A modified transparent cap-assisted delivery method for capsule endoscopy
Yao Yi, Ting-Ting Cao, Tao Gan, Zhu Wang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
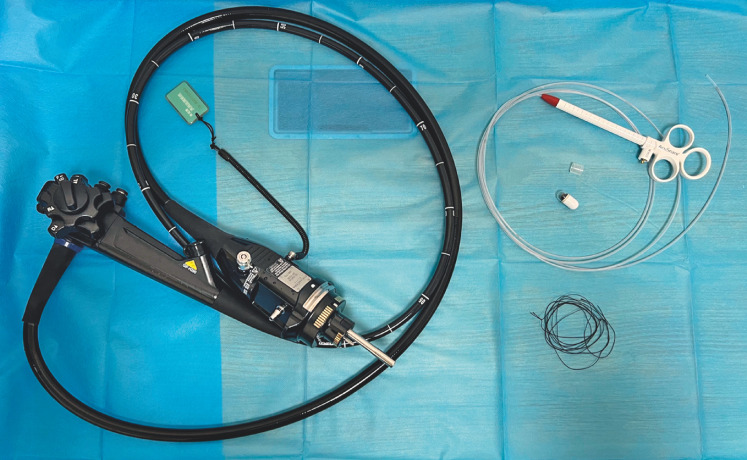 Fig. 1
Fig. 1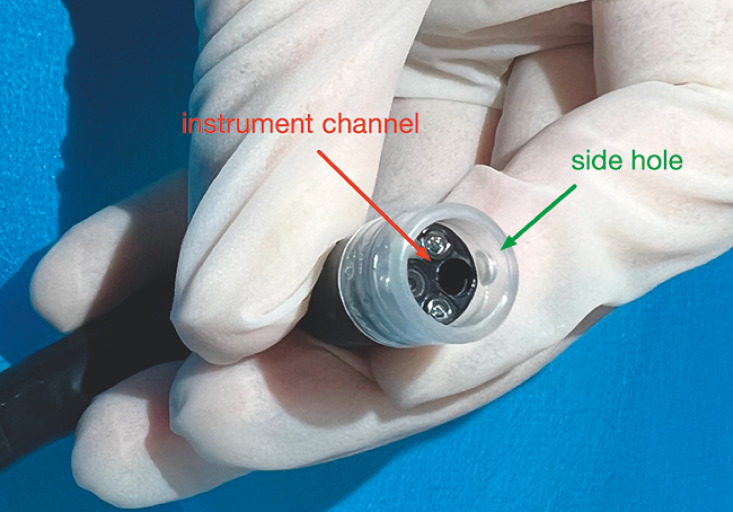 Fig. 2
Fig. 2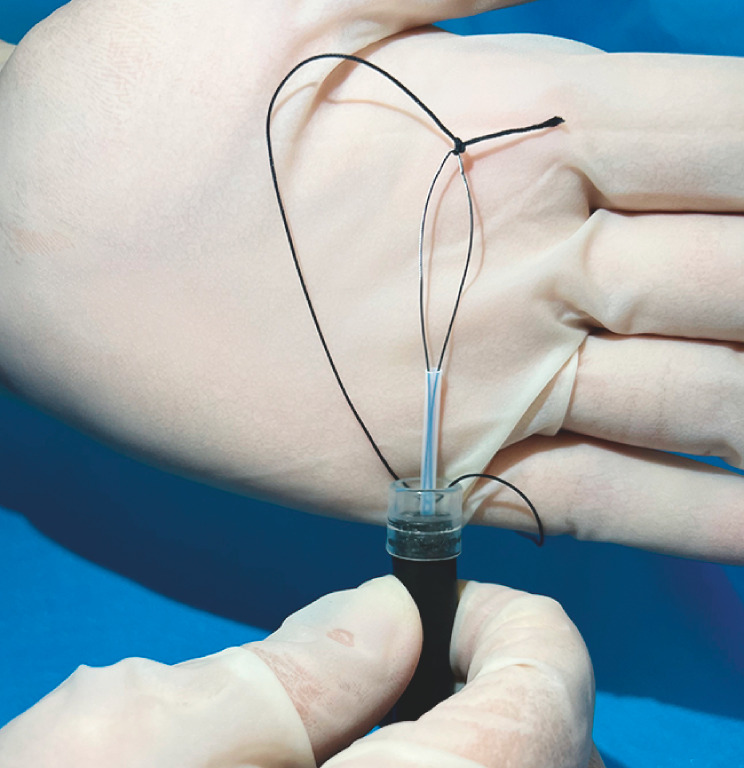 Fig. 3
Fig. 3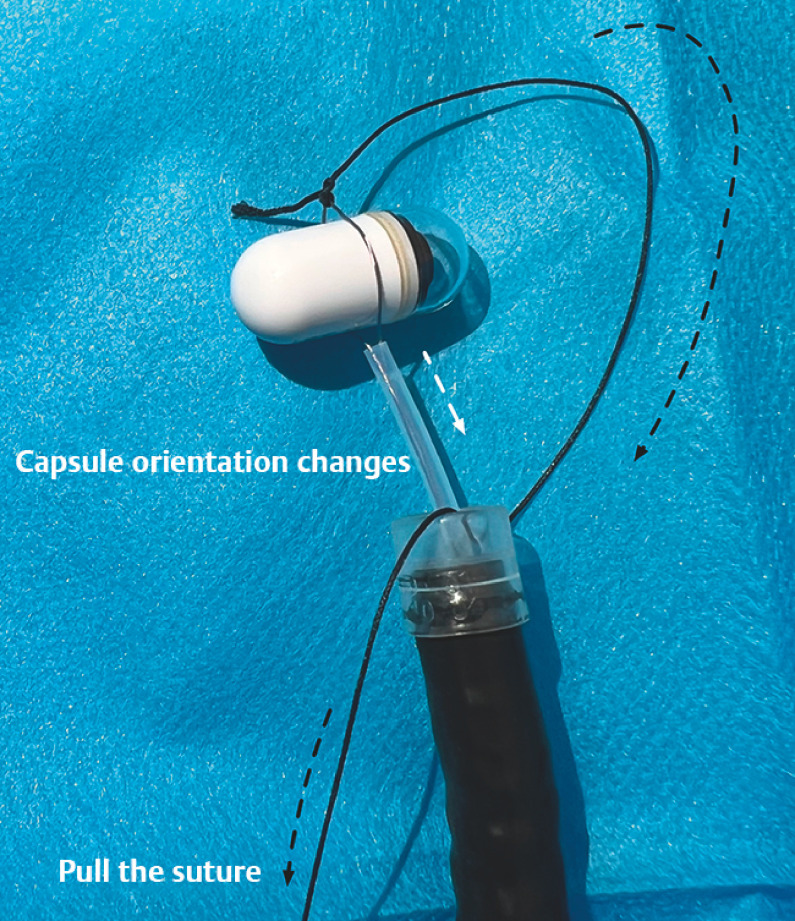 Fig. 4
Fig. 4 Fig. 5
Fig. 5- —Sichuan Science and Technology Program
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Bleeding Diagnosis and Treatment · Gastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment
Capsule endoscopy stands as the primary diagnosis method for small bowel observation. However, in patients with gastroparesis, pyloric stenosis, and altered anatomy, capsules may lodge in the esophagus or stomach after ingestion. For such instances of capsule stagnation, direct endoscopic deployment should be performed. Various accessories for this include the endoscopic retrieval net and the AdvanCE capsule delivery device (US Endoscopy, Mentor, Ohio, USA) 1 2 , but due to considerations of accessibility and cost, the polypectomy snares designed are frequently chosen in clinical settings. The standard practice involves using a snare to grasp the capsule and orient the capsule transversely. This orientation can pose difficulties in navigating narrow passageways like the esophageal inlet and pylorus.
A modified method is proposed to address this limitation. The approach requires a snare (SAS-1-S; Cook Medical, Bloomington, Indiana, USA ), a transparent cap (D-201-10704; Olympus, Tokyo, Japan), and surgical suture thread or dental floss ( Fig. 1 ). Initially, the transparent cap is positioned on the tip of the scope as usual, ensuring alignment of the cap’s side hole with the instrument channel of the scope ( Fig. 2 ). The suture is threaded through this hole and tied at the tip of the snare, which is inserted from the instrument channel ( Fig. 3 ). Experimentally, adjusting the capsuleʼs orientation into the longitudinal direction by pulling the suture has been shown to simplify insertion ( Fig. 4 , Fig. 5 ). Clinically, this longitudinal orientation, achieved via the cap and snare, facilitates smoother passage through the pylorus compared to the conventional transverse orientation. Supporting video evidence demonstrates the efficacy of this method ( Video 1 ).
The modified method requires a snare, a transparent cap, and a surgical suture.
The side hole (green arrow) of the transparent cap needs to be placed in line with the instrument channel (red arrow).
The surgical suture is threaded through the side hole of the transparent cap and tied at the tip of the snare.
The snare grasps the capsule and positions it transversely.
Pulling the suture (black arrow) changes the orientation of the capsule to the longitudinal direction (white arrow).
A modified transparent cap-assisted delivery method for capsule endoscopy.Video 1
In summary, this modified approach using a transparent cap may improve capsule delivery via a polypectomy snare, offering a practical and efficient solution to a common challenge in capsule endoscopy.
Endoscopy_UCTN_Code_TTT_1AO_2AL
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sumioka A Oka S Tsuboi A Endoscopic delivery method using a retrieval net for patients with small-bowel capsule endoscopy stagnation in the stomach Gastroenterol Res Pract 202120213.216193 E 610.1155/2021/3216193 PMC 870235234956361 · doi ↗ · pubmed ↗
- 2Ohmiya N Oka S Nakayama Y Safety and efficacy of the endoscopic delivery of capsule endoscopes in adult and pediatric patients: Multicenter Japanese study (Advan CE-J study)Dig Endosc 20223454355210.1111/den.1410434379849 · doi ↗ · pubmed ↗