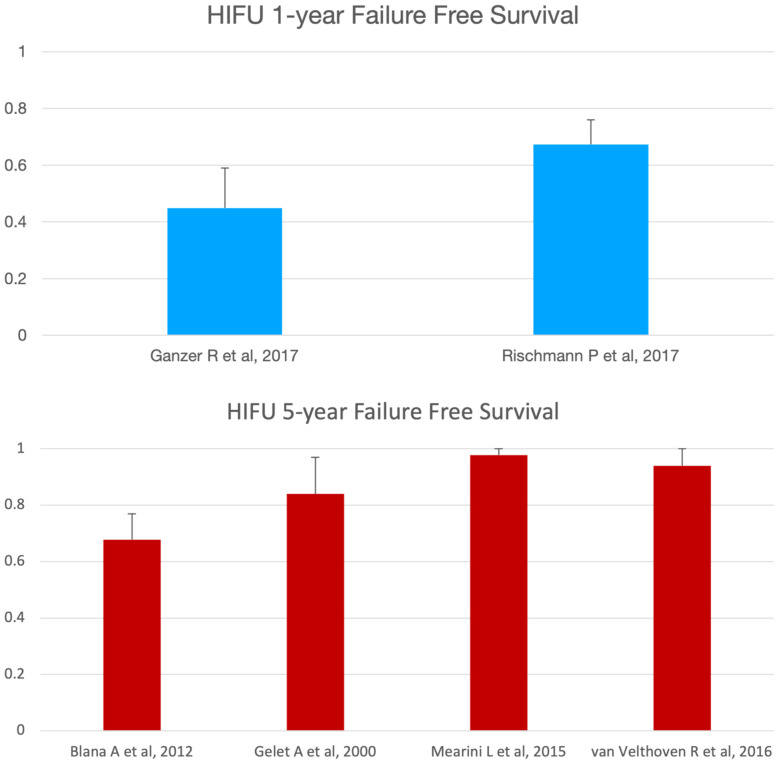 Figure 3
Figure 3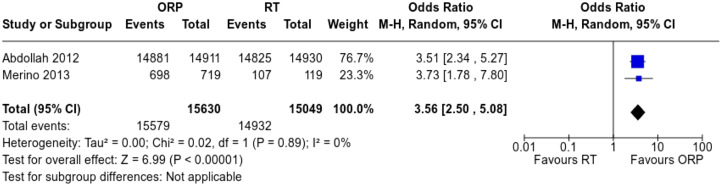 Figure 4
Figure 4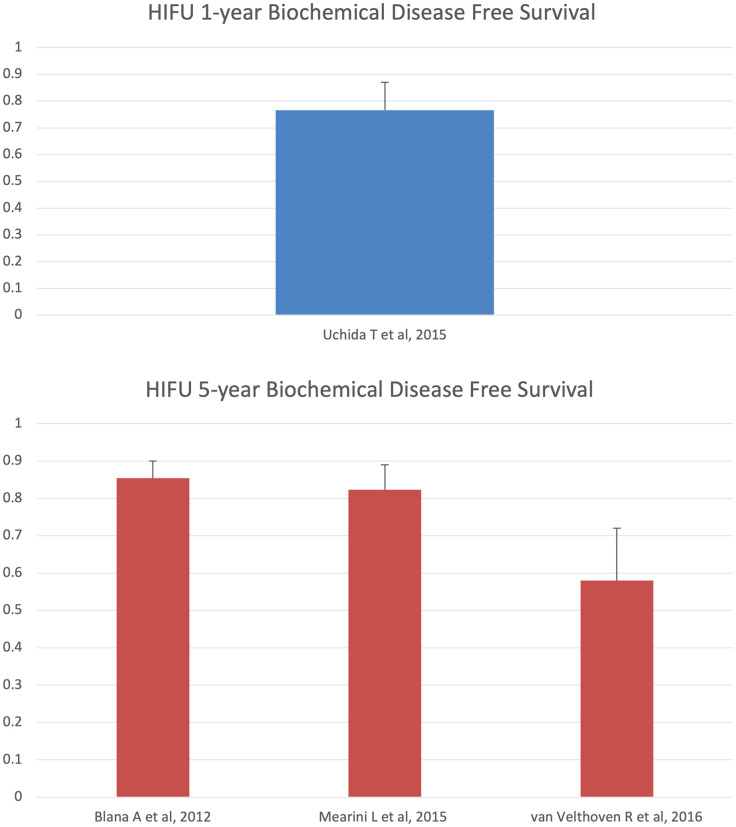 Figure 5
Figure 5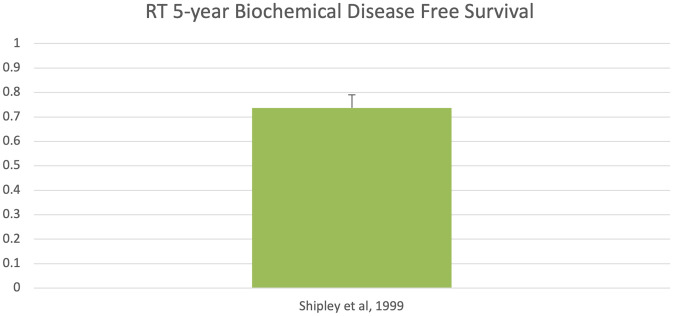 Figure 6
Figure 6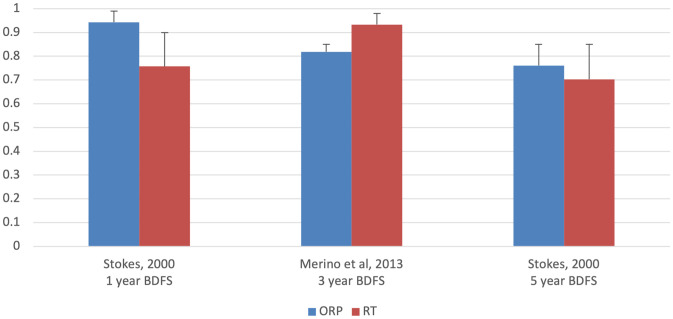 Figure 7
Figure 7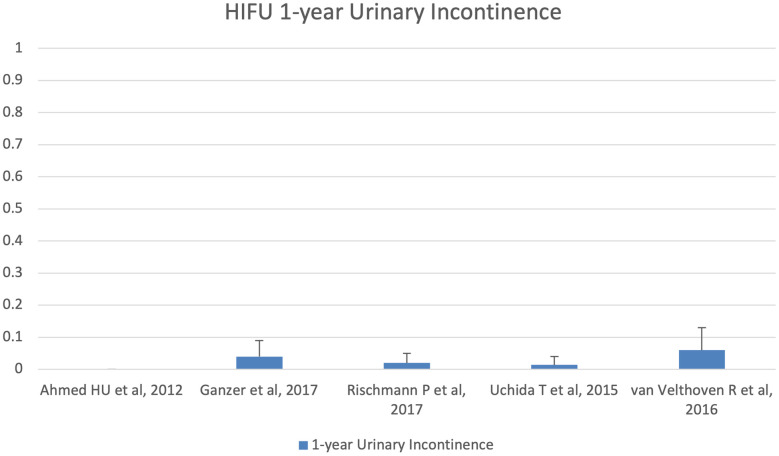 Figure 8
Figure 8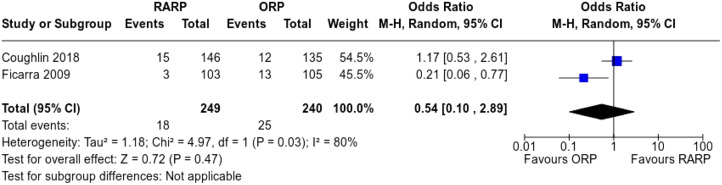 Figure 9
Figure 9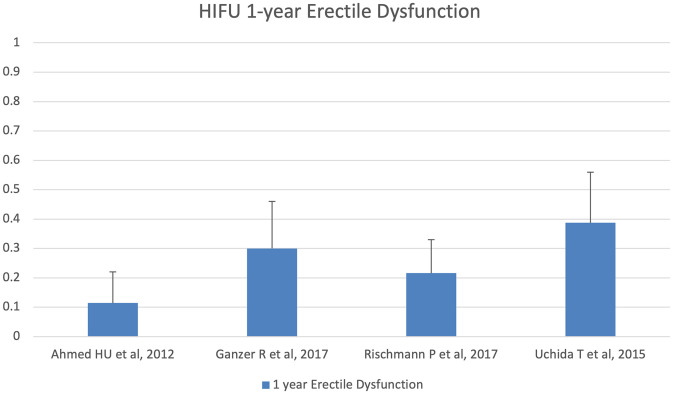 Figure 10
Figure 10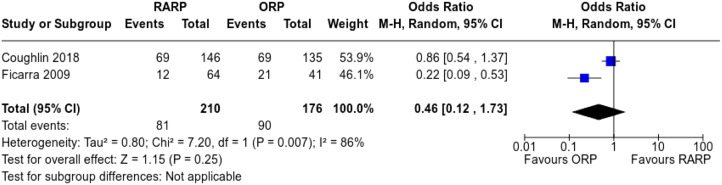 Figure 11
Figure 11Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsProstate Cancer Diagnosis and Treatment · Prostate Cancer Treatment and Research · Radiomics and Machine Learning in Medical Imaging
Introduction
Rationale
Prostate cancer is the most frequently diagnosed male cancer and the third leading cause of death from cancer among Canadian men.^1^ In Canada, 1 in 7 men will have prostate cancer, and 1 in 27 will die of it.^2^ There are different stages of prostate cancer that range from localized through locally advanced to advanced. Localized prostate cancer is confined to the prostate gland and does not grow into nearby tissues with clinical tumor node metastasis (TNM) stages cT1-T2 N0 M0 at presentation.^3^ Localized prostate cancer is further classified into low-, intermediate-, and high-risk groups of recurrence following radical treatment according to pretreatment variables of prostate-specific antigen (PSA), Gleason score, and clinical T stage. The low-risk group has pretreatment variables of PSA <10 ng/mL, Gleason score ≤6, and clinical T stages cT1c-T2a, while the intermediate-risk group has pretreatment variables of PSA 10-20 ng/mL, Gleason score 7, or clinical T stage cT2b.^4^ According to the Canadian Cancer Society (CCS) guidelines, open radical prostatectomy (ORP), robot-assisted radical prostatectomy (RARP), external beam radiation therapy (RT), and active surveillance are the main lines of primary treatment for localized low- and intermediate-risk prostate cancer.^5^ In the UK, the Urological Cancer Care Pathway Development Group of Aberdeen recommended ablative focal therapies as alternative strategies for treating localized low- and intermediate-risk prostate cancer.^6^ Ablative focal therapies include brachytherapy, cryotherapy, high-intensity focused ultrasound (HIFU), laser therapy, radiofrequency ablation, and photodynamic therapy. The European Association of Urology (EUA) has strongly recommended HIFU within clinical trials or registries for treatment of localized intermediate-risk prostate cancer, and the USA FDA approved HIFU for treatment of localized low- and intermediate-risk prostate cancer in October 2015.^7^
Objectives
We aimed to evaluate the cancer-related and functional outcomes, including the 1-, 3-, and 5-year failure-free survival (FFS) rates, 1-, 3-, and 5-year biochemical disease-free survival (BDFS) rates, 1-year urinary incontinence (UI) rate, and 1-year erectile dysfunction (ED) rate, of HIFU, ORP, RARP, and RT in primary treatment of localized low- and intermediate-risk prostate cancer.
Material and Methods
The introduction, methods, results, and discussion sections were performed following the Cochrane Handbook for Systematic Reviews of Interventions and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 27-item checklist.^8,9^ The PRISMA 27-item checklist is presented in the supplementary materials.
Eligibility Criteria
The filters used in the systematic review were humans, males, age ≥ 18 years, and clinical trials. The eligible clinical trials included case–control, cohort, and randomized controlled studies. Participants in the eligible clinical trials were male patients ≥ 18 years with histologically confirmed adenocarcinoma of the prostate. Screened studies were included if the participants had localized prostate cancer TNM stage cT1-T2 N0 M0 and low- or intermediate-risk of recurrence with pretreatment variables of PSA ≤20 ng/mL and Gleason score ≤7, the participants had not received any previous treatment for prostate cancer (including hormonal therapy, radiation therapy, surgery, or chemotherapy), and the participants were candidates for primary treatment with HIFU, ORP, RARP, or RT. Screened studies were excluded if the participants had locally advanced or metastatic prostate cancer TNM stage cT3 ± N1 ± M1 or the participants had a high risk of recurrence with pretreatment variables of PSA >20 ng/mL ± Gleason score >7, or the participants had received previous treatment for prostate cancer (including surgery, hormonal therapy, radiation therapy, or chemotherapy).
Information Sources
We searched bibliographic databases from inception through August 31, 2021, for all relevant published case–control, cohort, and randomized controlled studies that investigated the cancer-related and functional outcomes of HIFU, ORP, RARP, and RT as primary lines of treatment for localized low- and intermediate-risk prostate cancer. Medline, Embase, and Cochrane databases were accessed via PubMed, Ovid, and Wiley interfaces, respectively.
Search Strategy
The Patient, Intervention, Comparator, Outcome, Time, Study Type (PICOTS) model was applied to identify key topics that determined the systematic review search strategy. Patients had prostate cancer, the intervention was HIFU, ORP, RARP, or RT, the comparator was HIFU, ORP, RARP, RT, or no comparator, the outcomes were FFS rate, BDFS rate, UI rate, and ED rate, the time of data collection was at 1, 3, and 5 years for the FFS and BDFS rates and at 1 year for the UI and ED rates, and the study type was case–control, cohort, and randomized controlled studies. We mapped MeSH-controlled terms (subject headings) and searched keyword terms (synonyms) for the PICOTS components. We used truncation and search tags for the controlled terms (subject headings) and the keyword terms (synonyms), grouped controlled and keyword terms together using the Boolean AND or OR, and considered how final sets will be grouped together using the Boolean AND or OR Supplement 1: [https://docs.google.com/document/d/17mLpMjjLztTaZ8fTAX6Y5zILTilYTRFBfv3dnT1m1rA/edit?usp=sharing].
Selection and Data Collection Process
The systematic review was performed by 2 independent reviewers, where studies were identified via databases, deduplicated, filtered, screened against inclusion and exclusion criteria, assessed for eligibility, and selected for the systematic review.
Data Items
The studies selected for the systematic review evaluated cancer-related and functional outcomes, including the 1-, 3-, and 5-year FFS rates, 1-, 3-, and 5-year BDFS rates, 1-year UI rate, and 1-year ED rate of HIFU, ORP, RARP, and RT in primary treatment of localized low- and intermediate-risk prostate cancer. Failure-free survival is either the time from randomization or the time from primary treatment to the first of the following events: progression either locally, in lymph nodes, or in distant metastases, or death from prostate cancer. Failure-free survival includes disease-free survival, progression-free survival, metastasis-free survival, relapse-free survival, or cancer-specific survival. Biochemical disease-free survival is either the time from randomization or the time from primary treatment to PSA level ≥ 0.2 ng/mL following radical prostatectomy, PSA level ≥ 2 ng/mL above nadir PSA following radiation therapy, or PSA level ≥ 1.2 ng/mL above nadir following HIFU.^10^ Biochemical disease-free survival is also known as biochemical relapse-free survival, biochemical recurrence-free survival, biochemical failure-free survival, or PSA-failure-free survival. Urinary incontinence is the leaking of urine following HIFU, ORP, RARP, or RT, requiring the use of ≥ 1 pad per day. Urinary incontinence is also known as stress incontinence, urge incontinence, overflow incontinence, or mixed incontinence. Erectile dysfunction is the inability to achieve and sustain an erection following HIFU, ORP, RARP, or RT, sufficient for sexual intercourse. Erectile dysfunction is also known as impotence or sexual dysfunction.
Study Risk of Bias Assessment and Reporting Bias Assessment
Reviewers followed the Newcastle–Ottawa Scale (NOS) for cohort studies, the revised Cochrane Risk of Bias tool for randomized trials (ROB 2), and the Risk of Bias in Non-randomized Studies – of Interventions (ROBINS-I) tool to identify studies at high risk of bias, and differences were resolved through discussion.
Synthesis Methods and Effect Measures
Descriptive characteristics, including anthropometric data (weight, height, and body mass index), sociodemographic data (age, race, and ethnicity), and medical history and comorbidity data such as hypertension, diabetes, and heart disease have been balanced in some studies with active comparators and imbalanced in others. The prostate cancer characteristics, such as the PSA, Gleason score, and clinical T stage, have been balanced in studies with active comparators. The assessment outcomes of the studies lacking active comparators were analyzed with Excel’s Data Analysis Toolpak using maximum likelihood estimation and reported as point estimate (ˆp), while the assessment outcomes of the randomized and non-randomized studies with active comparators were analyzed with Cochrane Tools using a random-effects model with Mantel–Haenszel (M-H) estimator for Tau^2^ statistic and reported as odds ratio (OR). Quantitative (continuous) data were represented as means and SDs, while qualitative (categorical) data were represented as frequencies and percentages.^11,12^
Certainty Assessment
The confidence interval was set to 95% by the normal approximation method, and the margin of error accepted was set to 5%.
Results
Study Selection
A total of 1744 studies were identified via databases. Seven hundred eight duplicate studies were detected. After deduplication, 1036 unique studies were cross-checked against the filters. Nine hundred seventy studies were removed because they did not have the sought filters. The remaining 66 studies were reviewed against the inclusion/exclusion criteria. Forty studies did not meet the inclusion/exclusion criteria, and the remaining 26 studies were sought for retrieval. One study was not retrieved, and out of the 25 studies that were retrieved, 11 reports were excluded because of missing data, ancillary treatment, and exclusion criteria. Only 14 studies were included in the systematic review (1 study evaluated HIFU for focal ablation of the prostate, 3 studies evaluated HIFU for hemiablation of the prostate, 4 studies evaluated HIFU for whole-gland ablation of the prostate, 2 studies compared ORP vs. RARP, 3 studies compared ORP vs. RT, and 1 study evaluated RT of the prostate). These studies used a total of 34 927 participants. The PRISMA flow chart reflecting the identification of studies via databases, deduplication, screening, and assessment for eligibility is presented in Figure 1.
Study Characteristics
The key features, descriptive characteristics, and prostate cancer risk characteristics of the included studies are presented in Tables 1and2, respectively.
Risk of Bias in Studies and Reporting Biases
We examined the quality of evidence for each outcome according to NOS for cohort studies, the ROB 2 tool for randomized trials, and the ROBINS-I tool for non-randomized studies. The overall quality of evidence for each outcome was determined to be high, moderate, low, or very low, as presented in Supplement 2.^13^
Results of Individual Studies, Results of Syntheses, and Certainty of Evidence
Failure-Free Survival
Among the 8 studies of HIFU as the primary treatment of localized low- and intermediate-risk prostate cancer, 2 studies reported 1-year FFS survival rates of 44.9% and 67% (ˆp = 0.449-0.673; 95% CI, 0.31-0.76), and 4 studies reported 5-year FFS rates ranging from 67.8% to 97.8% (ˆp = 0.678-0.978; 95% CI, 0.58-1) (Figure 2). In addition, our search revealed a 5-year FFS rate favoring ORP compared to RT (OR = 3.56; 95% CI, 2.50-5.08) (Figure 3).
Biochemical Disease-Free Survival
Among the 8 studies of HIFU as the primary treatment of localized low- and intermediate-risk prostate cancer, 1 study reported a 1-year BDFS rate of 76.6% (ˆp = 0.766; 95% CI, 0.66-0.87) and 3 studies reported a 5-year BDFS rates ranging from 58% to 85.4% (ˆp = 0.58-0.854; 95% CI, 0.44-0.9) (Figure 4). In addition, our search revealed 1 RT study which reported 5-year BDFS rate of 73.7% (ˆp = 0.737; 95% CI, 0.67-0.79) (Figure 5), 1 ORP vs. RT study which reported a 1-year BDFS rate of 94.3% vs. 75.7% (ˆp = 0.943 vs. 0.757; 95% CI: 0.89-0.99 vs. 0.62-0.90) and 5-year BDFS rate of 76.1% vs. 70.3% (ˆp = 0.761 vs. 0.703; 95% CI, 0.67-0.85 vs. 0.56-0.85), and 1 ORP vs. RT study which reported a 3-year BDFS rate of 81.9% vs. 93.3% (ˆp = 0.819 vs. 0.933; 95% CI, 0.79-0.85 vs. 0.89-0.98), respectively (Figure 6).
Urinary Incontinence
Among the 8 studies of HIFU as the primary treatment of localized low- and intermediate-risk prostate cancer, 5 studies reported 1-year UI rates ranging from 0% to 6% (ˆp = 0-0.06; 95% CI, 0.0-0.13) (Figure 7). In addition, our search revealed 1-year UI rate favoring ORP compared to RARP (OR = 0.54; 95% CI, 0.10-2.89) (Figure 8).
Erectile Dysfunction
Among the 8 studies of HIFU as the primary treatment of localized low- and intermediate-risk prostate cancer, 4 studies reported 1-year ED rates ranging from 11.4% to 38.7% (ˆp = 0.114-0.387; 95% CI, 0.01-0.56) (Figure 9). In addition, our search revealed 1-year ED rate favoring ORP compared to RARP (OR = 0.46; 95% CI, 0.12-1.73) (Figure 10).
Discussion
As per the CCS and the National Comprehensive Cancer Network (NCCN) guidelines, primary treatment of localized low- and intermediate-risk prostate cancer includes active surveillance, watchful waiting, and radical local therapy (surgery and radiation therapy). Alternative focal therapy is not included in the CCS and NCCN guidelines for primary treatment of localized low- and intermediate-risk prostate cancer. The National Institute for Health and Excellence recommends using alternative focal therapy for localized prostate cancer. We conducted a systematic review and meta-analysis to compare up-to-date efficacy, safety, and functional outcomes of the second-line alternative focal therapy represented by HIFU versus up-to-date efficacy, safety, and functional outcomes of the first-line standard of care (radical local therapy) represented by ORP, RARP, and RT in the primary treatment of localized low- and intermediate-risk prostate cancer. Our systematic review showed single-arm cohort studies that lacked comparison of HIFU with the standard of care. There are 2 prospective, multicenter, single-arm cohort studies that reported HIFU 1-year FFS rates of 44.9% and 67%,^14,15^ 4 single-arm cohort studies that reported HIFU 5-year FFS rates ranging from 67.8% to 97.8%,16-19 1 prospective, multicenter, single-arm cohort study that reported HIFU 1-year BDFS rate of 76.6%,^19^ 3 single-arm cohort studies that reported HIFU 5-year BDFS rates ranging from 58% to 85.4%,^16,18,19^ 5 single-arm cohort studies that reported HIFU 1-year UI rates ranging from 0% to 6%,^14,15,19,20,21^ and 4 single-arm cohort studies that reported HIFU 1-year ED rates ranging from 11.4% to 38.7%.^14,15,20,21^ In addition, our systematic review showed randomized and non-randomized studies with active comparators comparing ORP to RT and ORP to RARP. Meta-analysis indicated a 5-year FFS favoring ORP compared to RT (OR = 3.56; 95% CI, 2.50-5.08),^22,23^ 1-year UI rate favoring ORP compared to RARP (OR = 0.54; 95% CI, 0.10-2.89), and 1-year ED rate favoring ORP compared to RARP (OR = 0.46; 95% CI, 0.12-1.73).^24,25^
Limitations of our systematic review include restrictive eligibility criteria which restrained our search, decreased the number of the studies included in the systematic review, and threatened the external validity of the systematic review, heterogeneous patient populations with variations in descriptive characteristics and prostate cancer risk characteristics, lack of adjustment for the imbalanced descriptive characteristics and prostate cancer risk characteristics leading to sampling error, inconsistency of the therapeutic modality for HIFU and inconsistency of the definitions used for FFS and BDFS which might affect reliability of the results, heterogeneous results which might need further statistical tests for measuring the probability of heterogeneity, and lack of randomization in non-randomized studies with active comparators leading to selection bias.
Prostate cancer is the third leading cause of cancer death among Canadian men.^1^ Open radical prostatectomy, RARP, and RT are 3 main lines of primary treatment for localized low- and intermediate-risk prostate cancer. High-intensity focused ultrasound is an alternative treatment to ORP, RARP, and RT. Real-world evidence studies of HIFU in the primary treatment of localized low- and intermediate-risk prostate cancer are required for public funding of HIFU. There is limited published literature assessing the efficacy, safety, and functional outcomes of HIFU in the primary treatment of localized low- and intermediate-risk prostate cancer. Most of the studies that evaluated the clinical outcomes of HIFU (including efficacy, safety, and functional outcomes) were small, non-randomized, uncontrolled trials. Without sufficient comparative, well-designed studies, policymakers may face challenges in determining the appropriate place of HIFU within the existing treatment algorithm, and patients will find it difficult to engage in the shared decision-making process. Well-designed comparative studies, including large sample-sized, randomized, controlled trials, might help establish the effectiveness and safety of HIFU relative to the standard of care treatment options. In addition, HIFU technology has advanced in the past few years, healthcare providers have become more familiar and skilled with using it, and it has been recently included in the National Institute for Health and Care Excellence guidance for treatment of localized prostate cancer.^26^ The procedure of HIFU has also evolved from whole-gland treatment to focal ablation, and as a result, the adverse events of HIFU have become fewer, and its advantages as organ preservation and short recovery time have gained significance. This might be an add-on supporting clinical decision-making, incorporation into guidelines, and reimbursement for this novel treatment modality.
Our systematic review and meta-analysis revealed a lack of studies with active comparators comparing HIFU to standard of care (ORP, RARP, or RT) in the primary treatment of localized low- and intermediate-risk prostate cancer. Open radical prostatectomy has a favorable efficacy outcomes profile compared to RT, while RARP has a beneficial functional outcomes profile compared to ORP, respectively. Given the burden of prostate cancer, more studies with active comparators comparing HIFU to standard of care (ORP, RARP, or RT) in the primary treatment of localized low- and intermediate-risk prostate cancer should be prioritized for future research. This will generate less heterogeneous data and draw more robust evidence for clinical decision-making, incorporation into guidelines, and reimbursement decisions.
Registration and Protocol Number
Our systematic review protocol has been registered in the International Prospective Register of Systematic reviews, registration number CRD 420337, and can be accessed at https://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42016037337.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1. Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2017. Toronto, ON: Canadian Cancer Society. cancer.ca/Canadian-Cancer-Statistics-2017-EN Accessed July 30, 2019.
- 2. Fradet Y Klotz L Trachtenberg J Zlotta A . The burden of prostate cancer in Canada. Can Urol Assoc J. 2009;3(suppl 2):S 92 S 100. (10.5489/cuaj.1113)PMC 269878219543427 · doi ↗ · pubmed ↗
- 3. Amin MB Edge SB Greene FL , et al. Prostate. In: AJCC Cancer Staging Manual. Amin MB , ed. 8th ed. New York, NY: Springer; 2017.
- 4. D’Amico AV Whittington R Malkowicz SB , et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA. 1998;280(11):969 974. (10.1001/jama.280.11.969)9749478 · doi ↗ · pubmed ↗
- 5. Canadian Cancer Society. Treatments for localized prostate cancer. In: Canadian Cancer Society. Accessed May 30, 2023. https://www.cancer.ca/en/cancer-information/cancer-type/prostate/treatment/localized/?region=on.
- 6. Ramsay CR Adewuyi TE Gray J , et al. Ablative therapy for people with localised prostate cancer: a systematic review and economic evaluation. Health Technol Assess. 2015;19(49):1 490. (10.3310/hta 19490)PMC 478123626140518 · doi ↗ · pubmed ↗
- 7. Nelson R . FDA approves first HIFU device for prostate tissue ablation. In: Medscape. https://www.medscape.com/viewarticle/853120.
- 8. Higgins JPT Thomas J Chandler J , et al., eds. Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane; 2022. www.training.cochrane.org/handbook