Stunted girl: A heartbreaking case report of underdiagnosed and untreated posterior ankyloglossia
Robertus Arian Datusanantyo, Simplicia Maria Anggrahini, Arif Tri Prasetyo

TL;DR
A case report shows how untreated posterior tongue-tie in a child led to stunted growth and developmental issues, which could have been prevented with early diagnosis and surgery.
Contribution
Highlights the underdiagnosed and severe impact of posterior ankyloglossia on child development and the role of plastic surgeons in addressing it.
Findings
Posterior ankyloglossia can cause stunting, speech disorders, and swallowing difficulties in children.
Surgical frenotomy improved tongue mobility and may prevent developmental delays.
Posterior ankyloglossia is rare, hard to diagnose, and often overlooked as a cause of growth issues.
Abstract
Plastic surgeons can help to eliminate stunting by surgically treating children born with congenital craniofacial anomalies such as tongue-tie, or ankyloglossia. Releasing ankyloglossia can help to support breastfeeding and the later development of orofacial anatomy and physiology. Failure to do so can lead to growth and development difficulties in children. We report a heartbreaking case of a stunted 8 year-old female with underdiagnosed and untreated ankyloglossia. The patient was consulted with a short stature, speech disorder, and swallowing disorder. History taking and physical examination led to a diagnosis of type 4 (posterior) ankyloglossia. The Hazelbaker Assessment Tool for Lingual Frenulum Function mandated a frenotomy. Under general anesthesia, frenotomy was performed surgically, and significant tongue mobility was gained. This case alerted both surgeon and pediatrician…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
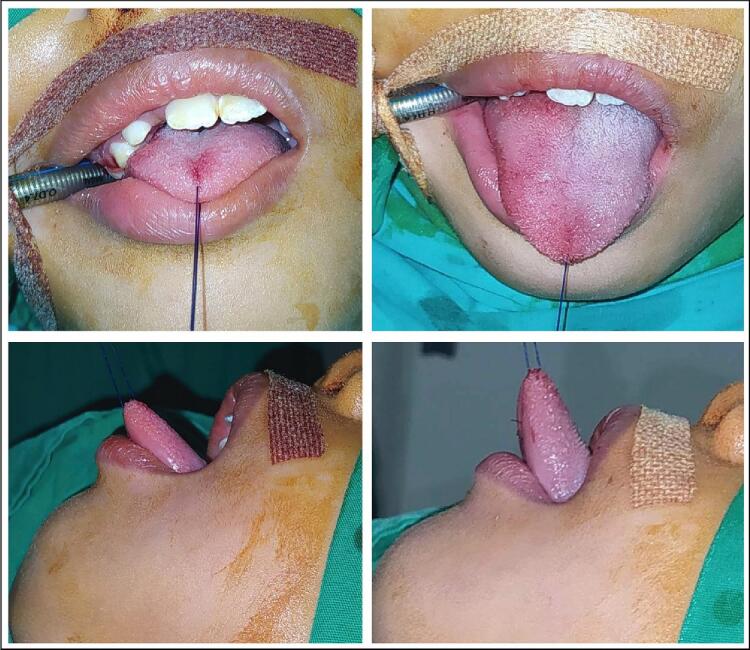 Figure 1
Figure 1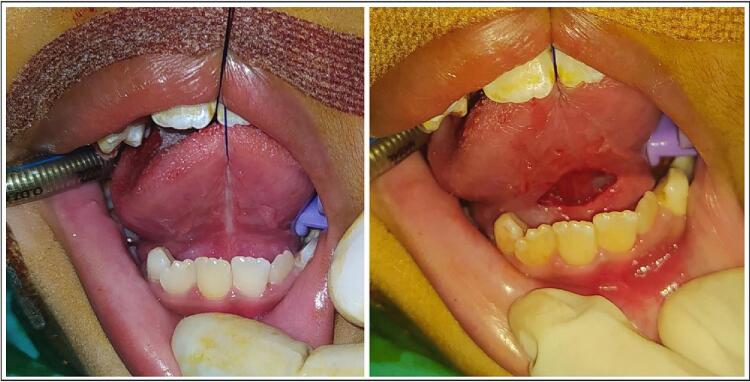 Figure 2
Figure 2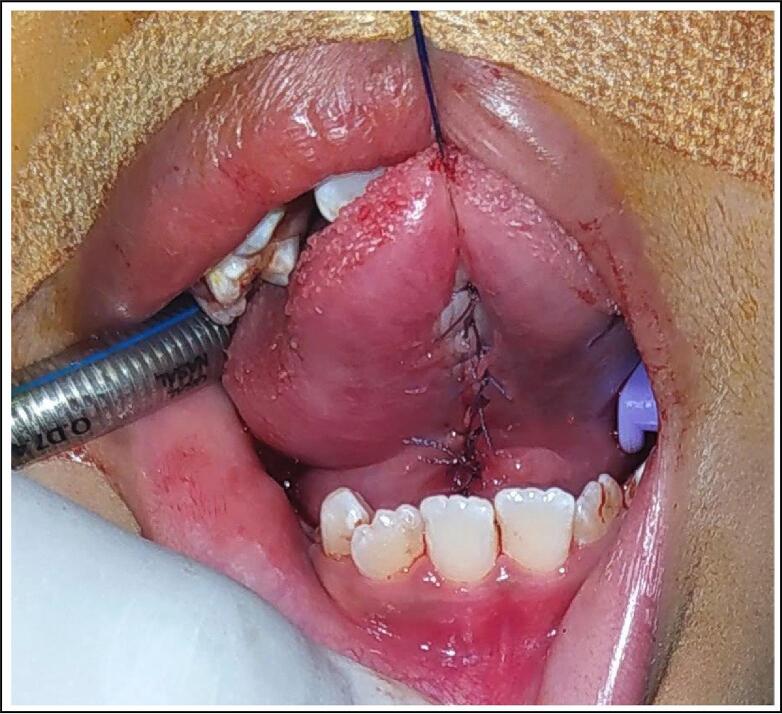 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral and Craniofacial Lesions · Genetic Syndromes and Imprinting · Head and Neck Anomalies
Introduction
1
Indonesia, particularly in the Lesser Sunda Islands, is still burdened with stunted children [1]. While poor linear growth or stunting (less than −2 of height-for-age Z score) [2] should be defined in the first one thousand days of age, stunted children beyond this age are seen in daily practice. Stunted children result from the complex interaction of multiple factors, both individually and at the household and community levels [[1], [2], [3]]. These factors are not necessarily pathological and may be related to household size, education level, maternal health status, and antenatal care.
However, children with poor nutritional intake may end up stunted. Swallowing difficulty or oropharyngeal dysphagia (OPD), prevents infants and children from optimal growth and development due to poor nutritional intake. The oral stage of OPD can be caused by tongue-tie, or ankyloglossia [4]. Ankyloglossia is a short lingual frenulum that limits tongue mobility, thus impairing tongue function, including swallowing [5].
Plastic surgeons are commonly consulted for ankyloglossia, especially when it is difficult to diagnose and treat. Different classifications and treatments of ankyloglossia are available but not widely accepted [6]. However, ankyloglossia is commonly classified based on free tongue length or elasticity of the frenulum, and the decision to surgical intervention is based on function and appearance [5]. Several researches support releasing ankyloglossia to improve breastfeeding, and failure to do so may lead to maldevelopment of orofacial musculatures [7].
We report a case of stunted girl whose ankyloglossia was underdiagnosed and was not treated properly. This case is particularly unique because the late diagnosis and treatment have led the patient to a stunted growth and underdeveloped physical and social skill. The patient was referred to our hospital, a general referral hospital with subspecialty and surgical service. This case is reported in line with the SCARE criteria [8].
Presentation of case
2
A little girl was referred to the pediatric and plastic surgery outpatient clinic with a chief complaint of speech disorder, drooling, and swallowing disorder. The patient was 8 years and 3 months old, with short stature (116 cm; −2 SD = 116.3 cm) and a weight of 18 kg (−2 SD = 19.1 kg). This made the patient slightly overweight, based on a body mass index of 20.1 (+2 SD = 20.8). The patient was born at 2400 g and had completed vaccination schedule as per the Indonesian health authorities' program.
Previously, the patient has been taken by the parent to visit several health care facilities to seek assessment regarding the difficulty in swallowing and speech. The patient has never been diagnosed with ankyloglossia, and some physical therapy was programmed but the parent didn't comply to all advice and treatment due to some social and domestic difficulties.
The patient spoke very little but maintained eye contact and used hand and facial gestures to communicate. She was cooperative during all physical examinations. Physical examination confirmed the inelasticity of the lingual frenulum, which attached from the posterior tip to below the alveolar ridge. The tip of the tongue could not extend beyond her lower lip (Fig. 1). When lifted, the tip of her tongue remained at the alveolar ridge. When asked to drink or eat, the patient showed difficulty in swallowing and excess water and saliva drooled from the corners of her mouth.Fig. 1. Pre- (left) and post- (right) operative photograph, notice the extension of tongue mobility.Fig. 1
The Hazelbaker Assessment Tool for Lingual Frenulum Function (HATLFF) appearance score was 7 and functional score was 10, indicating that frenotomy was necessary. The diagnosis of type 4 or posterior ankyloglossia was made, and frenotomy was performed under general anesthesia (Fig. 1).
Under general anesthesia, a horizontal incision was made in the mucosa to identify the thick fibrous band underneath (Fig. 2). Using both blunt and sharp dissection, the anterior tongue was released and improved mobility was gained. After hemostasis, the diamond-shaped mucosal defect was closed in a horizontal-to-vertical frenuloplasty fashion using absorbable sutures (Fig. 3).Fig. 2. Lingual frenulum in posterior ankyloglossia: short, thick, fibrous cord-like, obscured by mucosal curtain.Fig. 2. Fig. 3Horizontal-to-vertical frenuloplasty with absorbable suture.Fig. 3
Tongue mobility was improved, and the patient was transferred to a rehabilitation specialist to improve swallowing and speech. The patient returned to daily routine as a student of school for children with special needs. The parents observed no significant changes during the patient's routine physical and learning activity. During follow-up visits, we learned that the parents had failed to comply with the therapy schedule. Therefore, little to no functional improvement was observed on speech and swallowing post-operatively.
Discussion
3
Childhood stunting is the best indicator of inequalities that affect overall child well-being [9]. While stunting, by definition, is diagnosed in the first one thousand day of life, poor environmental conditions may falter children's growth beyond this milestone. The patient presented in this case was stunted. However, this condition was unlikely the result of environmental and social conditions. The child parents are both educated and have steady career. They live in urban area with plenty of access to healthcare. Thus, individual pathological condition is more likely to be responsible.
It is obvious during history and physical examination that the patient had been in continuous OPD due to ankyloglossia. This event led a series of consequences that resulted in her short stature and poor ability to perform daily task for a child her age. Segal and colleagues reported that ankyloglossia is associated with difficulties in breastfeeding, especially difficulty latching, nipple pain, and eventually risk of breastfeeding cessation [10]. A prevalence of ankyloglossia has been reported to be 5 %, but this may vary depending on the tools used in the assessment [11].
Ankyloglossia is also associated to speech disorder and malocclusion. A review by Suter and Bornstein described various mechanical limitation of the tongue in adults due to ankyloglossia, including difficulty in articulating specific consonants [6]. Ankyloglossia, although evidence is limited, may also influence the growth and development of the stomatognathic system and lead to malocclusion [6,7].
The simplest classification was proposed by Kotlow who measured tongue mobility using a dental instrument [12]. This method classifies ankyloglossia into clinically acceptable tongue mobility and four other class of ankyloglossia (Table 1). Walker and colleagues associated Kotlow's classification to breastfeeding difficulties and clearly suggested that maternal experience in breastfeeding should be an indicator of breastfeeding difficulty, as tongue mobility is associated with nipple pain [13].Table 1. Ankyloglossia according to Kotlow [12].Table 1. ClassRange of free tongueAcceptableNormal range of >16 mmClass IMild ankyloglossia, 12–16 mmClass IIModerate ankyloglossia, 8–11 mmClass IIISevere ankyloglossia, 3–7 mmClass IVComplete ankyloglossia, <3 mm
Coryllos and colleagues proposed another classification of ankyloglossia based on how close to the tip of the tongue the leading edge of the frenulum is attached [14]. This classification divides ankyloglossia into four types (Table 2). Ankyloglossia types 3 and 4 are called the posterior ankyloglossia and their uncharacteristic appearance may make them difficult to recognize during physical examination.Table 2. Types of ankyloglossia according to Coryllos and colleagues [14].Table 2. TypeFrenulum attachmentType 1Frenulum attached to tip of the tongue and anterior to alveolar ridge in the lower lip sulcusType 2Frenulum attached 2–4 mm posterior to the tip of the tongue and just behind the alveolar ridgeType 3Frenulum attached to the mid-tongue and the middle of floor mouth, usually tighter and less elasticType 4Frenulum is against the back of the tongue, thick, shiny, and very inelastic
While it was unfortunate for the patient to be underdiagnosed, posterior ankyloglossia itself is commonly missed when using attachment-only score [15]. In posterior ankyloglossia, the lingual frenulum is not prominent in inspection, but was short, thick or fibrous cord-like when examined using grooved director or manual palpation [16]. Chu and Bloom dramatically described it as “short, thick, fibrous cord posterior to the ventral tongue mucosa, obscured by mucosal curtain (Fig. 2)” [17].
The HATLFF is not a tool to diagnose ankyloglossia (Table 3). Instead, it quantifies functional and appearance items, and provides a recommendation for whether a frenotomy is necessary [18]. We perform this assessment on the patient and it showed impaired function and the appearance score was below 8. Both scores indicated that a frenotomy to be performed.Table 3. Hazelbaker assessment tool for lingual frenulum function [18].Table 3210. Appearance itemsAppearance of tongue when liftedRound or squareSlight cleft in tip apparentHeart-shapedElasticity of frenulumVery elastic (excellent)Moderately elasticLittle or no elasticityLength of lingual frenulum when tongue lifted>1 cm or embedded in tongue1 cm<1 cmAttachment of lingual frenulum to tonguePosterior to tipAt tipNotched tipAttachment of lingual frenulum to inferior alveolar ridgeAttached to floor of mouth or well below ridgeAttached just below ridgeAttached at ridge Function itemsLateralizationCompleteBody of tongue but not tongue tipNoneLift of tongueTip to mid-mouthOnly edges to mid-mouthTip stays at alveolar ridge or rises to mid-mouth only with jaw closureExtension of tongueTip over lower lipTip over lower gum onlyNeither of above or anterior to mid-tongue humpsSpread of anterior tongueCompleteModerate or partialLittle or noneCuppingEntire edge, firm cupSide edges only, moderate cupPoor or no cupPeristalsisComplete, anterior to posterior (originates at tip)Partial: originating posterior to tipNone or reverse peristalsisSnapbackNonePeriodicFrequent or with each suck14: Perfect score, regardless of appearance.11: Acceptable if appearance score >10.<11: Impaired function, frenotomy is considered if management fails. Frenotomy is necessary if appearance score is <8.
Significant gain was seen immediately after the frenotomy (Fig. 1). However, functional improvement was observed post-operatively. The parents were satisfied with the tongue mobility. Although the parents were informed and a transfer plan to a rehabilitation specialist was discussed, we were unable to observe any functional improvement after one year of follow up. The parent didn't comply with the rehabilitation schedule and the patient refused to physical treatment several times.
Unfortunately, the strength of this case is that we confirmed the collective failure that has resulted in a significant loss of this patient's potential as a daughter, child, and future community member. This is not only the devastating consequences of underdiagnosed and untreated posterior ankyloglossia, but also the collective failure to meet this patient's basic needs. While anterior ankyloglossia is easier to diagnose and accounts for 94 % of ankyloglossia [16], the minority posterior ankyloglossia is more challenging to diagnose. However, the patient had always had difficulty swallowing and later developed speech disorders. Both of these problems should have alerted the parents and healthcare professionals. Surgeons, in particular, should participate by considering posterior ankyloglossia when performing oral examination.
However, the limitation of this report is that despite anatomical gain in tongue mobility after the surgery, we failed to document significant functional improvement, especially in swallowing and speech. The parent gave written consent to this report and a clearance was granted by the hospital administrator to report and publish the case.
Conclusion
4
The absence of other social and environmental factors confirms that posterior (type 4) ankyloglossia was the single most responsible factor in this patient's growth and development disorder. This case implied that in clinical practice, surgeons and pediatricians should collaborate to ensure timely diagnosis and treatment of posterior ankyloglossia. Posterior ankyloglossia is not only rare and difficult to diagnose, but also leads to compromised growth. Timely diagnosis and treatment could have prevented such poor growth and development.
Consent
Written informed consent was obtained from the patient's parents for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
Approval for this case report was granted by the Prof. Dr. W. Z. Johannes General Hospital Director under an approval letter number: 445/2197/RSUD3.1.
Funding
This research did not receive any specific funding.
Author contribution
Robertus Arian Datusanantyo: Conceptualization; Data curation; Formal analysis; Methodology; Validation/Interpretation; Writing - original draft; and Writing - review & editing.
Simplicia Maria Anggrahini: Conceptualization; Data curation; Formal analysis; Methodology; Validation/Interpretation; Writing - original draft; and Writing - review & editing.
Arif Tri Prasetyo: Conceptualization; Data curation; Formal analysis; Methodology; Validation/Interpretation; Writing - original draft; and Writing - review & editing.
Guarantor
Robertus Arian Datusanantyo.
Simplicia Maria Anggrahini.
Arif Tri Prasetyo.
Research registration number
This study does not require registration.
Conflict of interest statement
The authors declare no conflicts of interest related to this study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wicaksono F.Harsanti T.Determinants of stunted children in Indonesia: a multilevelanalysis at the individual, household, and community levels Kesmas 15120204853
- 2Titaley C.R.Ariawan I.Hapsari D.Muasyaroh A.Dibley M.J.Determinants of the stunting of children under two years old in Indonesia: a multilevel analysis of the 2013 Indonesia basic health survey Nutrients 115May 1 201910.3390/nu 11051106 PMC 656719831109058 · doi ↗ · pubmed ↗
- 3Anastasia H.Hadju V.Hartono R.Manjilala 3S.Sirajuddin Salam A.Determinants of stunting in children under five years old in South Sulawesi and West Sulawesi Province: 2013 and 2018 Indonesian Basic Health Survey P Lo S One 185 May May 1 202310.1371/journal.pone.0281962 PMC 1017453137167300 · doi ↗ · pubmed ↗
- 4Moulton K.Seikel J.Loftin J.Devine N.Examining the effects of ankyloglossia on swallowing function International Journal of Orofacial Myology [Internet].441Nov 1 2018521 Available from:https://ijom.iaom.com/journal/vol 44/iss 1/1
- 5Brzęcka D.Garbacz M.Mical M.Zych B.Lewandowski B.Diagnosis, classification and management of ankyloglossia including its influence on breastfeeding Developmental Period Medicint.XXIII 12019798510.34763/devperiodmed.20192301.7985 PMC 852234130954985 · doi ↗ · pubmed ↗
- 6Suter V.G.A.Bornstein M.M.Ankyloglossia: facts and myths in diagnosis and treatment J. Periodontol.808Aug 2009120412191965602010.1902/jop.2009.090086 · doi ↗ · pubmed ↗
- 7Pompéia L.E.Ilinsky R.S.Feijóortolani C.L.Faltin K.Ankyloglossia and its influence on growth and development of the stomatognathic system Rev. Paul. Pediatr.352Apr 1 20172162212897733710.1590/1984-0462/;2017;35;2;00016 PMC 5496731 · doi ↗ · pubmed ↗
- 8Sohrabi C.Mathew G.Maria N.Kerwan A.Franchi T.Agha R.A.The SCARE 2023 guideline: updating consensus Surgical C Ase R Eport (SCARE) guidelines Int. J. Surg.1095 May 1 2023113611403701395310.1097/JS 9.0000000000000373 PMC 10389401 · doi ↗ · pubmed ↗