Folliculocentric eruption following stem cell transplantation
Michael J. Diaz, Mahtab Forouzandeh, Tyler Werbel, Kiran Motaparthi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1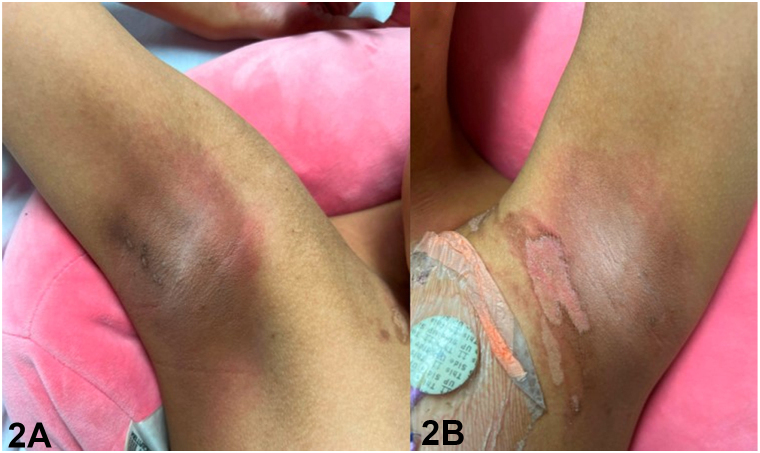 Figure 2
Figure 2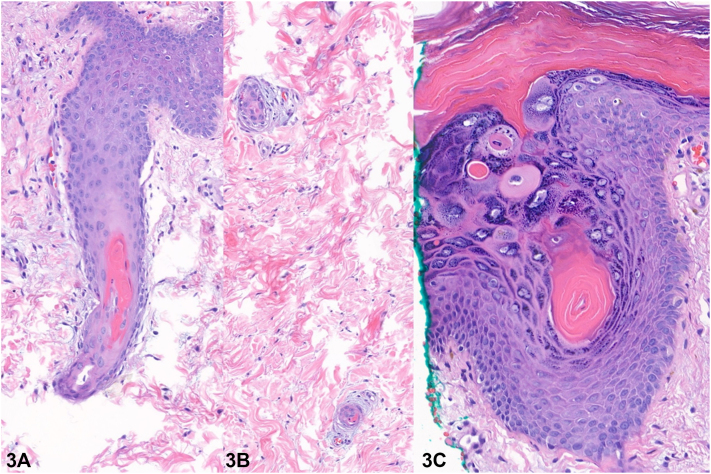 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChemotherapy-related skin toxicity · Nail Diseases and Treatments · Cancer and Skin Lesions
History
A 12-year-old girl with a history of acute myeloid leukemia presented with a 2-week history of perifollicular hyperpigmented papules. Onset was 44 days following haploidentical stem cell transplant, preceded by conditioning chemotherapy with busulfan and fludarabine. Examination revealed numerous hyperpigmented papules and superficial desquamation involving the bilateral axillae, inguinal folds, and abdominal flexures. Papules distributed on the inguinal area coalesced within the inguinal folds (Fig 1). Erythema and superficial desquamation were also observed in the axillae (Fig 2). Punch biopsy revealed dysmaturation overlying an acanthotic and papillomatous epidermis. Follicular plugging with dyskeratosis, dysmaturation, and syringosquamous metaplasia were also seen (Fig 3).Fig 1. Fig 2Fig 3
Question 1: Which of the following is the most likely diagnosis?
- A.Acute graft-versus-host disease (aGVHD)
- B.Lichen planopilaris (LPP)
- C.Toxic erythema of chemotherapy (TEC)
- D.Candidal intertrigo
- E.Toxic epidermal necrolysis (TEN)
Answers:
- A.aGVHD – Incorrect. The absence of an exanthematous to necrolytic clinical presentation in addition to the histopathological findings (dyskeratosis, follicular plugging, and syringosquamous metaplasia) are inconsistent with aGVHD.
- B.LPP – Incorrect. LPP is a scarring alopecia characterized by perifollicular erythema and scaling. While LPP demonstrates follicular distribution, this patient also presented with desquamation of the inguinal folds and axillae.
- C.TEC – Correct. TEC encompasses a spectrum of cutaneous eruptions triggered by chemotherapeutic drugs.1 Latency is variable, but findings classically appear within 2 days to 3 weeks of chemotherapy initiation and are self-limited, resolving with desquamation followed by postinflammatory hyperpigmentation.2 The perifollicular distribution, together with intertriginous desquamative erythema, recent chemotherapy, and consistent pathologic findings support a diagnosis of TEC secondary to the busulfan conditioning regimen. Similar presentations have been previously reported with use of busulfan-containing regimens.3
- D.Candidal intertrigo – Incorrect. Intertrigo complicated by candidiasis is characterized by a flexural eruption with erythema, maceration, and peripheral scale with pustules; satellite lesions are variable. Additionally, no fungal elements were identified on histopathology.
- E.TEN – Incorrect. The mild clinical presentation, lack of mucosal involvement, latency of more than 1 month, and evidence of dysmaturation on histopathology are not consistent with TEN.
Question 2: In differentiating TEC from aGVHD following stem cell transplant, which of the following clinical features is more likely to be observed in TEC?
- A.Morbilliform exanthem
- B.Severe mucositis
- C.Diarrhea
- D.Hepatitis
- E.Flexural distribution
Answers:
- A.Morbilliform exanthem – Incorrect. aGVHD typically presents as a morbilliform exanthem or in severe cases with epidermal necrolysis.
- B.Severe mucositis – Incorrect. Severe mucositis is more typical of TEN and can also be observed in aGVHD. Even in severe cases of TEC, mucositis is typically mild.
- C.Diarrhea – Incorrect. Systemic involvement including gastrointestinal disease and hepatitis is more characteristic of aGVHD.
- D.Hepatitis – Incorrect. Systemic involvement including hepatitis is more characteristic of aGVHD.
- E.Flexural distribution – Correct. TEC most commonly affects intertriginous areas or skin folds of flexural regions such as the axillae and groin.
Question 3: Which of the following statements provides the appropriate management of this condition?
- A.Methylprednisone
- B.Topical emollients or corticosteroids
- C.Hydroxychloroquine
- D.Fluconazole
- E.Intravenous immunoglobulin
Answers:
- A.Methylprednisone – Incorrect. High-dose systemic corticosteroids can be used for the treatment of aGVHD.
- B.Topical emollients or corticosteroids – Correct. TEC is most commonly managed with supportive care, including topic emollients and mild to high-potency topical corticosteroids.4^,^5
- C.Hydroxychloroquine – Incorrect. Hydroxychloroquine may be administered for LPP.
- D.Fluconazole – Incorrect. Fluconazole is the systemic treatment of choice for candidal intertrigo.
- E.Intravenous immunoglobulin – Incorrect. In combination with systemic corticosteroids, intravenous immunoglobulin is utilized in the treatment of TEN.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Smith S.M.Milam P.B.Fabbro S.K.Gru A.A.Kaffenberger B.H.Malignant intertrigo: a subset of toxic erythema of chemotherapy requiring recognition JAAD Case Rep 26201647648110.1016/j.jdcr.2016.08.01627981223 PMC 5149062 · doi ↗ · pubmed ↗
- 2Bolognia J.L.Cooper D.L.Glusac E.J.Toxic erythema of chemotherapy: a useful clinical term J Am Acad Dermatol 593200852452910.1016/j.jaad.2008.05.01818694683 · doi ↗ · pubmed ↗
- 3Parker T.L.Cooper D.L.Seropian S.E.Bolognia J.L.Toxic erythema of chemotherapy following i.v. BU plus fludarabine for allogeneic PBSC transplant Bone Marrow Transplant 485201364665010.1038/bmt.2012.21823165491 · doi ↗ · pubmed ↗
- 4Lu A.Endicott A.Tan S.Y.Toxic epidermal necrolysis-like toxic erythema of chemotherapy: 2 illustrative cases JAAD Case Rep 152021565910.1016/j.jdcr.2021.07.01034401432 PMC 8358280 · doi ↗ · pubmed ↗
- 5Yeager A.Stephen S.Forrestel A.Rosenbach M.Unilateral axillary toxic erythema of chemotherapy in a patient with previous axillary lymph node dissection: implications for pathophysiology and therapy JAMA Dermatol 1526201672772810.1001/jamadermatol.2015.490526747788 · doi ↗ · pubmed ↗