Defining what is left in a left-sided pancreatectomy
Kjetil Søreide, Ernesto Sparrelid

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
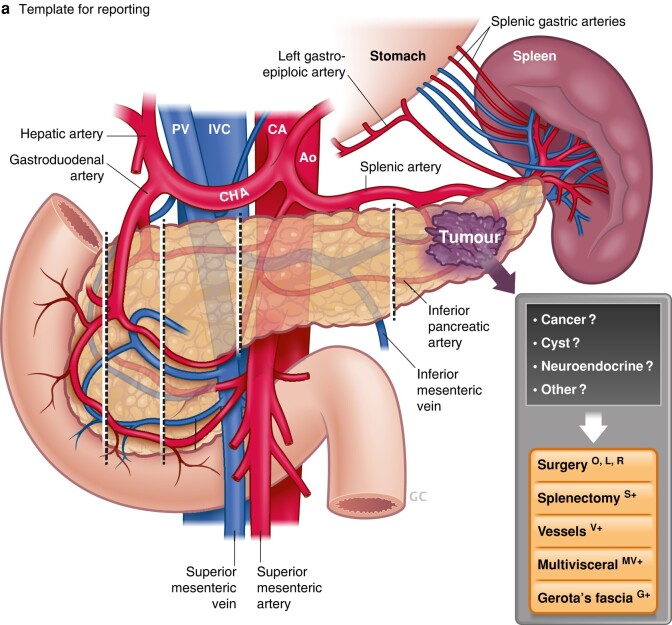 Figure 1
Figure 1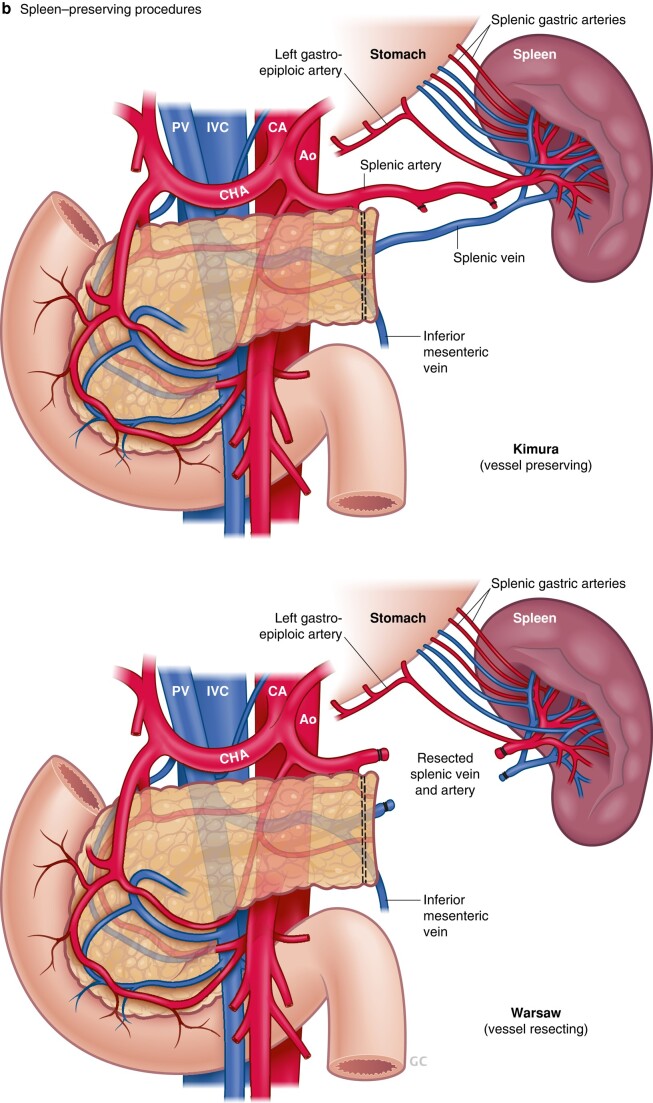 Figure 2
Figure 2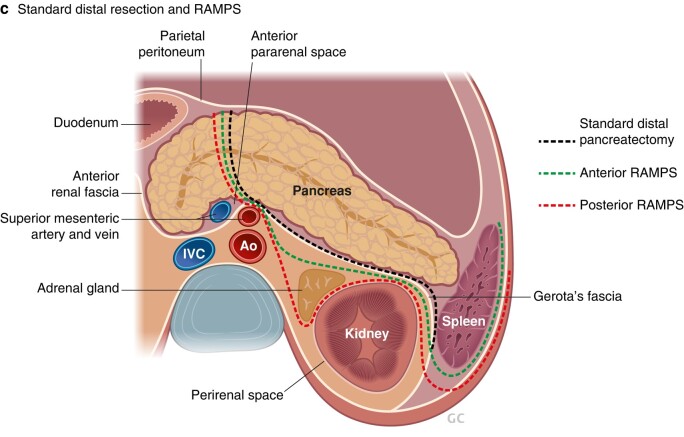 Figure 3
Figure 3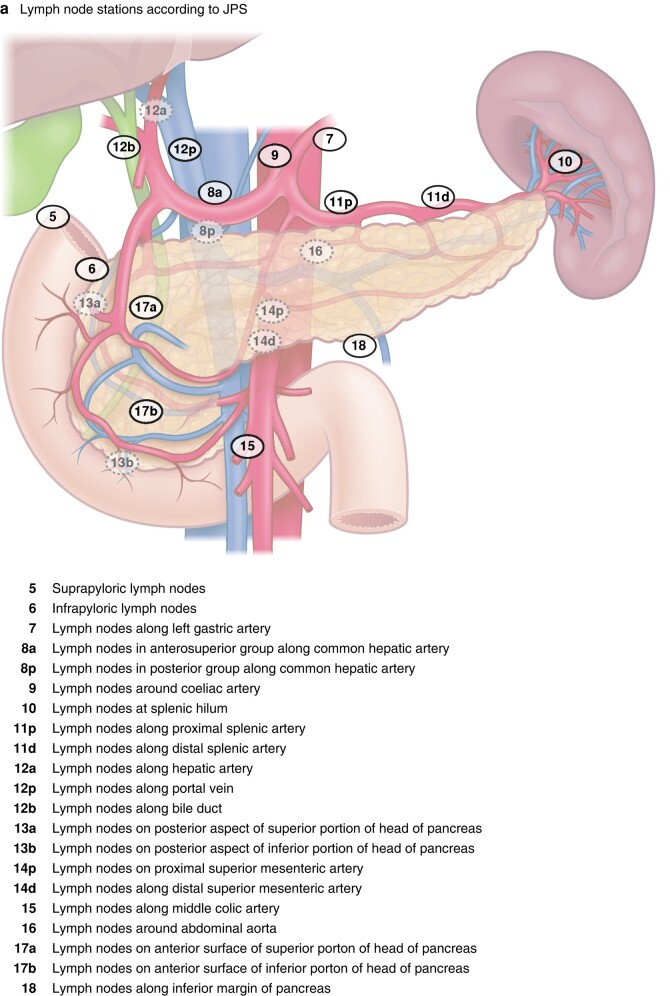 Figure 4
Figure 4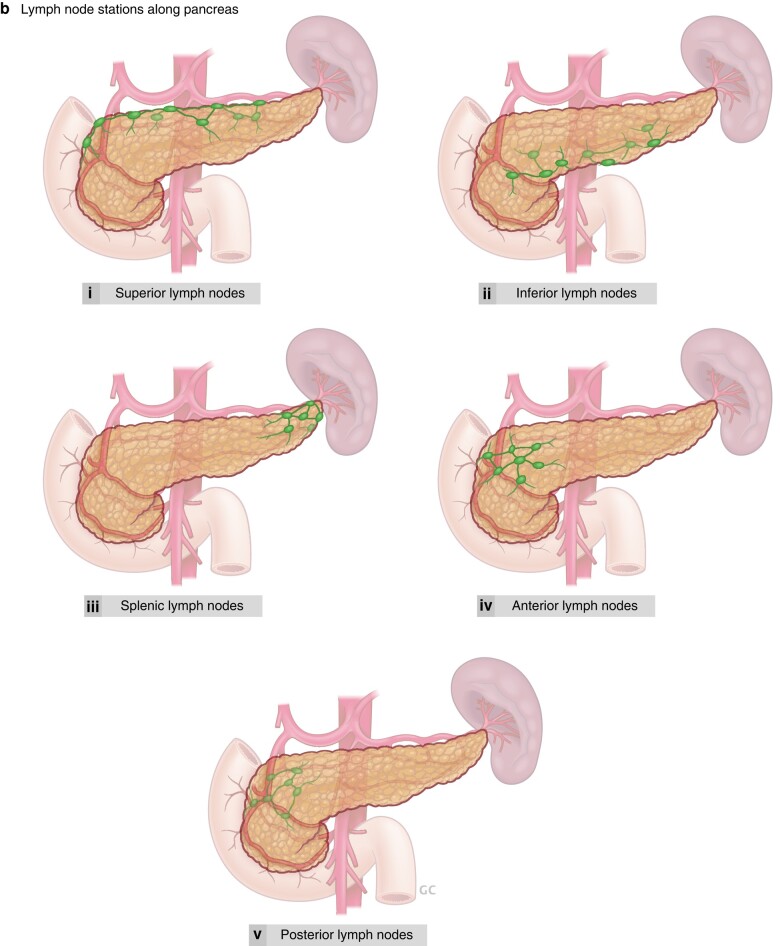 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Gastric Cancer Management and Outcomes · Cholangiocarcinoma and Gallbladder Cancer Studies
Distal pancreatectomy has received relatively less attention than the eponymous Whipple operation (pancreatoduodenectomy). However, increasing attention to detail in pancreatic surgery in general, and the development of minimally invasive techniques and better appreciation of benign, premalignant, and malignant pancreatic disease entities, has changed appreciation of the details. This has resulted in the need for a more refined consideration of distal pancreatectomy—increasingly referred to as ‘left-sided pancreatectomy’. Two current studies in BJS^1,2^ add to the knowledge base, and come as timely additions to recently evolving evidence on optimal management in distal pancreatectomy in the Journal^3–5^.
Of note, although several aspects of open and minimally invasive surgery in distal pancreatectomy have been entertained, in addition to the role of drains^6^ and risk of postoperative fistulas^7^, several other questions remain unanswered. One is the definition of ‘left’ in left-sided pancreatectomy. Another is the question of what else can, or even should, be left (behind): the spleen? lymph nodes? peripancreatic tissue?
Until recently, the definition of ‘left’ in left-sided pancreatectomy has been rather undeclared. In the past, the term ‘distal pancreatectomy’ was applied to any resection from a peripheral tail resection to a subtotal pancreatectomy. However, as shown in a large single-centre study^8^, there is considerable risk variation depending on the extent of resection. Hence, it is timely to see the novel definition and new terminology proposed in BJS by an international Delphi consensus group on left-sided pancreatectomy^1^. The new proposed terminology (Fig. 1a) defines the level of division of the pancreatic gland at defined anatomical landmarks, and allows a structured report of the procedure with additional parts included, such as splenectomy (designated S+) or spleen-preserving procedure (Fig. 1b) with vessel resection (designated V+)^1^. Multivisceral resection is designated MV+ and resection of Gerota’s fascia G+, as included in the radical antegrade modular pancreatosplenectomy (RAMPS) procedure^9^ (Fig. 1c), a still much debated topic. Hence, there is an opportunity to report and compare future studies that use this definition, and relate this to endpoints and assessment of outcomes.
Of note, the splenic vessels are not considered as part of ‘borderline’ or ‘locally advanced’ definitions in pancreatic cancer for tumours located in the body or tail^10^, even though cancers in this region also may be subject to more complex resectional procedures^11^. A lack of ‘borderline’ resectable terminology may also contribute to a lower likelihood of such tumours being considered for neoadjuvant chemotherapy, despite being associated with higher recurrence and lower survival rates^10^.
A second recurring discussion concerns the spleen, as this has commonly been considered as a part of a distal pancreatectomy, often en passant rather than according to indication, and with considerable variation in splenic salvage rates between institutions^12^. One reason for doing splenectomy routinely, rather than attempting a spleen-preserving procedure (Fig. 1b), may have been technical difficulties in dissection off the splenic vessels, particularly as practised in laparoscopic surgery. However, spleen preservation avoids the need for postsplenectomy vaccinations and the life-long increased infection risk. The introduction of robotically assisted minimally invasive surgery may facilitate spleen preservation, as demonstrated in one large study^13^ that showed higher spleen preservation rates (81% for robotic versus 63% laparoscopic procedures; P = 0.001). The spleen can be left after distal pancreatectomy by either sparing all the splenic vessels (Kimura procedure) or, even if the splenic vessels are difficult to dissect free (embedded in the pancreatic tissue, or involved by the tumour), by dividing and resecting the vessels (new terminology S+) and relying on the remaining blood flow from the gastrosplenic arteries (Warshaw procedure) (Fig. 1b).
With an increasing number of premalignant lesions considered for surgery, in particular neuroendocrine tumour and intraductal papillary mucinous neoplasia (IPMN), the indication for splenectomy has become less clear, if not obsolete from an oncological viewpoint. Indeed, in one of the largest cohort studies^2^ to date on IPMN, less than 7% of patients had lymph nodes with metastasis in the splenic hilum. What the study does not address is the risk of having isolated lymph node metastasis in the splenic hilum alone (station 10, and hence the need for splenectomy to remove these nodes), without any other lymph node metastases along the pancreatic surface, considering the lymphatic drainage routes of the pancreas (Fig. 2). As nodal harvest may be viewed as a staging (and not curative) procedure, it may be considered to avoid extensive node sampling in premalignant and not clinically overt cancer diseases. Of note, this topic is bound to stir debate until further evidence can be produced to support one decision over the other. A further extended debate in this regard is the need for perirenal fat clearance (referred to as RAMPS^9^) to achieve an oncologically safe operation for advanced cancers of the body and tail of the pancreas (Fig. 1c).
Taken together, considering what is ‘left’ in left-sided pancreatectomy has now been defined by consensus^1^. To consider, tongue in cheek, what else should be left, is still a matter of debate, but with some emerging data to support decisions. The spleen may be left (spleen-preserving procedure) for benign lesions such as IPMN^2^, as the risk of metastasis to the splenic lymph nodes is low (and with uncertainty whether spread is seen isolated in this area). Further data may be accrued using the novel proposed definitions and terminology^1^, with the hope of increasing the knowledge base in decision-making for left-sided pancreatectomy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Van Ramshorst TME , van Hilst J, Boggi U, Dokmak S, Edwin B, Keck Tet al Definitions and terminology of left-sided pancreatic resections: an international Delphi consensus. Br J Surg 2024. in press 10.1093/bjs/znae 03938686655 · doi ↗ · pubmed ↗
- 2Gorris M , van Bodegraven EA, Abu Hilal M, Bolm L, Busch OR, Del Chiaro Met al Outcomes after distal pancreatectomy with or without splenectomy for intraductal papillary mucinous neoplasm: international multicentre cohort study. Br J Surg 2024;111:znad 42410.1093/bjs/znad 424PMC 1077620738195084 · doi ↗ · pubmed ↗
- 3Giani A , van Ramshorst T, Mazzola M, Bassi C, Esposito A, de Pastena Met al Benchmarking of minimally invasive distal pancreatectomy with splenectomy: European multicentre study. Br J Surg 2022;109:1124–113035834788 10.1093/bjs/znac 204 · doi ↗ · pubmed ↗
- 4Nickel F , Distler M, Limen EF, Wise PA, Kowalewski KF, Tritarelli P Met al Initial learning curves of laparoscopic and robotic distal pancreatectomy compared with open distal pancreatectomy: multicentre analysis. Br J Surg 2023;110:1063–106736928918 10.1093/bjs/znad 045 · doi ↗ · pubmed ↗
- 5van Ramshorst TME , Giani A, Mazzola M, Dokmak S, Ftériche FS, Esposito Aet al Benchmarking of robotic and laparoscopic spleen-preserving distal pancreatectomy by using two different methods. Br J Surg 2022;110:76–8336322465 10.1093/bjs/znac 352PMC 10364499 · doi ↗ · pubmed ↗
- 6van Bodegraven EA , van Ramshorst TME, Balduzzi A, Hilal MA, Molenaar IQ, Salvia Ret al Routine abdominal drainage after distal pancreatectomy: meta-analysis. Br J Surg 2022;109:486–48835576374 10.1093/bjs/znac 042PMC 10364730 · doi ↗ · pubmed ↗
- 7Bonsdorff A , Ghorbani P, HelanteräI, Tarvainen T, Kontio T, Belfrage Het al Development and external validation of DISPAIR fistula risk score for clinically relevant postoperative pancreatic fistula risk after distal pancreatectomy. Br J Surg 2022;109:1131–113935983583 10.1093/bjs/znac 266PMC 10364701 · doi ↗ · pubmed ↗
- 8Loos M , Mack CE, Xu ATL, Hassenpflug M, Hinz U, Mehrabi Aet al Distal pancreatectomy: extent of resection determines surgical risk categories. Ann Surg 2024;279:479–48537259852 10.1097/SLA.0000000000005935 PMC 10829897 · doi ↗ · pubmed ↗