Short-term and long-term outcomes of on-pump beating-heart coronary artery bypass surgery in dialysis and non-dialysis patients: a retrospective study in a single center
Chia-Hsun Lin, Yen‐Yang Chen, Yu‐Tong Yen, Patrick Hung‐Ju Kao, Chai-Hock Chua, Hung-Hsing Chao, Ming-Jen Lu

TL;DR
This study found that dialysis patients undergoing a specific heart surgery have similar short-term outcomes but worse long-term survival compared to non-dialysis patients.
Contribution
The study provides new evidence on the safety and effectiveness of OPBH-CABG in dialysis patients compared to non-dialysis patients.
Findings
Dialysis patients had longer hospital stays and higher late mortality compared to non-dialysis patients.
There were no significant differences in in-hospital mortality or surgical complications between the two groups.
OPBH-CABG is a safe and effective option for dialysis patients.
Abstract
This study aimed to evaluate the short-term and long-term outcomes of dialysis and non-dialysis patients after On-pump beating-heart coronary artery bypass grafting (OPBH-CABG). We retrospectively reviewed medical records of 659 patients underwent OPBH-CABG at our hospital from 2009 to 2019, including 549 non-dialysis patients and 110 dialysis patients. Outcomes were in-hospital mortality, length of stay, surgical complications, post-CABG reintervention, and late mortality. The median follow-up was 3.88 years in non-dialysis patients and 2.24 years in dialysis patients. Propensity matching analysis was performed. After 1:1 matching, dialysis patients had significantly longer length of stay (14 (11–18) vs. 12 (10–15), p = 0.016), higher rates of myocardial infarction (16.85% vs. 6.74%, p = 0.037) and late mortality (25.93% vs. 9.4%, p = 0.005) after CABG compared to non-dialysis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
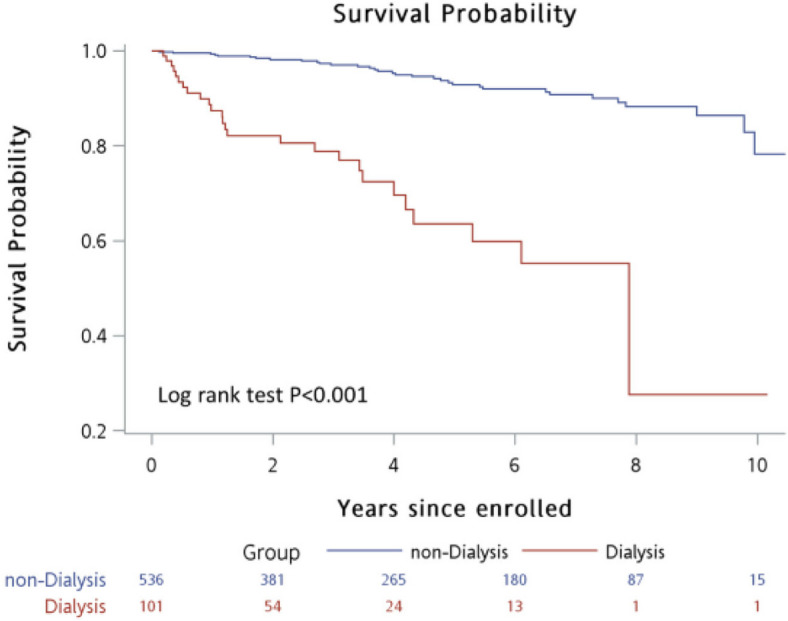 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMechanical Circulatory Support Devices · Heart Failure Treatment and Management · Cardiac Structural Anomalies and Repair
Background
Patients on dialysis have high risks for coronary artery diseases and displayed poor prognosis after coronary artery bypass grafting (CABG) compared to non-dialysis patients, including higher surgical mortality, postoperative complications, readmission rate, revascularization, and lower survival [1–5]. On-pump heart-beating CABG is a hybrid surgical approach maintaining stable hemodynamics with the support of cardiopulmonary bypass, but without cardioplegic arrest and aortic cross-clamping [6]. This may lead to lower myocardial injury, therefore is an option for patients with high-risk profiles. However, its outcomes in different high-risk groups remain further investigation. The purpose of this study was to evaluate short-term and long-term outcomes in dialysis and non-dialysis patients after on-pump beating-heart CABG.
Methods
Patients
This retrospective study enrolled patients underwent coronary artery on-pump beating-heart bypass surgery in our hospital between 2009 and 2019. Inclusion criteria were: 1) with coronary artery disease; 2) indicated for CABG surgery. No exclusion criteria. All necessary information was reviewed from medical record, including demography, clinical characteristics, and postoperative complications. The study was approved by the institutional review board, and the requirement of informed consent was waived.
Operative procedure of on-pump beating heart CABG and renal management
Our perioperative management of renal replacement therapy were as follows: 1) low-potassium hemodialysis (HD) for consecutive 3 days before operation; 2) only hemofiltration during bypass; 3) start of regular intermittent HD on the first postoperative day, followed by regular intermittent HD three times a week.
CABG was performed with a median sternotomy. A partial cardiopulmonary bypass was used. The left anterior descending (LAD) artery was anastomosed with left or right ITA graft. The non-LAD coronary arteries were grafted with a sequential saphenous vein graft (SVG). The distal end of SVG was anastomosed to ascending aorta using partially side-clamping of aorta. Intra-aortic blood pump (IABP) was used liberally pre- or post-operatively in patients with hemodynamic instability, unstable cardiac rhythms, or poor LV function.
Outcomes
Short-term outcomes were in-hospital mortality, length of stay, surgical complications. Long-term outcomes were adverse cardiac events, percutaneous coronary intervention (PCI) reintervention, and late mortality during follow-up. Adverse cardiac events included recurrent angina and myocardial infarction (MI). Late mortality is defined as death during follow-up.
Statistical analysis
Continuous data with a normal distribution were analyzed by Student’s t-test and are presented as the mean ± standard deviation (SD); continuous data without a normal distribution are presented as the median (interquartile range (IQR)) and were analyzed by the Wilcoxon rank-sum test. Normal distribution of variables was tested by Shapiro–Wilk. Categorical data were analyzed with the chi-square test or Fisher’s exact test and are presented as n (%), as appropriate. Patients were matched as propensity score (PS) with the ratio of dialysis: non-dialysis = 1:1 according to age, male sex, BMI, smoking status, preoperative EF, CCS angina class, diabetes mellitus, hyperlipidemia, cardiac dysfunction, PAOD, liver insufficiency, cerebral deficits, number of grafts, complete revascularization, grafting strategy. Kaplan–Meier plot was performed and used log-rank test to compare late mortality between non-dialysis and dialysis patients. Late mortality was identified as death after discharge, and the follow-up duration was estimated from surgery date to the last visit or death. A two-sided P-value of < 0.05 was regarded as statistically significant. Data management and statistical analyses were conducted with SAS version 9.4 software (SAS Institute, Inc.).
Results
Demographic characteristics
A total of 549 non-dialysis patients and 110 dialysis patients were included in this study (Table 1). Compared to dialysis patients, non-dialysis patients had significantly higher body mass index, higher proportions of male, current smoker, normal preoperative ejection fraction (EF), Canadian cardiovascular society (CCS) classes I and II, hyperlipidemia, complete revascularization, bilateral internal thoracic arteries grafting, and longer follow-up period. Non-dialysis patients also had significantly lower European system for cardiac operative risk evaluation (EuroSCORE), lower proportions of diabetes, cardiac dysfunction, peripheral artery occlusive disease (PAOD), liver insufficiency, and cerebral deficits. After PS matching, 89 non-dialysis patients and 89 dialysis patients were enrolled in the analysis. The characteristics between non-dialysis and dialysis groups were balanced, except EuroSCORE and follow-up period. Non-dialysis patients still had lower additive and logistic score and longer follow-up period.Table 1. Baseline characteristics of the study population before and after matchingCharacteristicBefore matchingAfter matchingNon-dialysis patients****Dialysis patientsP**-valueNon-dialysis patientsDialysis patientsP-value****(N = 549)(N = 110)(N = 89)****(N = 89)Age, years63.00 (57.00–69.00)62.00 (55.00–67.00)0.06562.94 ± 9.5762.69 ± 9.080.854Male sex443 (80.69%)74 (67.27%)0.00263 (70.79%)64 (71.91%)0.868BMI, kg/m^2^25.92 (23.46–28.40)24.58 (22.03–26.44) < .00124.28 (21.91–27.34)24.80 (22.43–26.40)0.671EuroSCORE^a^ Additive4.00 (2.00–7.00)8.00 (5.50–10.00) < .0016.00 (3.00–9.00)8.00 (5.00–10.00)0.005 Logistic2.59 (1.32–6.21)8.91 (4.73–17.60) < .0014.58 (2.24–11.94)7.62 (4.10–15.20)0.010Year of surgery0.1230.462 2009–201071 (12.93%)9 (8.18%)13 (14.61%)7 (7.87%) 2011–2012121 (22.04%)15 (13.64%)17 (19.1%)12 (13.48%) 2013–201498 (17.85%)24 (21.82%)19 (21.35%)22 (24.72%) 2015–2016105 (19.13%)26 (23.64%)15 (16.85%)18 (20.22%) 2017–2019154 (28.05%)36 (32.73%)25 (28.09%)30 (33.71%)Smoking status < .001** > 0.999 Never-smoker354 (64.48%)95 (86.36%)75 (84.27%)75 (84.27%) Ex-smoker71 (12.93%)4 (3.64%)5 (5.62%)4 (4.49%) Current smoker124 (22.59%)11 (10.00%)9 (10.11%)10 (11.24%)Preoperative EF, %** < .0010.921 > 50, normal LV function385 (70.13%)52 (47.27%)48 (53.93%)47 (52.81%) 40–50, mild LV dysfunction77 (14.03%)26 (23.64%)18 (20.22%)19 (21.35%) 30–40, moderate LV dysfunction52 (9.47%)21 (19.09%)18 (20.22%)16 (17.98%) < 30, severe LV dysfunction35 (6.38%)11 (10%)5 (5.62%)7 (7.87%)Postoperative EF, %0.0800.455 > 50, normal LV function370 (67.4%)60 (54.55%)48 (53.93%)50 (56.18%) 40–50, mild LV dysfunction83 (15.12%)24 (21.82%)17 (19.1%)20 (22.47%) 30–40, moderate LV dysfunction50 (9.11%)13 (11.82%)9 (10.11%)11 (12.36%) < 30, severe LV dysfunction46 (8.38%)13 (11.82%)15 (16.85%)8 (8.99%)CCS Angina Class0.0010.887 I or II141 (25.68%)19 (17.27%)17 (19.1%)15 (16.85%) III210 (38.25%)30 (27.27%)26 (29.21%)25 (28.09%) IV198 (36.07%)61 (55.45%)46 (51.69%)49 (55.06%)Comorbidities Diabetes mellitus307 (55.92%)78 (70.91%)0.00455 (61.8%)62 (69.66%)0.269 Hypertension422 (76.87%)89 (80.91%)0.35468 (76.4%)73 (82.02%)0.356 Hyperlipidemia341 (62.11%)38 (34.55%) < .00133 (37.08%)34 (38.2%)0.877 COPD19 (3.46%)1 (0.91%)0.2253 (3.37%)1 (1.12%)0.621 Cardiac dysfunction107 (19.49%)31 (28.18%)0.04127 (30.34%)23 (25.84%)0.505 Renal dysfunction17 (3.1%)4 (3.64%)0.76597 (7.87%)4 (4.49%)0.350 PAOD12 (2.19%)14 (12.73%) < .0016 (6.74%)7 (7.87%)0.773 Liver insufficiency23 (4.19%)10 (9.09%)0.0318 (8.99%)6 (6.74%)0.578 Cerebral deficits48 (8.74%)20 (18.18%)0.00317 (19.1%)17 (19.1%) > 0.999Number of grafts0.0050.969 117 (3.1%)0 (0%)-- 245 (8.2%)11 (10%)10 (11.24%)9 (10.11%) 3112 (20.4%)37 (33.64%)26 (29.21%)26 (29.21%) ≥ 4375 (68.31%)62 (56.36%)53 (59.55%)54 (60.67%)Complete revascularization ^b^485 (89.48%)89 (80.91%)0.01273 (82.02%)73 (82.02%) > 0.999Grafting Strategy < .0010.541 NO ITA39 (7.1%)5 (4.55%)6 (6.74%)4 (4.49%) SITA352 (64.12%)93 (84.55%)75 (84.27%)73 (82.02%) BITA158 (28.78%)12 (10.91%)8 (8.99%)12 (13.48%)IABP use119 (21.68%)25 (22.73%)0.80826 (29.21%)17 (19.1%)0.115Years of follow-up3.88 (1.61–7.00)2.24 (0.73–4.01) < .001**4.57 (1.15–6.84)2.14 (0.73–4.13)0.001Significant values are showing in boldContinuous data without normal distribution were presented as median (IQR) and categorical data were presented as n (%)SD Standard deviation, IQR Interquartile range, BMI body mass index, EuroSCORE European system for cardiac operative risk evaluation, CABG coronary artery bypass graft surgery, EF ejection fraction, LITA left internal thoracic artery, LAD left anterior descending artery, LV left ventricular, CCS Canadian cardiovascular society, COPD chronic obstruction pulmonary disease, PAOD peripheral artery occlusive disease, BITA blateral internal thoracic arteries, MI myocardial infarction, PCI percutaneous coronary intervention, RCA right coronary artery, LCX left circumflex coronary artery, SVG saphenous vein graft, IABP intra-aortic balloon pump^a^There were 502 patients in the non-dialysis group and 104 patients in the dialysis group. 53 of patients were missing in all study population; 11 of patients were missing after matching^b^7 of patients were missing in all study population
The outcomes after CABG between non-dialysis and dialysis patients after PS matching are presented in Table 2. After CABG, dialysis group had significantly higher longer length of stay (14 (11–18) vs 11 (9–14) days, p = 0.016), post-CABG MI frequency (16.85% vs. 6.74%, p = 0.037), and mortality rate (25.93% vs 9.41%, p = 0.005) than non-dialysis group. No significant differences in in-hospital mortality, surgical complications or post-CABG reintervention were observed between groups. Figure 1 presents the crude survival curves excluded in-hospital death. A significantly lower survival during follow-up was observed in dialysis group compared to the non-dialysis group (p < 0.001 with long rank test).Table 2. Postoperative outcomes of the study population after PSMVariableNon-dialysis patientsDialysis patientsP-value**(N = 89)****(N = 89)Short-term outcomes In-hospital mortality4 (4.49%)8 (8.99%)0.232 Length of hospital stay for surgery, days12 (10–15)14 (11–18)0.016 Surgical complications Cardiac3 (3.37%)3 (3.37%) > 0.999 Non-cardiac26 (29.21%)24 (26.97%)0.739 Sepsis3 (3.37%)4 (4.49%) > 0.999 Wound infection8 (8.99%)4 (4.49%)0.232 Respiratory failure4 (4.49%)7 (7.87%)0.350 Hyperkalemia3 (3.37%)2 (2.25%) > 0.999 Gastrointestinal bleeding1 (1.12%)2 (2.25%) > 0.999 Stroke3 (3.37%)2 (2.25%) > 0.999 Reoperation for hemorrhage control5 (5.62%)8 (8.99%)0.387 Requiring ventilation > 24 h9 (10.11%)7 (7.87%)0.600Long-term outcomes** Postoperative outcome Recurrent angina17 (19.1%)12 (13.48%)0.310 Post-CABG MI6 (6.74%)15 (16.85%)0.037 Post-CABG reintervention16 (17.98%)20 (22.47%)0.455 PCI for failed LAD graft6 (6.74%)4 (4.49%)0.515 PCI for non-CABG RCA or LCX7 (7.87%)10 (11.24%)0.444 PCI for failed SVG graft8 (8.99%)14 (15.73%)0.172Late mortality ^a^8 (9.41%)21 (25.93%)0.005Significant values are showing in boldContinuous data without normal distribution are presented as median (IQR) and categorical data are presented as n (%)^a^Patients died in hospital were not included in the analysisFig. 1Crude survival rate including all death. A low survival curve was observed in dialysis patients during follow-up compared to non-dialysis patients (Long rank test, p < 0.001)
The outcomes of dialysis patients after CABG are presented in Table 3, including 99 patients with HD and 11 patients with peritoneal dialysis (PD). The in-hospital mortality was 7.07% in HD patients and 18.18% in PD patients (p = 0.222). No significant differences were found between the two groups, except the PD group had more cardiac complications than the HD group (18.18% vs 2.02%, p = 0.049).Table 3. Postoperative outcomes of the dialysis patientsCharacteristicHDPDP-value**(N = 99)****(N = 11)**In-hospital mortality7 (7.07%)2 (18.18%)0.222Length of stay for surgery, days14 (11–19)12 (10–15)0.081Complications Cardiac2 (2.02%)2 (18.18%)0.049 Non-cardiac28 (28.28%)3 (27.27%) > 0.999 Sepsis5 (5.05%)0 (0%) > 0.999 Wound infection6 (6.06%)0 (0%) > 0.999 Respiratory failure7 (7.07%)1 (9.09%)0.582 Hyperkalemia2 (2.02%)0 (0%) > 0.999 Gastrointestinal bleeding2 (2.02%)0 (0%) > 0.999 Stroke2 (2.02%)0 (0%) > 0.999 Reoperation for hemorrhage control9 (9.09%)1 (9.09%) > 0.999 Requiring ventilation > 24 h9 (9.09%)1 (9.09%) > 0.999Major adverse cardiac events Late mortality24 (24.24%)2 (18.18%) > 0.999Significant values are showing in boldContinuous data are presented as median were median (IQR) and categorical data are presented as n (%)
Discussions
The results of the present study, dialysis patients had significantly worse outcomes compared to non-dialysis patients after on-pump beating-heart CABG, including longer length of stay, higher rate of post-CABG MI, and lower survival during follow-up. However, no significant differences in in-hospital mortality, surgical complications, or revascularization rate during follow-up were observed between dialysis and non-dialysis groups. Our results show that on-pump beating-heart CABG is a safe and effective option for dialysis patients.
In the present study, no significant differences in in-hospital mortality, surgical complications, or post-CABG reintervention during follow-up was observed between dialysis and non-dialysis patients. Dialysis is known as an independent risk factor for surgical mortality after CABG [1, 3–5]. Our results showed on-pump beating-heart CABG could achieve comparable short-term surgical outcomes in dialysis patients as those in non-dialysis patients. Meanwhile, Chen et al. reported a higher risk for revascularization after CABG in dialysis patients than non-dialysis patients [3]. It is well-recognized that on-pump CABG ensures comprehensive revascularization [7, 8]. Our result showed that on-pump beating-heart CABG achieves good long-term revascularization also in dialysis group. These results together show that it is a safe and effective option for dialysis patients.
Our results showed that dialysis patients had a significantly longer length of stay, higher rate of MI, and poorer survival after CABG compared to non-dialysis patients. Dialysis is significantly associated with poor outcomes after cardiac surgery [1–5], and the risk for mortality is elevated as dialysis-dependence duration extends [1, 3]. Studies have reported that dialysis patients show significantly higher 30-day mortality, readmission rate, rates of postoperative MI or revascularization, and lower survival after CABG compared to non-dialysis patients [1–5]. CABG is not associated with short-term mortality but improves life expectancy of dialysis patients [5, 9, 10]. For better prognosis, more attention must be paid on dialysis patients’ postoperative conditions after CABG, including monitoring cardiovascular stability, and education of self-care for patients and caregivers.
In the present study, PD patients showed twofold higher in-hospital mortality compared to HD patients without statistically significant difference (2/12 vs. 7/115, p = 0.222) probably due to the limited sample size. Studies reported that PD patients were prone to higher in-hospital mortality than HD patients after CABG [11, 12]. Further study is needed to clarify the underlying mechanism.
Limitation
The study had some limitations. First, it is a retrospective study with those inherent limitations. Second, the study had small sample size and unequal distribution of patients across the dialysis and non-dialysis groups, which may skew the analysis of outcomes. Therefore, PS matching analysis was employed to account for these variables.
Conclusion
After on-pump beating-heart CABG, dialysis patients have longer length of stay, higher rate of postoperative MI, and poor survival; whereas no significant differences in in-hospital mortality or revascularization rate during follow-up between dialysis and non-dialysis patients. Our findings show that on-pump beating-heart CABG could achieve comparable surgical mortality and good long-term revascularization in dialysis patients as those in non-dialysis patients. It is a safe and effective option for dialysis patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bianco V Kilic A Gleason TG Aranda-Michel E Navid F Sultan I Longitudinal outcomes of dialysis-dependent patients undergoing isolated coronary artery bypass grafting J Card Surg 201934311011710.1111/jocs.1399130735576 · doi ↗ · pubmed ↗
- 2Leontyev S Davierwala PM Gaube LMRöhrig KA Lehmann S Holzhey DM Outcomes of dialysis-dependent patients after cardiac operations in a single-center experience of 483 patients Ann Thorac Surg 201710341270127610.1016/j.athoracsur.2016.07.05227938884 · doi ↗ · pubmed ↗
- 3Chen SW Chang CH Lin YS Wu VC Chen DY Tsai FC Effect of dialysis dependence and duration on post-coronary artery bypass grafting outcomes in patients with chronic kidney disease: A nationwide cohort study in Asia Int J Cardiol 2016223657110.1016/j.ijcard.2016.08.12127532236 · doi ↗ · pubmed ↗
- 4Sezai A Nakata K Hata M Yoshitake I Wakui S Hata H Long-term results of dialysis patients with chronic kidney disease undergoing coronary artery bypass grafting Ann Thorac Cardiovasc Surg 201319644144810.5761/atcs.oa.12.0202823411841 · doi ↗ · pubmed ↗
- 5Charytan DM Kuntz RE Risks of coronary artery bypass surgery in dialysis-dependent patients–analysis of the 2001 National Inpatient Sample Nephrol Dial Transplant 20072261665167110.1093/ndt/gfl 83517299001 · doi ↗ · pubmed ↗
- 6Perrault LP Menasche P Peynet J Faris B Bel Ade Chaumaray T On-pump, beating-heart coronary artery operations in high-risk patients: an acceptable trade-off?Ann Thorac Surg 1997641368137310.1016/S 0003-4975(97)00842-49386706 · doi ↗ · pubmed ↗
- 7Jiang Y Xu L Liu Y Deng B Dong N Chen S Beating-heart on-pump coronary artery bypass grafting vs. off-pump coronary artery bypass grafting: a systematic review and meta-analysis J Thorac Dis 20211374185419410.21037/jtd-21-26834422347 PMC 8339796 · doi ↗ · pubmed ↗
- 8Wang C Jiang Y Jiang X Chen S On-pump beating heart versus conventional on-pump coronary artery bypass grafting on clinical outcomes: a meta-analysis J Thorac Dis 20211374169418410.21037/jtd-21-56834422346 PMC 8339771 · doi ↗ · pubmed ↗