Forward-viewing echoendoscope aids tissue acquisition via the afferent limb after pancreaticoduodenectomy
Soma Fukuda, Susumu Hijioka, Yoshikuni Nagashio, Yuta Maruki, Mark Chatto, Yutaka Saito, Takuji Okusaka
Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
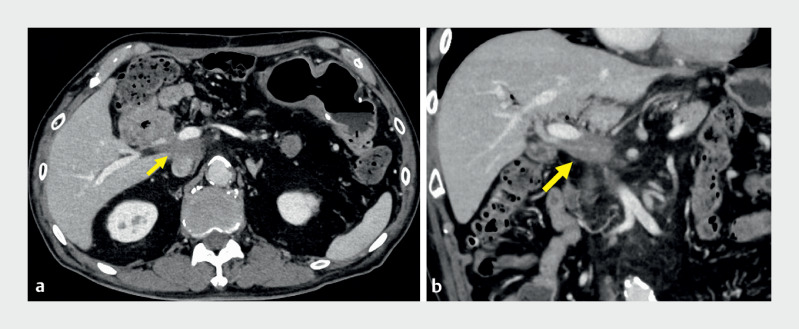 Fig. 1
Fig. 1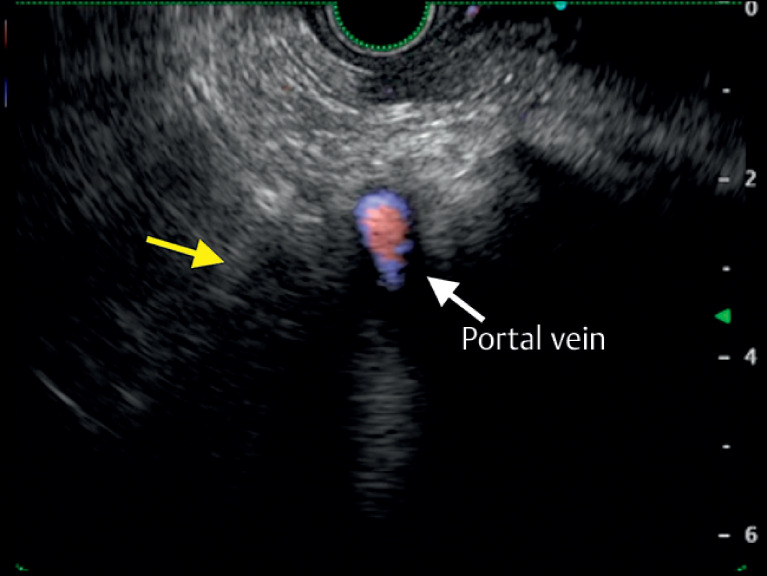 Fig. 2
Fig. 2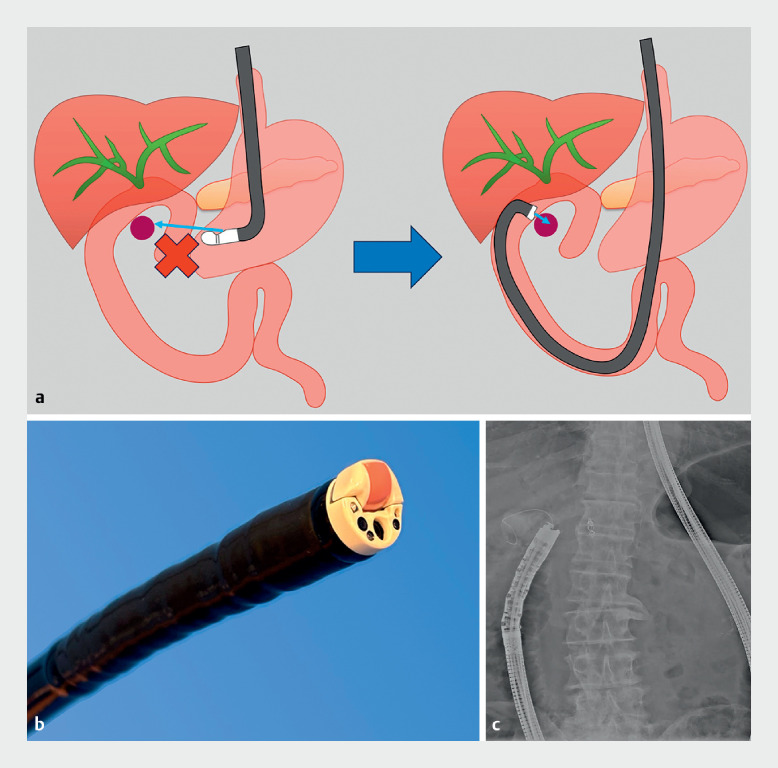 Fig. 3
Fig. 3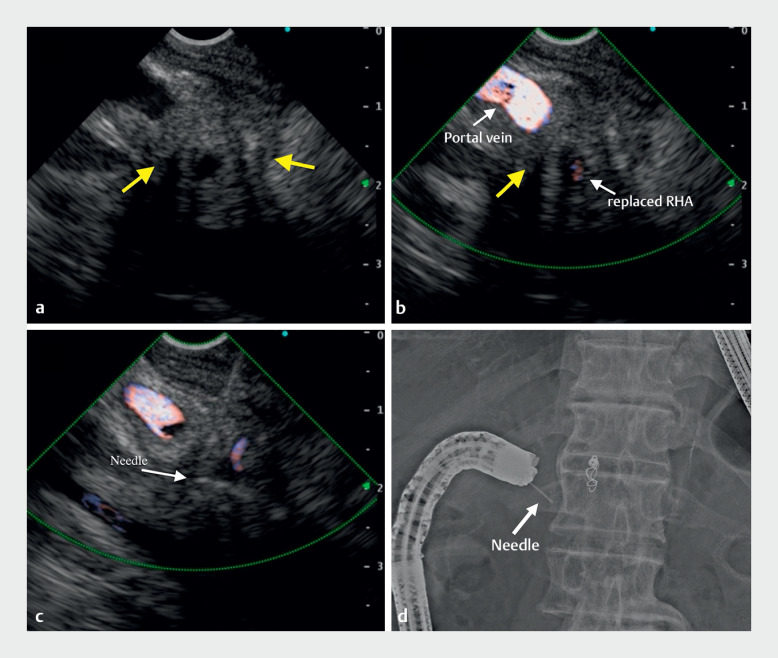 Fig. 4
Fig. 4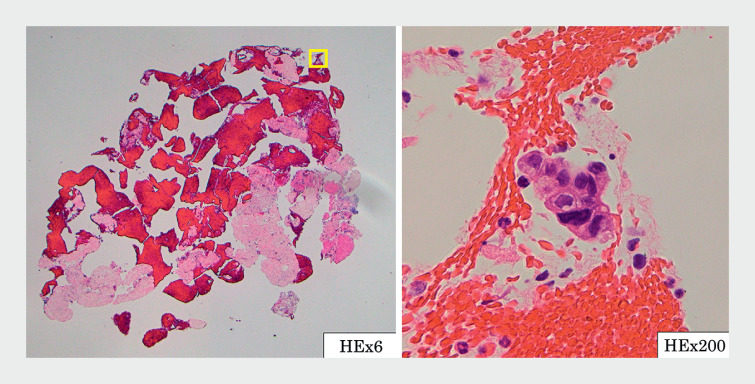 Fig. 5
Fig. 5- —This work was supported in part by The National Cancer Center Research and Development Fund.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMilitary Technology and Strategies · Legal and Regulatory Analysis · Linguistic, Cultural, and Literary Studies
Endoscopic ultrasound-guided tissue acquisition (EUS-TA), commonly performed with an oblique-viewing echoendoscope, can be difficult in patients with surgically altered anatomy 1 . Recently, EUS-TA using an oblique-viewing echoendoscope inserted over a guidewire into the afferent limb has been reported 2 , but there is the risk of perforation. Although forward-viewing echoendoscopes can be safely inserted into the distal intestinal tract, there are few reports about EUS-TA via the afferent limb using them 3 4 . Here, we describe a patient with surgically altered anatomy who underwent EUS-TA using a forward-viewing echoendoscope for recurrent cancer of the distal bile duct.
The 85-year-old man had previously undergone pancreaticoduodenectomy with modified Child’s reconstruction for distal bile duct cancer. Two years later, computed tomography revealed a 30-mm intra-abdominal mass behind the portal vein ( Fig. 1 ), suggestive of bile duct cancer recurrence. We attempted EUS-TA using a transgastric approach. However, the mass puncture could not be performed because of the intervening portal vein ( Fig. 2 ). Therefore, a decision was made to perform EUS-TA via the afferent limb using a forward-viewing echoendoscope (TGF-UC260J; Olympus, Tokyo, Japan) instead ( Fig. 3 a , b ). The colonoscope was inserted into the afferent limb, followed by a guidewire, and the colonoscope was removed. Next, the echoendoscope was inserted into the afferent limb over the guidewire under fluoroscopic guidance and endoscopic vision ( Fig. 3 c ). EUS successfully showed a hypoechoic mass adjacent to the portal vein ( Fig. 4 a , b ). EUS-TA was performed without complications using a 22-gauge Franseen needle ( Fig. 4 c , d , Video 1 ). The histopathological diagnosis was adenocarcinoma, consistent with bile duct cancer recurrence ( Fig. 5 ).
Contrast-enhanced computed tomography showing a 30-mm hypovascular mass (arrow) behind the portal vein. a Axial image. b Coronal image.
Transgastric echoendoscopic image showing the obscure mass (arrow) with the intervening portal vein.
a Endoscopic ultrasound-guided tissue acquisition (EUS-TA) with an oblique-viewing echoendoscope was technically unfeasible due to positional difficulty. Hence, a decision was made to perform EUS-TA via the afferent limb using a forward-viewing echoendoscope instead. b Forward-viewing echoendoscope (TGF-UC260J; Olympus, Tokyo, Japan). c Fluoroscopic image showing the forward-viewing echoendoscope inserted into the afferent limb.
Endoscopic ultrasound-guided tissue acquisition. a EUS view of the hypoechoic mass (arrow) with B mode. b EUS view of the hypoechoic mass (arrow) using the color Doppler function. RHA, right hepatic artery. c Puncture of the mass under EUS guidance using a 22-gauge fine-needle biopsy needle. d Fluoroscopic image during EUS-TA.
Histopathological appearance, revealing adenocarcinoma.
Endoscopic ultrasound-guided tissue acquisition successfully performed via the afferent limb using a forward-viewing echoendoscope in a patient with previous pancreaticoduodenectomy with modified Child’s reconstruction.Video 1
In cases of hilar lesions after pancreaticoduodenectomy with Child’s reconstruction, EUS-TA using an oblique-viewing echoendoscope is often difficult because the lesion is far away since it is approached transgastrically. Use of a forward-viewing echoendoscope may enable safe insertion into the afferent limb and EUS-TA with a short puncture distance 5 .
Endoscopy_UCTN_Code_TTT_1AS_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tanaka K Hayashi T Utsunomiya R Endoscopic ultrasound-guided fine needle aspiration for diagnosing pancreatic mass in patients with surgically altered upper gastrointestinal anatomy Dig Endosc 20203296797310.1111/den.1362531912558 · doi ↗ · pubmed ↗
- 2Ban T Kawakami H Kubota Y Endoscopic ultrasonography-guided fine-needle biopsy from the pancreatic head of a patient with Roux-en-Y reconstruction Endoscopy 201850 E 202E 20410.1055/a-0624-131929895054 · doi ↗ · pubmed ↗
- 3Gong TT Zhang MM Zou DWEUS-FNA of a lesion in the pancreatic head using a forward-viewing echoendoscope in a patient with Billroth II gastrectomy (with video)Endosc Ultrasound 20221124324510.4103/EUS-D-21-0010135017384 PMC 9258016 · doi ↗ · pubmed ↗
- 4Ohno A Kaku T Kawabe K Fine-needle-aspiration using forward-viewing echoendoscope for the recurrence of intraductal tubulopapillary neoplasm Dig Endosc 202032 e 102e 10310.1111/den.1370032472606 · doi ↗ · pubmed ↗
- 5Iwashita T Nakai Y Lee JG Newly-developed, forward-viewing echoendoscope: a comparative pilot study to the standard echoendoscope in the imaging of abdominal organs and feasibility of endoscopic ultrasound-guided interventions J Gastroenterol Hepatol 20122736236710.1111/j.1440-1746.2011.06923.x 21916990 · doi ↗ · pubmed ↗