The Relationship Between Breast Density and Breast Cancer Surgical Outcomes: A Systematic Review
Yousef Alalawi, Sultan Abdulrahman S Alamrani, Omar M Alruwaili, Ibrahim F Alzahrani, Abdullah M Al Madshush

TL;DR
This study reviews how breast density relates to surgical outcomes in breast cancer patients, finding mixed evidence on its impact.
Contribution
A systematic review of breast density's role in surgical outcomes, highlighting inconsistent associations across studies.
Findings
Low breast density is linked to fewer preoperative and intraoperative challenges and lower local recurrence.
Breast density shows no clear link to disease recurrence, survival, or re-excision in some studies.
Further research is needed to clarify breast density's role in breast cancer outcomes.
Abstract
This study aims to investigate the relationship between mammographic breast density and the surgical outcomes of breast cancer. PubMed, SCOPUS, Web of Science, Science Direct, and the Wiley Library were systematically searched for relevant literature. Rayyan QRCI was employed throughout this comprehensive process. Our results included ten studies with a total of 5017 women diagnosed with breast cancer. The follow-up duration ranged from 1 year to 15.1 years. Eight out of the twelve included studies reported that low mammographic breast density was significantly associated with no local recurrence, metachronous contralateral breast cancer, and fewer challenges in the preoperative and intraoperative phases. On the other hand, four studies reported that mammographic breast density is not linked to disease recurrence, survival, re-excision, or an incomplete clinical and pathological…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
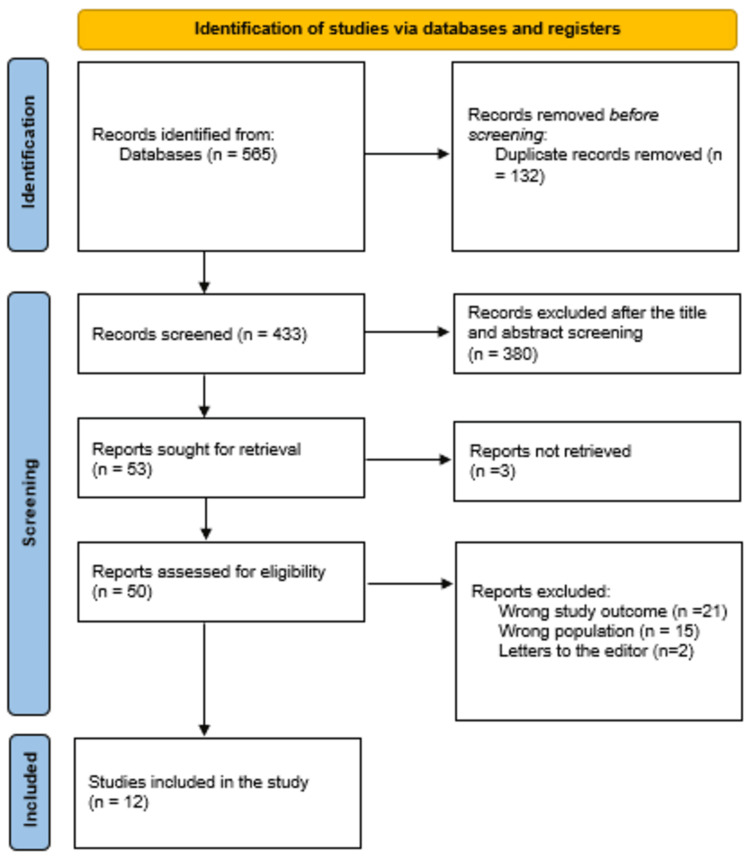 Figure 1
Figure 1| Study | Study design | Country | Participants | Mean age |
| Eriksson et al. [ | Case-control | Sweden | PD <25% (n = 1,329) PD ≥25% (n = 445) | 50-74 |
| Cil et al. [ | Case-control | Canada | Low density (99), intermediate density (107), high density (129) | 63.5 |
| Faermann et al. [ | Case-control | Canada | 165 dense and 105 not dense | 50.2 |
| Edwards et al. [ | Case-control | USA | Fatty (n = 80, 20.1 %), scattered (n = 170, 42.7 %), heterogeneous (n = 121, 30.4 %), and extreme (n = 27, 6.7%) | 42-71 |
| Bani et al. [ | Prospective cohort | Germany | 565 | 55.8 ± 11.6 |
| Zdanowski et al. [ | Retrospective cohort | Sweden | 302 | 41-68 |
| Park et al. [ | Case-control | USA | 136 | NM |
| Huang et al. [ | Case-control | Taiwan | 121 cases and 121 control | 51.4 |
| Sadaka et al. [ | Case-control | Egypt | 23 with low breast density and 64 high breast density | NM |
| Kim et al. [ | Retrospective cohort | Korea | Recurrence group (12) and nonrecurrence (68) | 44.4 ± 6.5 |
| Walsh et al. [ | Case-control | USA | Minimum density 1/2 (n = 487) 3/4 (n = 214 | 28-90 |
| Agarwal et al. [ | Case-control | Australia | 127 | 28-97 |
| Study | Follow-up duration (years) | Menopausal status | Type of surgery | Patient outcome | Main outcomes | JBI |
| Eriksson et al. [ | 10 | Post-menopausal | Breast conservative surgery and mastectomy | Local recurrence and locoregional recurrence | Elevated mammography density is a risk factor for local and locoregional recurrence, not related to distant metastases or survival. | Moderate |
| Cil et al. [ | 0.9–15.1 | The majority 219 (65.4%) are postmenopausal | Breast conservative surgery | Local recurrence | The study found no local disease recurrence among 34 women with poor breast density who did not undergo radiation, indicating that their decision to forgo radiation was not impaired. | Moderate |
| Faermann et al. [ | 6 | NM | Mastectomy | local recurrence, re-excision, involved margins, metachronous contralateral breast cancer, late distant recurrence, and death | Preoperative breast magnetic resonance imaging in dense breast patients may improve long-term and surgical outcomes, with lower incidence of local recurrence and metachronous contralateral breast cancer, and fewer re-excision operations, though the difference is not statistically significant. | High |
| Edwards et al. [ | 1 | NM | Breast conservative surgery | Re-excision | The study found no significant impact of mammographic density on margin involvement, conversion to mastectomy, or extra margin removal during breast conservative surgery, suggesting that mammographic density should not influence surgical decisions. | Moderate |
| Bani et al. [ | NM | NM | Breast conservative surgery | Recurrence | Mammographic density is a key risk indicator in breast-conserving therapy, as higher density increases challenges in tumor localization and removal. | Moderate |
| Zdanowski et al. [ | 3.4 | Majority were postmenopausal | The type of surgery was not detected | Recurrence and survival | A study found that patients with very dense breasts had lower recurrence-free and breast cancer-specific survival rates compared to those with less dense breasts. | Moderate |
| Park et al. [ | 7.7 | NM | Breast conservative surgery | Local recurrence | High mammographic breast density predicts local recurrence after breast conservative surgery and radiotherapy, but not distant recurrence. Obesity and high mammographic breast density have a negative confounding. | High |
| Huang et al. [ | 7 | Majority were >50 years | Modified radical mastectomy | Local recurrence | For invasive breast cancer, high mammographic breast density (>50% density) is a strong independent predictor of local recurrence following Modified radical mastectomy. | High |
| Sadaka et al. [ | More than half (55.2%) were above 50 years | Modified radical mastectomy | Local recurrence | The local recurrence of invasive breast cancer in female patients is significantly influenced by mammographic breast density. | Moderate | |
| Kim et al. [ | 3.1-5 | 15 (18.75%) were postmenopausal | Breast conservative surgery and received adjuvant tamoxifen treatment | Recurrence | Breast cancer patients receiving adjuvant tamoxifen showed changes in breast density as an independent risk factor for cancer recurrence, as determined by 3D magnetic resonance imaging before and after treatment. | Moderate |
| Walsh et al. [ | 0–5.3 | NM | Breast conservative surgery | Re-excision | The study found that while women with thick breasts are more likely to need surgery, their breast density did not negatively affect their disease-free survival. | Moderate |
| Agarwal et al. [ | 9.3 | NM | Breast conservative surgery | Clinical and pathological response | High mammographic breast density is not linked to pathologic complete response or breast cancer death, but rather to a lesser clinical complete response and a higher rate of relapse. | Moderate |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDigital Radiography and Breast Imaging · Breast Cancer Treatment Studies · AI in cancer detection
Introduction and background
Breast cancer continues to be the most often diagnosed cancer globally and the second leading cause of cancer-related death for women. The American Cancer Society predicts that, in 2024, approximately 310,720 new cases of invasive breast cancer will be diagnosed in women, along with about 56,500 new cases of ductal carcinoma in situ (DCIS). Tragically, an estimated 42,250 women are expected to lose their lives to breast cancer [1]. Screen film mammography has been mostly replaced with digital mammography in the last ten years, with mammography still being the modality utilized in ordinary clinical practice for screening and diagnosis. However, because mammography exposes patients to cumulative low-level X-ray radiation, it is not the best method for measuring breast density. A great deal of research has been done on alternative modalities, chief among these being digital breast tomosynthesis and magnetic resonance imaging [2,3].
Due to the different radiographic attenuation characteristics of fibroglandular tissue versus fat, mammographic density refers to the percentage of opaque (white) dense breast tissue compared to the radiolucent (dark) areas seen on mammography [4]. Mammographic density is typically expressed as a percent, which is computed by dividing the dense area by the total breast area [5].
Numerous studies have looked into the relationship between mammographic density and treatment outcomes as well as prognosis [6-8]. Different findings, meanwhile, have been produced by this research about the correlation between mammographic density characteristics and patient outcomes. Research indicates that there are ethnic differences in treatment response and breast cancer mortality [9,10], as well as a 20-30% variance in mammographic density that coincides with variation in breast cancer incidence [11]. It is unclear, though, if ethnic differences or the mammographic density phenotype that was utilized are confusing the link between mammographic density and the result. Crucially, nothing is known about how mammographic density modifications affect the nature and results of breast cancer treatment. Despite the aforementioned gaps, no evaluation of the literature has been done to determine the actual effects of mammographic breast density and mammographic density reduction after cancer treatment on the prognosis of women who have been diagnosed with or are receiving treatment for breast cancer. This highlights the necessity of conducting a thorough examination of published research to determine the connection between mammographic density and treatment results. The main objective of this comprehensive review is to investigate the relationship between breast density and the surgical outcomes of breast cancer.
Review
The present systematic review adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) standards [12].
Study design and duration
January 2024 marked the start of this systematic review.
Search strategy
Articles were determined through five main databases: PubMed, SCOPUS, Web of Science, Science Direct, and Wiley Library to comprise relevant data. We limited our search to English and considered each database's specific needs. The following keywords were transformed into PubMed Mesh terms or subject terms in Scopus and used to locate the pertinent studies: "Breast cancer," "Breast density," "Mammographic density," "Surgical outcomes," "Survival," "Recurrence," and "Re-excision." The Boolean operators "OR" "AND" and "NOT" matched the required keywords. Publications with full English text, available free articles, and human trials were among the search results.
Eligibility criteria
Inclusion Criteria
We considered articles that studied the relationship between mammographic breast density and the surgical outcomes of breast cancer and any study design discussing the required outcomes for inclusion in this review. Adults (>18 years), only human subjects, English language, and free, accessible articles were included.
Exclusion Criteria
In our evaluation approach, we excluded case reports, unpublished data, reviews, letters, conference abstracts, and insufficient data. After the investigators finished their eligibility review, any disagreements were discussed and resolved by the authors.
Data extraction
The outcomes of the search technique were verified twice with Rayyan QCRI [13]. The researchers added inclusion/exclusion criteria to the aggregated search results in order to evaluate the relevance of the titles and abstracts. The reviewers thoroughly read all of the papers that met the inclusion criteria. The authors talked about how to settle arguments. A previously developed data extraction form was used to upload the approved study. The authors extracted data about the study titles, authors, study year, country, participants, follow-up, menopausal status, type of surgery, patient outcome, and main outcomes. A separate sheet was created for the risk of bias assessment.
Strategy for data synthesis
The summary tables created utilizing information from relevant studies provide a qualitative assessment of the research findings and their constituent parts. The best technique for making use of the data from the included study articles was chosen after the data for the systematic review was gathered.
Risk of bias assessment
The Joanna Briggs Institute's (JBI) [14] key assessment criteria for studies providing prevalence data were applied in order to evaluate the research's quality. This technique was used to evaluate studies using nine questions. The question was given a score of 1 if the answer was in the affirmative. Any response that was no, unclear, or not applicable received a score of 0. For overall quality, ratings of less than 4, 5 to 7, and more than 8 were regarded as low, moderate, and high quality, respectively. The scholars assessed the caliber of the research they carried out, and disagreements were settled by discussion.
Results
The systematic search yielded a total of 565 study articles, of which we deleted 132 duplicates. Title and abstract screening were conducted on 433 studies, and 380 were excluded. We retrieved 53 reports and excluded only 3 articles. Finally, 50 studies were screened for full-text assessment; 21 were excluded for the wrong study outcomes, 15 for the wrong population type, and 2 articles were letters to the editors. Twelve eligible study articles were included in this systematic review. A summary of the study selection process is presented in Figure 1.
PRISMA flowchart summarizes the study selection process.PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Table 1 presents the sociodemographic characteristics of the included study articles [15-26]. Our results included 12 studies, with 5017 women diagnosed with breast cancer. Nine studies were case-control studies [15-18,21-23,25,26], two were retrospective in nature [20,24], and one was prospective in nature.
Table 2 presents the clinical characteristics. The follow-up duration ranged from 1 year [18] to 15.1 years [16]. Eight out of the twelve included studies reported that low mammographic breast density was significantly associated with no local recurrence, metachronous contralateral breast cancer, and fewer challenges in the preoperative and intraoperative phases [16,17,19-24]. On the other hand, four studies reported that mammographic breast density is not linked to disease recurrence, survival, re-excision, or an incomplete clinical and pathological response [15,18,25,26].
Discussion
The available research indicates a dearth of information about surgical outcomes in particular and contradictory findings when using mammographic density to evaluate the course of breast cancer treatment. A number of factors, such as mammographic breast density assessment techniques, study design, sample selection, mammographic breast density measurement time, surgical type, varying follow-up lengths, and confounder adjustment, could account for the contradictory data. To use data collected from radiological imaging for breast cancer prediction and treatment efficacy monitoring, a deeper comprehension of these parameters and their implications is necessary.
This review demonstrated that low mammographic breast density was significantly associated with no local recurrence, no metachronous contralateral breast cancer, higher survival rates, and fewer challenges in the preoperative and intraoperative phases [16,17,19-24]. Similarly, Kanbayti et al., in their systematic review and meta-analysis, reported that there is limited evidence to suggest that having a high baseline mammographic breast density raises the risk of breast cancer mortality, complete blood count, and recurrence. On the other hand, mammographic breast density reduction is linked to a lower incidence of complete blood count, breast cancer-related mortality, and breast cancer recurrence. These results present a promising picture of the effectiveness of mammographic breast density for evaluating breast cancer treatment outcomes or enhancing the functionality of the available models for predicting breast cancer treatment outcomes [27].
The ability of dense breasts to limit drug delivery to the tumor site [28], the existence of residual tumor volumes in extremely dense breasts compared to fatty breasts [18], and the increased risk of cancer in dense breast women [22] are some of the theories put forth to explain the low recurrence in dense breasts.
Crucially, in order to use mammographic density reduction as a stand-in marker for treatment outcomes, we need to pinpoint the metrics or phenotypes that most accurately reflect changes in mammographic breast density, particularly alterations in the fibroglandular tissue composition, which is the primary tissue that affects outcomes. Mammographic density reduction has been linked to better results in other phenotypes, but there are not nearly enough data to make firm judgments. Three investigations have demonstrated that, in women for whom area-based approaches were unable to detect changes in mammographic breast density following endocrine therapy, volumetric assessments from mammograms and magnetic resonance imaging could [29-31]. However, this research did not examine the patient outcome from such a reduction in mammographic breast density. Consequently, more research is required to evaluate the connection between variations in volumetric density and patient outcomes. Considering that volumetric instruments need raw data, which can be challenging to get, automated mammographic breast density measurement techniques that take area and depth data into consideration ought to be investigated. These methods could provide a more accurate evaluation of mammographic breast density reduction as a factor influencing patient outcomes. Results may vary depending on therapy interventions, length of treatment, and treatment regimes. The majority of the examined studies have limitations because they failed to take these parameters' impact on the relationship between mammographic breast density and treatment results into consideration. Furthermore, it was challenging to determine if mammographic breast density is an independent or intermediate marker of treatment outcome because nearly all of the research examined relationships with minimal focus on outcome prediction.
On the other hand, four studies reported that mammographic breast density is not linked to disease recurrence, survival, re-excision, or an incomplete clinical and pathological response [15,18,25,26]. Tracking changes in density is complicated by the short follow-up intervals in published studies. Based on the observation that individuals with low mammographic breast density saw slight reductions that could not have been enough to affect mortality, it seems that mammographic breast density is another crucial factor to take into account [32,33]. Further research should be done on the possibility that racial characteristics contribute to the negative correlation between mammographic density reduction and recurrence [24].
Conclusions
Low mammographic breast density is significantly associated with reduced challenges in the preoperative and intraoperative phases, no local recurrence, and fewer mastectomy cases. However, the link between mammographic breast density and disease recurrence, survival, re-excision, and incomplete clinical and pathological response is less clear, with some studies reporting no significant association. The findings suggest that mammographic breast density may play a role in certain aspects of breast cancer outcomes, but further research is needed to fully understand its impact.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cancer facts and figures 20242024 1 2024 American Cancer Society 20242024 https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2024/2024-cancer-facts-and-figures-acs.pdf
- 2Current and future methods for measuring breast density: a brief comparative review Breast Cancer Manag Sak MA Littrup PJ Duric N Mullooly M Sherman ME Gierach GL 209221420152894389310.2217/bmt.15.13PMC 5609705 · doi ↗ · pubmed ↗
- 3Looking beyond the mammogram to assess mammographic density: A narrative review Biomed Spectrosc Imaging Hugo HJ Tourell MC O’Gorman PM 6380720181
- 4Mammographic density and the risk and detection of breast cancer N Engl J Med Boyd NF Guo H Martin LJ 22723635620071722995010.1056/NEJ Moa 062790 · doi ↗ · pubmed ↗
- 5Percent mammographic density and dense area as risk factors for breast cancer Geburtshilfe Frauenheilkd Rauh C Hack CC Häberle L 7277337220122525846510.1055/s-0032-1315129 PMC 4168400 · doi ↗ · pubmed ↗
- 6Very low mammographic breast density predicts poorer outcome in patients with invasive breast cancer Eur Radiol Masarwah A Auvinen P Sudah M 187518822520152573551210.1007/s 00330-015-3626-2 · doi ↗ · pubmed ↗
- 7Mammographic density reduction as a prognostic marker for postmenopausal breast cancer: results using a joint longitudinal-survival modeling approach Am J Epidemiol Andersson TM Crowther MJ Czene K Hall P Humphreys K 1065107318620172863332410.1093/aje/kwx 178PMC 5860633 · doi ↗ · pubmed ↗
- 8Minimal impact of adjuvant exemestane or tamoxifen treatment on mammographic breast density in postmenopausal breast cancer patients: a Dutch TEAM trial analysis Acta Oncol van Nes JG Beex LV Seynaeve C 3493605420152538345110.3109/0284186 X.2014.964809 · doi ↗ · pubmed ↗