Mind the gap! Interdisciplinary approach to anterior chest wall reconstruction after total sternectomy
Olaf Michael Glueck, Denis Ehrl, Rudolf A. Hatz, Jan M. Fertmann

TL;DR
This paper presents a new interdisciplinary surgical method for chest wall reconstruction after sternectomy, showing good patient outcomes and quality of life.
Contribution
A standardized interdisciplinary approach combining titanium bars and muscle flaps for chest wall reconstruction is proposed.
Findings
All patients reported chest wall stability and good quality of life after reconstruction.
Spirometry results showed improved FEV1/FVC post-surgery with no implant defects.
No prolonged pain or lung function impairment was observed in follow-ups.
Abstract
There are various reconstructive methods after total sternectomy. Reproducibility is scarce due to overall small patient numbers. Therefore we present a standardized, interdisciplinary approach for thoracic and plastic surgery. Four patients underwent interdisciplinary chest wall reconstruction with STRATOS® titanium bars and myocutaneous vastus lateralis muscle free flap in our center. All patients reported chest wall stability after reconstruction. They reported good quality of life, no dyspnea, prolonged pain or impairment in lung function from rigid reconstruction. FEV1/FVC was overall better after surgery. Secondary wound healing was not impaired and there was no implant defect in follow up. We recommend an interdisciplinary surgical approach in chest wall reconstruction after total sternectomy. The combination of rigid reconstruction with titanium bars and a myocutaneous vastus…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
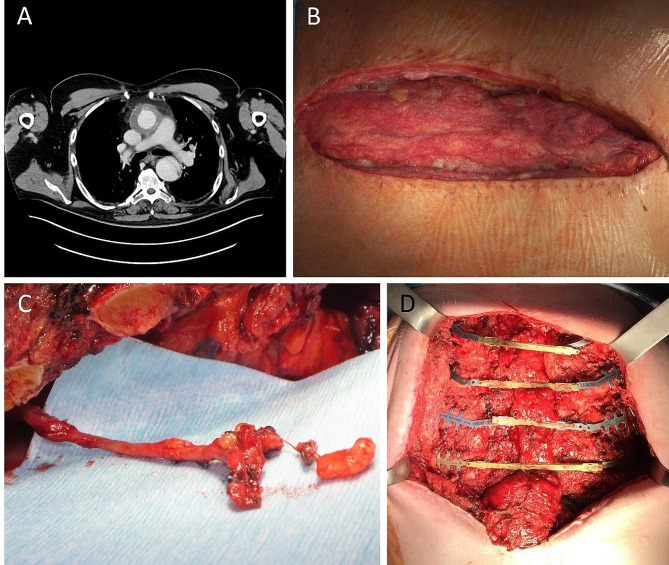 Figure 1
Figure 1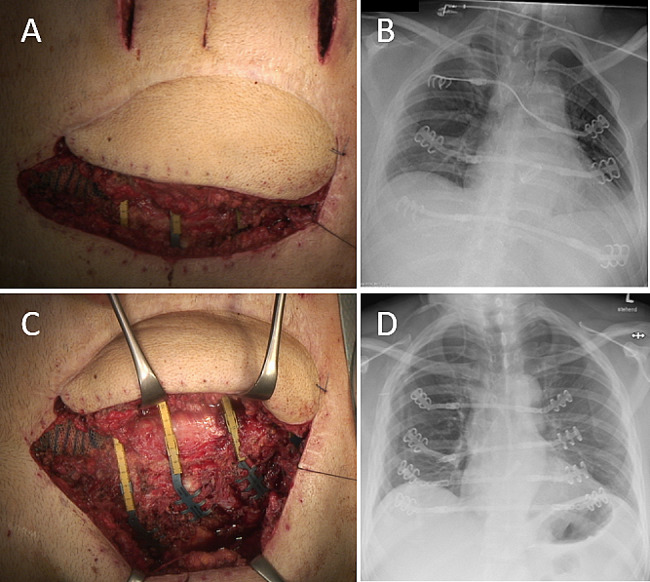 Figure 2
Figure 2 Figure 3
Figure 3- —Universitätsklinik München (6933)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSurgical site infection prevention · Reconstructive Surgery and Microvascular Techniques · Pleural and Pulmonary Diseases
Background
Total sternectomy is rare but can be necessary due to oncological and non-oncologic disease. Most primary and secondary tumors of the anterior chest wall involve only small parts of the sternum, if at all. It is mainly connective tissue tumors like osteosarcoma or chondrosarcoma, or metastasis. Benign sternum destruction is a rare complication in 1–2% after open cardiac or aortic surgery. Small defects can develop to deep sternal wound infections (DSWI) with subsequent osteomyelitis [1, 2]. Failure of less-invasive treatment options leads to the need of total sternectomy and in the following, a robust and aesthetic reconstruction of the anterior chest wall. This is essential for stability, functionality and quality of life [3]. Reconstructive methods range from mesh – methylmethacrylate – mesh sandwiches or titanium mesh grafts to titanium bars and individualized 3D-printed sternum interponates and cadaveric sternal allografts, mostly described in case reports [4–9].
We present a small series of an interdisciplinary reconstructive surgical approach in four patients using titanium bars (STRATOS™, MedXpert GmbH, Eschbach, Germany) and free myocutaneous vastus lateralis muscle flap coverage.
Patients and methods
Ethical statement
All data presented was gathered after approval of the institutional Ethics Committee of the Ludwig-Maximilians University Hospital of Munich (reference no 21–0475). Patients have given consent for use of their images.
We present an interdisciplinary surgical approach in four comparable cases of anterior thoracic wall reconstruction after total sternectomy. Indications were either malignancy or deep sternal wound infection (see Table 1). All patients were male, the mean age was 62,5 years (53–72) at time of surgery. Patient A, B and D underwent various treatments for sternal defect after full or sternectomy before and all patients presented with different sets of comorbidities (Table 1). We performed computed tomography (CT) angiography in all patients for evaluation of target vessels for anastomosis and for thorough surgical planning. All patients underwent spirometric testing before and after surgery. For comparability the FEV1/FVC ratio was used to describe changes in lung function. Furthermore, subjective postoperative breathing mechanics were evaluated by observation and questioning the patients before and after surgery.
Table 1. Demographical data, follow-up and pulmonary function of the selected patientsPatient APatient BPatient CPatient DAge (y)60726553SexmmmmBMI (kg/m²)33.227.226.735.0Cause of defectaortic arch replacementtriple bypassNSCLCaortic valve replacementtraffic accidentSternal defectDSWIDSWIsternum metastasisDSWIPretreatmentsternal rewiringomental interpositioningomental interpositioningleft upper lobe lobectomychest wall resectionsternal rewiringsternal osteosynthesisComorbiditiesarterial hypertension OSASatrial fibrillationdepressionrenal replacement therapyIDDMNSCLCrenal insufficiencyOSAShepatic steatosisIDDMRevision surgerynonesecondary wound closurenoneSTRATOS bar replacementICU stay (d)21814Hospital stay (d) overall vs. post surgery10/922/1442/2925/24Follow-up47 m, alive45 m, alive10 m, dead3 m, aliveTiffeneau-index pre to post surgery+5% (85 - 87%)-5% (69% - 64%)+11% (64 - 75%)+/- 0 (83%)Abbreviations: OSAS - obstructive sleep apnea syndrome; IDDM - insulin dependent diabetes mellitus; NSCLC - Non small-cell lung cancer
For patients A to C we advised wound debridement and negative pressure wound therapy (NPWT, V.A.C.® System, 3 M + KCI, St. Paul, MN, USA) for defect sanitation before surgery. The indication for surgery was given if the defect was considered rehabilitated with negative microbiological swabs and clean wound bed alongside declining infectious parameters in laboratory tests. In surgery, the destroyed sternum and adjacent ribs were resected with thorough debridement of the adherent structures, followed by reconstruction with four titanium bars and defect coverage with myocutaneous musculus vastus lateralis (MVL) free flap. Free MVL flap was chosen after failure of less invasive coverage attempts, for example pectoralis major suture. Furthermore, since the defects had to be conditioned beforehand, there was scar tissue build-up along the sides after NPWT, resulting in difficult mobilization of other graft options like latissimus dorsi grafts or pectoralis major muscle flaps. All patients were distinctly obese, resulting in additional tension on the anterior chest wall in supine position, therefore a free MVL flap was chosen to reduce tension and ensure better wound healing.
Sternal defect preparation: Patients were placed in supine position. The sternal wound defect was widely resected, in the oncological case to maximum extent to achieve tumor-free margins. For DSWI, all necrotic tissue was resected up to healthy bone material. For vascular anastomosis of the myocutaneous flap, the right internal mammary artery or the inferior thyroid vessels were carefully prepared and blocked with heparin-sodium solution (Fig. 1C). In case of abdomino-mediastinal herniation after previous omentum interpositioning, the defect was repaired using IPOM mesh graft technique or direct suture after repositioning the omentum to intraabdominal.
Defect coverage: Ribs 2–5 were parasternally freed from connective and muscle tissue for clip placement. Clips with alternating rigid and flexible connectors were placed. The connecting bars were then attached to the clips in cranial to caudal order from the side after thorough measurement and corresponding shortening. (Fig. 1D).
Free flap preparation: Following rigid chest wall reconstruction, myocutaneous vastus lateralis muscle (MVL) free flaps were raised and micro-anastomosed to the vessels mentioned above. The left or right vastus lateralis was chosen as donor site and the planned flap measured to fit the sternal defect size. It was then thoroughly dissected and raised with a long cranial pedicle for re-anastomosis. The respective donor site wound was primarily closed by suture in all patients.
Free flap replantation: The raised MVL flap was then directly re-anastomosed on the prefabricated vessels (as mentioned above) with running suture, after shortening the vessels appropriately to avoid kinking. Flap blood flow was continuously monitored by duplex ultrasound during surgery. Post surgery, blood flow monitoring was gradually reduced over the course of 10 days. For postoperative thrombosis prophylaxis, the patients received iv heparin or, in case of HIT, argatroban. Drainages were placed in all levels (pleural, mediastinal, sub-flap), if necessary.
All patients received perioperative antibiotic prophylaxis with cefuroxime or in case of known allergy clindamycin, followed by broad-spectrum antibiotic (piperacillin/tazobactam) for a minimum of three to five days, or pathogen-appropriate treatment in case of positive swab.
Patient D initially refused rigid reconstruction and underwent defect coverage with MVL free flap only. There was prolonged thoracic wall instability and the patient consented to secondary rigid reconstruction. The left half of the flap was lifted, and the left sided clips placed (Fig. 2A). The right-sided clips were placed through single incisions of the right chest wall and the connecting bars placed from left to right under the flap.
Fig. 1(A) computed tomography transversal, note missing sternum; (B) sternectomy wound after preconditioning with NPWT, note interpositioned omentum flap; (C) internal mammary artery preparation for vessel anastomosis; (D) rigid stabilization with alternating clip implantation
Results
All patients were primarily extubated postoperatively, still in the operating theater. They reported good chest wall stability and no impairment of breathing mechanics, consistent with pre- and postoperative lung function testing. The FEV1/FVC ratio showed a mean increase of + 2.5% (see Table 1), while the focus was mainly on stable breathing mechanics after rigid reconstruction of the anterior chest wall. The mean defect size was 229,8 cm² (200–400 cm²). Postoperative hospital stay was 19 days (9–29), with a mean ICU stay of 6 days [1–14]. Postoperative pain syndrome was evaluated by visual analog scale (VAS) and managed through peridural anaesthesia in two cases, in combination with WHO standard by non-steroidal antiphlogistics alongside oral or intravenous opioid drugs. Control chest x-ray imaging confirmed stable clip and connection bar placement. The patients furthermore reported excellent aesthetic outcome with improved quality of life and excellent myocutaneous flap vitality. There were no secondary complications to the flap or at the clip-bone interface even after radiation therapy in one patient. There was no impairment in function or any other complication observed at the flap donor site. At d3 after surgery in Patient D, chest x-ray revealed deformed titanium bars from excessive mobilization, requiring revision surgery (Fig. 2B). The MVL flap was semi-lifted in a protective manner and remained vital (Fig. 2A, C). This patient eventually returned to his profession as a singer without impaired breathing mechanics and good lung function. The aesthetic outcome is presented in Fig. 3. Mean follow-up was 26 months (2–47), with one patient lost-to-follow up and one patient deceased.
Fig. 2(A) Semi-elevated flap for bar placement, note: top of picture represents patients left side; (B) bar deformity after mobilization; (C) bar revision with semi-elevated flap, note: top of picture represents patients left side; (D) correct placement of STRATOS system after revision surgery
Fig. 3. Fully healed MVL flap in patient D, two months post-surgery; Note: arrow indicating cranial direction
Discussion
The main limitation of this report is the small case number, but we can conclude that large-scale reconstructive surgery of the anterior chest wall after total sternectomy can be performed without negative impact to overall outcome and rare minor complications. We consider the main indication for the presented procedure to be need for complete sternal resection with failure of less invasive reconstructive procedures. As contraindications, we identified ongoing wound infection, no target vessel for flap anastomosis and lack of sufficient bone tissue (osteomyelitis) for secure clip placement. Short intensive care unit and hospital stay as well as improved breathing mechanics result in overall improved quality of life in this patient cohort. This is concordant with previously published case reports which used different reconstructive approaches for sternum defects [3–7, 10, 11]. While many reports are individual treatment approaches with individualized reconstruction methods, we are relying on a commercially available system (STRATOS®) to facilitate reproducibility. Similar techniques have previously been described in works of Berthet et al. [12, 13]. However, it should be emphasized that in the previous reports there were three cases of total sternectomy, which showed smaller defects that could be covered without free myocutaneous flap. Also, we cannot agree with reports of bar fractures [12, 14], but in contrary report on bar stability even after severe deformation in patient D. This may in part be due to usage of rotating connector parts in this cohort, ensuring more flexibility with mobilization and breathing mechanics.
Conclusion
Thorough planning is indispensable for solid and aesthetic outcome in large reconstructive surgery. We demonstrate the feasibility of a combined rigid and aesthetic soft tissue reconstruction of the anterior chest wall after complete sternectomy with reestablished breathing mechanics and the possibility to qualify oncologic patients to further therapy in selected cases. In combination with growing experience in large-extent reconstructive surgery flap interposition, we are gaining confidence in complex cases of sternum reconstruction.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Baillot R Cloutier D Montalin L Cote L Lellouche F Houde C Impact of deep sternal wound infection management with vacuum-assisted closure therapy followed by sternal osteosynthesis: a 15-year review of 23,499 sternotomies Eur J Cardiothorac Surg 2010374880710.1016/j.ejcts.2009.09.02319880326 · doi ↗ · pubmed ↗
- 2Kubota H Miyata H Motomura N Ono M Takamoto S Harii K Deep sternal wound infection after cardiac surgery J Cardiothorac Surg 2013813210.1186/1749-8090-8-13223688324 PMC 3663691 · doi ↗ · pubmed ↗
- 3Banuelos J Abu-Ghname A Bite U Moran SL Bakri K Blackmon SH Reconstruction of Oncologic Sternectomy defects: lessons learned from 60 cases at a single Institution Plast Reconstr Surg Glob Open 201977 e 235110.1097/GOX.000000000000235131942367 PMC 6952121 · doi ↗ · pubmed ↗
- 4Motono N Shimada K Kamata T Uramoto H Sternal resection and reconstruction for metastasis due to breast cancer: the Marlex sandwich technique and implantation of a pedicled latissimus dorsi musculocutaneous flap J Cardiothorac Surg 20191417910.1186/s 13019-019-0905-z 30999925 PMC 6471832 · doi ↗ · pubmed ↗
- 5Fabre D El Batti S Singhal S Mercier O Mussot S Fadel EA paradigm shift for sternal reconstruction using a novel titanium rib bridge system following oncological resections Eur J Cardiothorac Surg 20124269657010.1093/ejcts/ezs 21122551966 · doi ↗ · pubmed ↗
- 6Dell’Amore A Cassanelli N Dolci G Stella F An alternative technique for anterior chest wall reconstruction: the sternal allograft transplantation Interact Cardiovasc Thorac Surg 2012156944710.1093/icvts/ivs 41122990634 PMC 3501314 · doi ↗ · pubmed ↗
- 7Aranda JL Jimenez MF Rodriguez M Varela G Tridimensional titanium-printed custom-made prosthesis for sternocostal reconstruction Eur J Cardiothorac Surg 2015484 e 92410.1093/ejcts/ezv 26526242897 · doi ↗ · pubmed ↗
- 8Topolnitskiy E Chekalkin T Marchenko E Yasenchuk Y Repair of huge thoracic defect combined with hernia after multimodality treatment of breast cancer Respir Med Case Rep 2021341015583487725210.1016/j.rmcr.2021.101558 PMC 8633021 · doi ↗ · pubmed ↗