Swallowing Function and Quality of Life in Patients Treated With Transoral Videolaryngoscopic Surgery for Pharyngolaryngeal Cancer
Koji Ebisumoto, Akihiro Sakai, Hiroaki Iijima, Fumiyuki Goto, Mayu Yamauchi, Daisuke Maki, Takanobu Teramura, Koichiro Wasano, Kenji Okami

TL;DR
This study examines how transoral surgery affects swallowing and quality of life in patients with throat cancer, finding that most maintain good function, though elderly patients are at higher risk for issues.
Contribution
The study provides evidence that transoral videolaryngoscopic surgery preserves swallowing function in most patients, with age being a key risk factor for impairment.
Findings
Most patients maintained good swallowing function after TOVS with favorable FOSS scores.
Age ≥65 years was a significant predictor of impaired swallowing function post-surgery.
Elderly patients with laryngeal hypoesthesia and poor clearance are at higher risk for swallowing dysfunction.
Abstract
Background: It is controversial whether transoral resection for early pharyngolaryngeal cancer preserves swallowing function and quality of life. We investigated swallowing function and quality of life before and after transoral videolaryngoscopic surgery (TOVS). Methods: Seventy-three patients with pharyngolaryngeal cancer who underwent TOVS between July 2012 and July 2022 were enrolled in this prospective analysis. The Hyodo score and European Organization for Research and Treatment of Cancer Quality of Life Questionnaires were recorded preoperatively and at three, six, and 12 months postoperatively, in addition to the postoperative functional outcome swallowing scale (FOSS) at six months postoperatively. Results: Although most patients could consume food orally without restrictions with a preferable FOSS score, 23 patients showed impaired Hyodo scores. Age ≥65 years significantly…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
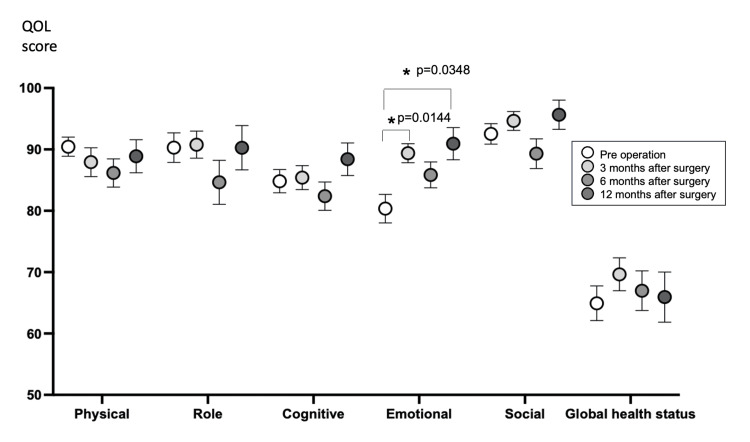 Figure 1
Figure 1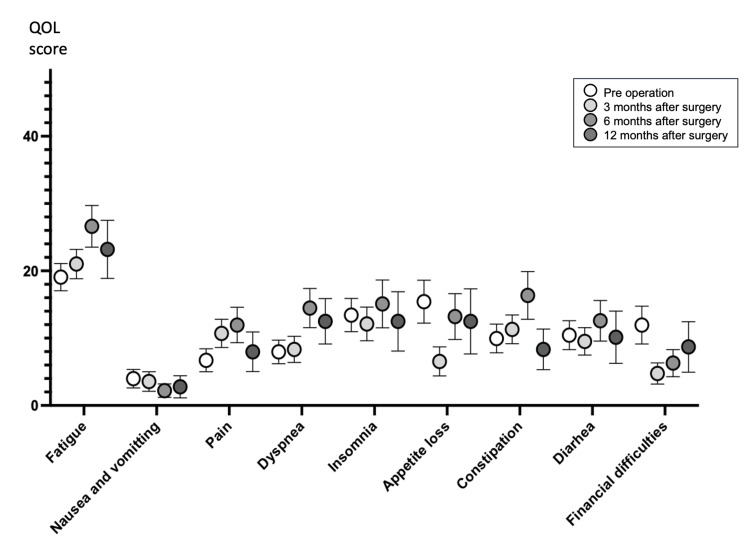 Figure 2
Figure 2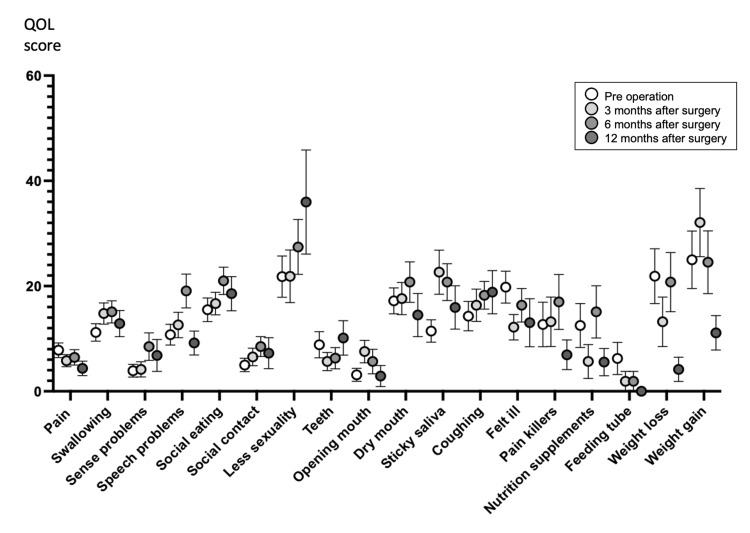 Figure 3
Figure 3| (1) The salivary pooling degree at the vallecula and piriform sinuses | |
| 0 | No pooling |
| 1 | Pooling at the only vallecula |
| 2 | Pooling in vallecula and piriform sinus and no penetration into larynx |
| 3 | Pooling in vallecula and piriform sinus and penetration into larynx |
| (2) The glottal closure reflex induced by touching the epiglottis or arytenoid with the endoscope | |
| 0 | Marked reflex by one touching |
| 1 | Slow and/or weak reflex by one touching |
| 2 | Reflex by two or three touching |
| 3 | No reflex despite three touching |
| (3) The location of the bolus at the swallowing reflex initiation assessed by “white-out” timing | |
| 0 | Pharyngeal |
| 1 | Vallecula |
| 2 | Piriform sinuses |
| 3 | No swallowing |
| (4) The extent of pharyngeal clearance after blue-dyed water is swallowed | |
| 0 | No residue |
| 1 | Pharyngeal residues remain, but are absent after swallowing is attempted two or three times |
| 2 | Pharyngeal residues remain, but no penetration into larynx |
| 3 | Pharyngeal residues remain, and penetration into larynx |
| Age, median (IQR), years | 71 (61-74) | ||
| Sex | |||
| Male/female | 59/14 | ||
| BMI, median (IQR), kg/m2 | 20.845 (19.05-23.77) | ||
| Primary site | |||
| Supraglottis (n=9) | Epiglottis | 4 | |
| Arytenoid | 5 | ||
| Hypopharynx (n=38) | Piriform sinus | 25 | |
| Posterior wall | 9 | ||
| Post cricoid | 2 | ||
| Piriform sinus to posterior wall | 2 | ||
| Orophrynx (n=32) | Tonsil (p16+) | 19 (14) | |
| Base of tongue (p16+) | 3 (0) | ||
| Superior wall | 6 | ||
| Lateral wall | 1 | ||
| Posterior wall | 3 | ||
| T classification | |||
| T1 | 49 | ||
| T2 | 30 | ||
| Multiple lesions | 6 | ||
| Lymph node metastasis | 14 | ||
| Neck dissection | 16 | ||
| Tracheostomy | 2 | ||
| Postoperative irradiation | 2 | ||
| Cancer history | |||
| Head and neck cancer (n=20) | Extended resection | 2 | |
| Neck dissection | 4 | ||
| Transoral resection | 12 | ||
| Irradiation | 6 | ||
| Esophageal cancer (n=35) | Extended resection | 23 | |
| Endoscopic resection | 13 | ||
| Irradiation | 5 | ||
| FOSS stage | Number of patients |
| 0 | 61 |
| 1 | 10 |
| 2 | 2 |
| Pre-operation (mean±SE) | 3 months (mean±SE) | 6 months (mean±SE) | 12 months (mean±SE) | P-value | |
| Salivary pooling degree at the vallecula and piriform sinuses | 0.41±0.067 | 0.31±0.065 | 0.38±0.077 | 0.38±0.112 | 0.959 |
| Glottal closure reflex induced by touching the epiglottis or arytenoid with endoscope | 0.31±0.080 | 0.33±0.076 | 0.36±0.081 | 0.19±0.079 | 0.746 |
| Location of bolus at swallowing reflex initiation assessed by “white-out” timing | 0.53±0.070 | 0.42±0.074 | 0.51±0.083 | 0.31±0.092 | 0.368 |
| Extent of pharyngeal clearance after swallowing blue-dyed water | 0.38±0.069 | 0.48±0.105 | 0.35±0.076 | 0.19±0.148 | 0.428 |
| Total Hyodo score | 1.63±0.196 | 1.54±0.235 | 1.53±0.233 | 1.52±0.256 | 0.880 |
| number of patients | 64 | 52 | 53 | 25 |
| Variables | Odds ratio | 95% Confidence Interval | P-value |
| Age | |||
| <65 | Reference | ||
| ≥65 | 4.583 | 1.203-17.454 | 0.026 |
| Body mass index | |||
| ≥18.5 | Reference | ||
| <18.5 | 1.246 | 0.296-5.236 | 0.764 |
| Primary lesion | |||
| Supraglottis/ Hypopharynx | Reference | ||
| Oropharynx | 0.62 | 0.151-2.547 | 0.507 |
| T classification | |||
| T1 | Reference | ||
| T2 | 0.836 | 0.193-3.627 | 0.811 |
| Neck Dissection | |||
| No | Reference | ||
| Yes | 1.121 | 0.209-6.007 | 0.894 |
| History of head and neck cancer | |||
| No | Reference | ||
| Yes | 2.023 | 0.371-11.026 | 0.416 |
| Irradiation history for head and neck | |||
| No | Reference | ||
| Yes | 0.59 | 0.048-7.269 | 0.68 |
| History of esophageal cancer | |||
| No | Reference | ||
| Yes | 0.265 | 0.055-1.272 | 0.097 |
| Pre operation (mean±SE) | 3months (mean±SE; P-value) | 6months (mean±SE; P-value) | 12months (mean±SE; P-value) | P-value | |
| 1. The salivary pooling degree at the vallecula and piriform sinuses | 0.348±0.102 | 0.619±0.011; 0.2579 | 0.571±0.130; 0.6134 | 0.636±0.203; 0.6086 | 0.321 |
| 2. The glottal closure reflex induced by touching the epiglottis or arytenoid with the endoscope | 0.043±0.043 | 0.619±0.146; .0015 | 0.477±0.148; 0.0374 | 0.182±0.122; >0.9999 | 0.003 |
| 3. The location of the bolus at the swallowing reflex initiation assessed by “white-out” timing | 0.435±0.123 | 0.762±0.118; 0.1291 | 0.714±0.122; 0.2524 | 0.364±0.152; >0.9999 | 0.076 |
| 4. The extent of pharyngeal clearance after blue-dyed water is swallowed | 0.214±0.088 | 0.857±0.199; 0.0196 | 0.524±0.131; 0.3147 | 0.727±0.237; 0.1487 | 0.039 |
| Hyodo Score | 1.043±0.231 | 2.857±0.367; 0.0002 | 2.286±0.332; 0.008 | 1.909±0.415; 0.2286 | 0.0005 |
| number of patients | 23 | 21 | 21 | 11 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Cancer Studies · Dysphagia Assessment and Management · Head and Neck Surgical Oncology
Introduction
Head and neck cancer requires multidisciplinary treatment with surgery, radiation therapy, and chemotherapy. In surgical treatment, especially extended resection, organ loss is directly related to loss of function and quality of life (QOL). However, even when chemoradiotherapy is used for organ preservation [1], serious late complications such as jaw osteonecrosis, dysphagia, persistent dry mouth, sticky saliva, and tooth decay are problematic. Organ preservation does not always mean functional preservation, which may have a rather negative impact on long-term prognosis [2,3]. Therefore, minimally invasive treatments aimed at preserving function are attracting attention and transoral resection is a promising surgical strategy. The primary surgical technique is transoral robotic surgery (TORS), which is primarily used to treat oropharyngeal cancer [4,5]. In recent years, the incidence of human papillomavirus-associated cancers has increased significantly [6], especially in developed countries, and these cancers tend to occur in the palatine and lingual tonsils compared to classic head and neck cancers. The number of TORS cases is increasing due to an increase in the number of oropharyngeal cancers [7].
TORS has only been covered by insurance in Japan since April 2022. Therefore, it has not yet gained popularity. However, efforts have focused on the early diagnosis and treatment of head and neck cancer as a double primary cancer with esophageal cancer [8]. In recent years, Japan has made notable progress in endoscopic imaging techniques, particularly with advancements like narrow-band imaging (NBI), enabling the early detection of pharyngeal cancer ahead of other countries [9]. Within this context, there has been the development of endoscopic laryngopharyngeal surgery (ELPS) as an advanced form of endoscopic esophageal cancer surgery [10]. Additionally, transoral videolaryngoscopic surgery (TOVS) has emerged, building upon traditional videolaryngoscopic surgical techniques [11]. The evolution of optical devices and surgical instruments has positioned non-robotic surgery as a crucial component of transoral surgery in Japan, recognized for its efficacy and minimally invasive nature [12-14]. Notably, at our institution, TOVS has been utilized for transoral resection of pharyngolaryngeal cancer since 2012.
While there are reports of good postoperative swallowing function in both TORS [15,16] and TOVS [17], a recently published study showed that the QOL related to swallowing function in patients treated with both TORS and radiotherapy was worse than that in patients given radiotherapy alone [18], which is controversial. Since there are few reports on the quantitative evaluation of swallowing function and QOL with transoral resection, we conducted a prospective survey on the pre- and postoperative swallowing function and QOL of patients treated with TOVS at our department.
Materials and methods
This research adhered to the principles of the Declaration of Helsinki, and the protocol entitled “Functional evaluation for the patients with head and neck cancer and dysphagia” received approval from the institutional review board of Tokai University, number 08-R98 (approved on February 3, 2009) and 18R256 (approved on February 19, 2019). Although both studies were identical, they were reexamined at the direction of the Institutional Review Board due to the extended duration of the study. Every participant in this study gave their informed consent for inclusion.
Out of the individuals who underwent transoral TOVS for pharyngolaryngeal cancer at our department from July 2012 to July 2022, a total of 73 patients who gave their consent for participation in the prospective study were included. The inclusion criteria comprised individuals aged 18 years or older with an Eastern Cooperative Oncology Group performance status (ECOG PS) of 0. The exclusion criteria were patients younger than 18 years, ECOG PS ≥1, and those deemed inappropriate by the physician, such as those with obvious aspiration pneumonia or incapacity to consent. The eighth edition of the Union for International Cancer Control guidelines was used to classify the TNM stage.
The Functional Outcome Swallowing Scale (FOSS) [19] was recorded at six months postoperatively. The Hyodo score [20], using flexible endoscopic evaluation of swallowing (FEES) and European Organization for Research and Treatment of Cancer Quality of Life questionnaires (EORTC QLQ C30, EORTC QLQ H&N35) [21,22] was also recorded preoperatively and three, six, and 12 months postoperatively. The patients were classified into two groups according to whether their postoperative Hyodo score was impaired. To evaluate the predictors of worsening Hyodo score, logistic regression analysis was performed with the following predictor variables: age (≥65 years), preoperative body mass index (BMI, <18.5 kg/m^2^), primary lesion, T classification, with or without neck dissection, history of head and neck cancer, history of irradiation for head and neck, and history of esophageal cancer.
Surgical indication
Criteria for considering TOVS included the following: (1) presence of primary lesions in the oropharynx, hypopharynx, or supraglottis; (2) clinical presentation of T1 or T2 lesions; (3) absence of lymph node metastasis or presence of resectable cervical lymph node metastasis; (4) limited to within half circumferential extension; and (5) absence of distant metastases.
Exclusion criteria encompassed: (1) indications of suspected invasion on imaging studies, including the hyoid bone, thyroid cartilage, and cricoid cartilage; (2) invasion into deep tissue adjacent to the constrictor muscle or posterior invasion of the deep vertebral fascia; (3) ECOG PS of ≥ 2; (4) severe cardiopulmonary impairment; and (5) factors that might impede transoral resection, such as trismus.
Surgical procedure
The surgical approach followed the TOVS method outlined by Tomifuji et al. [14,17]. To create the surgical field, either the FK-WO retractor (Olympus Medical Systems, Tokyo, Japan) or the Weerda distending laryngoscope (Karl Storz, Tuttlingen, Germany) was utilized. Visualization of the surgical field employed a video endoscope with a movable tip, such as the OLYMPUS LTF-S190-5 or ENDOEYE FLEX 3D (Olympus Medical Systems). Electrocautery was performed using a Colorado microdissection needle (Stryker Japan KK, Tokyo, Japan) or a malleable electrocautery needle (KD 600, Olympus Medical Systems). Grasping forceps included STEINER grasping forceps, LARYNGOFORCERII grasping forceps (Karl Storz, Tuttlingen, Germany), and a MicroFrance Heart-Shaped grasper (Integra MicroFrance, Saint Aubin le Monial, France).
Lesion confirmation utilized Narrow-Band Imaging (NBI) systems and iodine-staining techniques. Tumors were resected en bloc with a safety margin of 5-10 mm. Fibrin glue and polyglycolic acid sheets were applied to cover mucosal defects [23].
Neck dissection was performed in cases with cervical lymph node metastases, while tracheostomy was not performed as a routine procedure. Postoperative radiotherapy or chemoradiotherapy was considered when adverse features were confirmed through histopathological examination after surgery.
Evaluation of Hyodo score with fiberoptic endoscopic examination of swallowing (FEES)
FEES can be performed in conjunction with a laryngeal fiberscope, which is a procedure frequently used by otolaryngologists and head and neck surgeons. The Hyodo score consists of four sub-scores: (1) the salivary pooling degree at the vallecula and piriform sinuses, (2) the glottal closure reflex induced by touching the epiglottis or arytenoid with the endoscope, (3) the location of the bolus at the swallowing reflex initiation assessed by “white-out” timing, and (4) the extent of pharyngeal clearance after blue-dyed water is swallowed. These four sub-scores are rated on a four-point scale from 0-3, and the sum of the four sub-scores is the Hyodo score [20]. The scoring criteria for each sub-score are shown in Table 1. This simple scoring system has moderate sensitivity and high specificity for predicting aspiration, which provides information on whether patients are capable of oral intake, and is considered a strong predictor of aspiration when the score exceeds 6 [20]. The FEES was performed in open-label and the bolus used for the test was liquid (blue dyed water). It was evaluated by at least two head and neck surgeons and a certified nurse in nursing care of dysphagia.
Evaluation of FOSS
The degree of dysphagia was evaluated using the FOSS six months after surgery. The FOSS categorizes swallowing function into six stages as follows: stage 0, normal function and asymptomatic; stage 1, normal function with episodic or daily symptoms of dysphagia; stage 2, compensated abnormal function manifested by significant dietary modifications or prolonged mealtimes but without weight loss or aspiration; stage 3, decompensated abnormal function with weight loss of less than 10% of body weight over six months caused by dysphagia or daily coughing, gagging, or aspiration during meals; stage 4, severely decompensated abnormal function with weight loss exceeding 10% of bodyweight over 6 months caused by dysphagia or severe aspiration with bronchopulmonary complications; and stage 5, non-oral feeding for all nutrition [19].
Statistical analysis
The Kruskal-Wallis test was used to compare the mean rank of each timepoint. Dunn’s test was employed for multiple comparisons of preoperation versus postoperative timepoints. Logistic regression analysis was performed to explore the factors that impaired Hyodo scores. Statistical tests were performed using GraphPad Prism 9.5.1 (Graph Pad Software, Boston, MA, USA), and logistic regression analysis was performed using the R-powered data tool Exploratory v6.12.5 (Exploratory Inc., Mill Valley, CA). Statistical significance was established at p < 0.05.
Ethical statement
Every participant in this study gave their informed consent for inclusion. The research adhered to the principles of the Declaration of Helsinki, and the protocol received approval from the institutional review board (Tokai University, 08-R98).
Results
Patient characteristics
This study included 73 patients (59 males and 14 females) with 79 lesions and a median age of 71 years. The median BMI was 20.845 kg/m^2^.
There were nine primary lesions in the supraglottis (four in the epiglottis, five in the arytenoid), 38 in the hypopharynx (25 in the piriform sinus, nine in the posterior wall, two post-cricoid, two in the piriform sinus to posterior wall), and 32 in the oropharynx (19 in the tonsils (p16-positive in 14), three in the base of the tongue (all p16-negative), six in the superior wall, one in the lateral wall, three in the posterior wall). Forty-nine lesions were T1, 30 lesions were T2, and six patients had multiple lesions. Fourteen patients had positive cervical lymph nodes and 16 patients underwent neck dissection. There were 35 patients with a history of esophageal cancer (23 with extended resection, 13 with endoscopic resection, five with irradiation), and 20 with a history of head and neck cancer (two with extended resection, four with neck dissection, 12 with transoral resection, six with irradiation). Only two patients underwent temporary tracheostomy to prevent surgically induced airway obstruction, and only two patients received postoperative irradiation. The patient characteristics are summarized in Table 2.
Outcome of swallowing function
The FOSS score at six months after surgery was grade 0 in 61 patients, grade 1 in 10 patients, and grade 2 in two patients. Most patients were able to consume food orally without any restrictions (Table 3).
There was no significant worsening of the mean Hyodo score in all subjects. The mean sub-scores also showed no significant difference compared to the preoperative sub-scores (Table 4). However, 23 patients exhibited impaired postoperative Hyodo score. Logistic regression analysis was performed on these 23 impaired patients to estimate predictors using age, BMI, primary site, T classification, neck dissection, history of head and neck cancer, history of radiation therapy to the head and neck, and history of esophageal cancer as predictor variables. Age ≥65 years was a significant predictor (p=0.026, Table 5).
Table 5: Logistic regression analysis to predict Hyodo score impairment.Statistical significance was established at p < 0.05.
In the time series, the Hyodo score of the impaired patient group significantly worsened at three and six months postoperatively (p=0.0002 and p=0.008, respectively; Table 6). Sub-scores also showed worsening at three and six months postoperatively for the glottal closure reflex induced by touching the epiglottis or arytenoid with the endoscope (p=0.0015, p=0.0374) and at three months postoperatively for the extent of pharyngeal clearance after blue-dyed water was swallowed (p=0.0196). No significant differences were found in other parameters such as the salivary pooling degree at the vallecula and piriform sinuses and the location of the bolus at the swallowing reflex initiation assessed by “white-out” timing.
Table 6: Score detail of Hyodo score and sub-score of impaired patients.The Kruskal-Wallis test was used to compare the mean rank of each time point. Dunn’s test was employed for multiple comparisons of preoperation versus postoperative timepoints. Statistical significance was established at p < 0.05.SE; Standard error
Outcome of QOL
Changes in EORTC QLQ C30 Functional Scale scores are shown in Figure 1. In the EORTC QLQ C30 Functional Scale, a higher score is interpreted as a better QOL. The Kruskal-Wallis test showed significant improvement in emotional score (p=0.016), which were significantly better at three months (p=0.0144) and 12 months (p=0.0348) after surgery compared to preoperation. No significant differences were observed among the other parameters.
Score trend of EORTC QLQ C30 Functional scales.Multiple comparisons of preoperation versus postoperative time points, Statistical significance was established at p < 0.05 (Asterisk).
Changes in EORTC QLQ C30 Symptom Scale scores are shown in Figure 2. In contrast to the functional scales, the lower the score on the symptom scales, the higher the QOL. The Kruskal-Wallis test showed no significant differences for any of the symptom scale parameters based on the measurement time points.
Score trend of EORTC QLQ C30 symptom scales.Multiple comparisons of preoperation versus postoperative time points, Statistical significance was established at p < 0.05.
Changes in EORTC QLQ H&N35 scores are shown in Figure 3. As with the EORTC QLQ C30 Symptom Scales, the smaller score indicates a higher QOL for H&N35. The Kruskal-Wallis test showed no significant differences for any of its respective parameters based on the measurement time points. No significant deterioration in QOL was identified after TOVS in either questionnaire method.
Score trend of EORTC QLQ H&N35.Multiple comparisons of preoperation versus postoperative time points, Statistical significance was established at p < 0.05.
Discussion
The mean QOL scores showed no significant differences before and after TOVS. In addition, the FOSS at six months after surgery showed that the overall level of oral intake was maintained, suggesting that TOVS is useful in maintaining swallowing function.
Neither the total Hyodo score, nor its sub-scores worsened overall, but by examining only exacerbation cases, we found exacerbation factors. In previous reports, predictors of dysphagia included ECOG PS, age ≥80 years, low BMI, and a history of head and neck irradiation [24-26]. We selected age, BMI, history of head and neck cancer, and history of head and neck irradiation as predictors for multivariate analysis. The age cut-off was 65 years, which is the World Health Organization (WHO) standard for elderly adults, and the BMI cut-off was 18.5 kg/m^2^, which is also the WHO standard for underweight. In addition, because of ADLH2 gene polymorphisms, esophageal squamous cell carcinoma is an important overlapping cancer of the head and neck region in Japan [8]; therefore, a history of esophageal cancer was added as a predictive factor. Neck dissection was also considered because surgical manipulation of the neck might affect swallowing function. The ECOG PS was not considered as all patients had an ECOG PS of 0. Consequently, age ≥65 years was the only predictor of a worsening Hyodo score.
The trend of the Hyodo score of impaired patients suggests that the score deterioration peaks at three and six months postoperatively, especially the glottal closure reflex induced by touching the epiglottis or arytenoid with the endoscope and the extent of pharyngeal clearance after blue-dyed water is swallowed. The trend is similar to other TORS reports on postoperative swallowing that have shown improvement over time [16]. Fujiwara et al. showed that the postoperative FOSS was worse in patients with aspiration on preoperative videofluoroscopy [24]. Although this study did not include cases of obvious aspiration on preoperative FEES, postoperative dysphagia due to decreased laryngeal perception and poor pharyngeal clearance should be considered in elderly patients.
One report showed improvement in endoscopic swallowing scores in elderly patients with dysphagia after laryngeal elevation training such as the swallowing forehead exercise and the chin push-pull maneuver without highly loaded head lifting [27]. Therefore, the introduction of perioperative rehabilitation may contribute to the maintenance or early recovery of swallowing function after transoral resection. Further studies are warranted.
There are reports of good QOL after microscopic mucosal resection [28], good voice and swallowing function after ELPS [13], and good QOL after transoral laser microsurgery for hypopharyngeal cancer [29]. Half of the patients in this study also had hypopharyngeal cancer, and despite differences in conventional surgical and evaluation methods, transoral resection for early stage pharyngolaryngeal cancer may contribute to the maintenance of QOL.
Some reports on transoral resection and QOL after TORS have been published, mostly in patients with oropharyngeal cancer. The ORATOR study reported worse QOL in the TORS + neck dissection group than in the radiation group [18]. However, some studies have suggested that transoral resection maintains the patient’s QOL [15,16]. In the ORATOR study, >70% of patients received postoperative radiotherapy after TORS. In the other studies, TORS alone or postoperative irradiation was used in less than half of all cases. The present study was conducted in a group of patients where only a few received postoperative irradiation, and our results show that QOL was maintained. Postoperative irradiation has a significant impact on QOL; therefore, the key to maintaining QOL is selecting patients who do not require postoperative irradiation. A detailed preoperative study of resectability is required to ensure successful transoral resection with a preferable QOL.
This study had several limitations. Although this was a prospective study, it was conducted at a single institution. This was not a comparison with other treatments, and a selection bias exists. The study also had many missing statistical values and was not a complete study of repeat cases. The Hyodo Score is simple, and widely used in Japanese clinical practice. The Japanese version is easily available and, therefore used in this study instead of the other validated FEES scales such as the penetration-aspiration scale [30], it should be noted that the Hyodo score is an unconventional evaluation method. Furthermore, many of this population have previous history of esophageal cancer and other head and neck cancers. They may be distinct from other populations; therefore, the study results may not be generalizable. However, quite favorable swallowing function and QOL are still given at the tumor sites.
Conclusions
TOVS generally preserves good swallowing function. However, there have been cases of deterioration of swallowing function peaking at three to six months postoperatively. Particular attention should be paid to the decline in swallowing function due to laryngeal imperception and poor pharyngeal clearance, especially in the elderly over 65 years of age.
QOL after TOVS is well maintained in the group of patients with no postoperative irradiation. Careful selection of patients whose treatment can be completed with transoral resection alone will help maintain QOL.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer N Engl J Med Forastiere AA Goepfert H Maor M 2091209834920031464563610.1056/NEJ Moa 031317 · doi ↗ · pubmed ↗
- 2Factors associated with severe late toxicity after concurrent chemoradiation for locally advanced head and neck cancer: an RTOG analysis J Clin Oncol Machtay M Moughan J Trotti A 358235892620081855987510.1200/JCO.2007.14.8841 PMC 4911537 · doi ↗ · pubmed ↗
- 3Long-term results of RTOG 91-11: a comparison of three nonsurgical treatment strategies to preserve the larynx in patients with locally advanced larynx cancer J Clin Oncol Forastiere AA Zhang Q Weber RS 8458523120132318299310.1200/JCO.2012.43.6097 PMC 3577950 · doi ↗ · pubmed ↗
- 4Transoral robotic surgery (TORS) for base of tongue neoplasms Laryngoscope O'Malley BW Jr Weinstein GS Snyder W Hockstein NG 1465147211620061688575510.1097/01.mlg.0000227184.90514.1a · doi ↗ · pubmed ↗
- 5Transoral robotic surgery: radical tonsillectomy Arch Otolaryngol Head Neck Surg Weinstein GS O'Malley BW Jr Snyder W Sherman E Quon H 1220122613320071808696310.1001/archotol.133.12.1220 · doi ↗ · pubmed ↗
- 6Human papillomavirus and rising oropharyngeal cancer incidence in the United States J Clin Oncol Chaturvedi AK Engels EA Pfeiffer RM 429443012920112196950310.1200/JCO.2011.36.4596 PMC 3221528 · doi ↗ · pubmed ↗
- 7Increase in primary surgical treatment of T 1 and T 2 oropharyngeal squamous cell carcinoma and rates of adverse pathologic features: National Cancer Data Base Cancer Cracchiolo JR Baxi SS Morris LG Ganly I Patel SG Cohen MA Roman BR 1523153212220162697005010.1002/cncr.29938 PMC 4860079 · doi ↗ · pubmed ↗
- 8Risk of superficial squamous cell carcinoma developing in the head and neck region in patients with esophageal squamous cell carcinoma Laryngoscope Katada C Muto M Nakayama M 1291129612220122267453210.1002/lary.23249 · doi ↗ · pubmed ↗