Reversible Cerebral Vasoconstriction Syndrome Mimicking Eclampsia
Chalothorn Wannaphut, Yoshito Nishimura, Weiming Du, Chutawat Kookanok, Travis Watai, Christina Chong

TL;DR
A pregnant woman initially thought to have eclampsia was later diagnosed with a rare condition called reversible cerebral vasoconstriction syndrome.
Contribution
The case highlights the diagnostic challenge of distinguishing RCVS from eclampsia and the potential role of calcium channel blockers in treatment.
Findings
The patient's symptoms and CTA findings led to a diagnosis of RCVS, not eclampsia.
Treatment with levetiracetam, magnesium, and nimodipine resulted in favorable neurological outcomes.
The case underscores the need to consider RCVS in the differential diagnosis of postpartum neurological symptoms.
Abstract
This report describes the case of an 18-year-old Micronesian pregnant woman at 32 weeks gestation, initially presumed to have eclampsia but later diagnosed with reversible cerebral vasoconstriction syndrome (RCVS). She presented with seizures, altered mental status, nystagmus, lower extremity weakness, and absent reflexes. An extensive workup ruled out infectious and autoimmune causes, but a computed tomography angiogram (CTA) revealed severe cerebral vasoconstriction. Treatment included levetiracetam, intravenous magnesium, and nimodipine. The case highlights the challenge of differentiating RCVS from eclampsia in the postpartum period, emphasizing the importance of considering alternative diagnoses and brain CTA when RCVS is suspected, with calcium channel blockers potentially contributing to favorable neurological outcomes.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
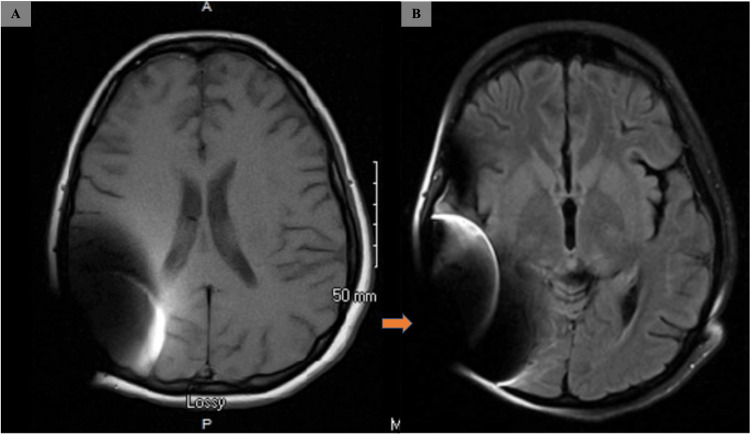 Figure 1
Figure 1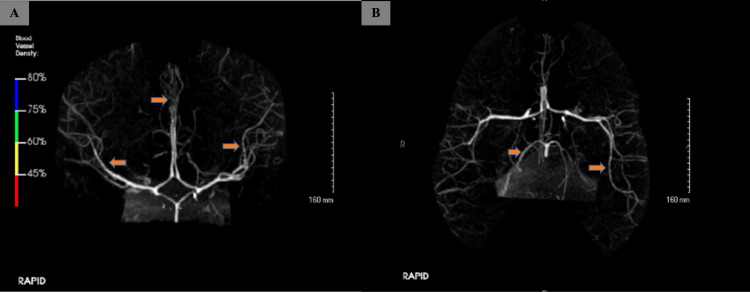 Figure 2
Figure 2| Complete blood count | Result | Reference range |
| WBC (103 /uL) | 7.2 | 3.8-10.84 |
| Hb (g/dl) | 10.1 | 11.2-15.7 |
| Hct (%) | 30.6 | 34.1-44.9 |
| Plt (103 /uL) | 261 | 151-424 |
| Biochemical findings | ||
| Na (mEq/L) | 137 | 133-145 |
| K (mEq/L) | 3.6 | 3.3-5.1 |
| Cl (mEq/L) | 98 | 95-108 |
| Mg (mEq/L) | 1.7 | 1.6-2.6 |
| Ca (mEq/L) | 8.5 | 8.3-10.5 |
| Glucose (mg/dL) | 80 | 70-99 |
| BUN (mg/dL) | 12 | 6.0-23 |
| S.Cr (mg/dL) | 0.7 | 0.6-1.4 |
| TP (g/dL) | 6.5 | 6.4-8.3 |
| Alb (g/dL) | 3.5 | 3.5-5.2 |
| AST (IU/L) | 20 | <40 |
| ALT (IU/L) | 19 | <42 |
| ALP (IU/L) | 120 | 35-129 |
| T.Bil (mg/dL) | 0.5 | <1.2 |
| LDH (IU/L) | 238 | 135-250 |
| Autoimmune workup findings | ||
| ANA | <40 | <40 |
| Anti-dsDNA | <1 | <4 |
| Anti-MOG-IgG | Negative | Negative |
| NMO antibody | Negative | Negative |
| AntiGQ1B | Negative | Negative |
| Cerebrospinal fluid analysis | Result | Reference range |
| Color | Colorless | Colorless |
| Appearance | Clear | Clear |
| RBC | 0 | 0 |
| WBC | 1 | <5 |
| Neutrophils (%) | 0 | 0 |
| Lymphocytes (%) | 100 | <5 |
| Monocytes (%) | 0 | 0 |
| Eosinophils (%) | 0 | 0 |
| Basophils (%) | 0 | 0 |
| Protein (mg/dl) | 62 | 15-45 |
| Sugar (mg/dl) | 60 | >60% of plasma value |
| Oligoclonal bands | Negative | Negative |
| Myelin basic protein | Negative | Negative |
| CSF meningitis/encephalitis panel | ||
|
| Not detected | |
| Haemophilus Influenzae | Not detected | |
| Listeria mononocytogenes | Not detected | |
| Neisseria | Not detected | |
| Streptococcus agalactiae | Not detected | |
| Streptococcus pneumoniae | Not detected | |
| Cytomegalovirus | Not detected | |
| Enterovirus | Not detected | |
| Herpetic simplex virus type 1 | Not detected | |
| Herpetic simplex virus type 2 | Not detected | |
| Human herpes virus 6 | Not detected | |
| Human parechovirus | Not detected | |
| Varicella | Not detected | |
| Cryptococcus | Not detected | |
|
| Negative | |
| VDRL | Non-reactive | |
| Gram stain | Negative | |
| CSF encephalopathy/paraneoplastic panel | ||
| AMPA-R Ab | Negative | |
| Amphiphysin | Negative | |
| AGNA-1 | Negative | |
| ANNA-1 | Negative | |
| ANNA-2 | Negative | |
| ANNA-3 | Negative | |
| CASPR2-IgG | Negative | |
| CRMP-5 | Negative | |
| DPPX AB IFA | Negative | |
| GABA-B-R Ab | Negative | |
| GAD65 Ab nmol/L | Negative | |
| IgLON5 IFA | Negative | |
| LGI1-IgG | Negative | |
| mGLuR1 Ab | Negative | |
| NMDAR Ab | Negative | |
| PCCA-1 | Negative | |
| PCCA-Tr | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological Complications and Syndromes · Moyamoya disease diagnosis and treatment · Pregnancy and preeclampsia studies
Introduction
Eclampsia is a serious pregnancy complication known for causing seizures, which can be life-threatening. However, seizures occurring beyond 48 hours postpartum are less likely to be triggered by eclampsia, necessitating investigations for alternative causes. Reversible cerebral vasoconstriction syndrome (RCVS) in postpartum women, also known as Call-Fleming syndrome, is a rare condition that was first documented in 1988 and is characterized by transient constriction of cerebral blood vessels [1,2]. While the hallmark manifestation is typically a sudden-onset headache, RCVS can also present with a spectrum of neurological symptoms, including confusion, focal neurologic deficit, photophobia, phonophobia, and epileptic seizures. In postpartum women, RCVS tends to manifest within the first three months following childbirth [2,3]. This temporal association underscores the importance of considering RCVS in the differential diagnosis of postpartum patients presenting with abnormal neurological symptoms. The present case describes diagnostic and therapeutic challenges in an 18-year-old pregnant woman with eclampsia who developed abnormal neurological symptoms postpartum and was ultimately diagnosed with RCVS.
Case presentation
An 18-year-old G1P0 Micronesian woman at 32 weeks of pregnancy, with a history of bilateral hearing loss treated with cochlear implants, presented with altered mental status, bilateral lower extremity weakness, and absent reflexes following an episode of eclampsia that necessitated emergent primary low transverse cesarean section (PLTCS). Eleven days earlier, she was admitted for sepsis secondary to pyelonephritis, treated with ceftriaxone, and discharged with oral cephalexin. Four days before the medicine consultation, she had a tonic-clonic seizure requiring PLTCS for non-reassuring fetal status. Post the operation, she was admitted to the intensive care unit and downgraded two days later, but she remained confused and had another seizure 48 hours postpartum. Medicine and neurology consultations were obtained, and levetiracetam and magnesium drip were initiated.
Upon examination, she was oriented to time, place, and person but was inattentive and easily distracted. Vital signs were unremarkable except for blood pressure of 155/119 mmHg. The patient appeared lethargic with a flat affect, and neurological examination revealed positive gaze-evoked nystagmus, 5/5 strength in bilateral upper extremities, 3/5 in bilateral lower extremities, intact light-touch sensations, positive cerebellar signs, and areflexia in patellar and Achilles reflexes. Plantar were flexor and there was no clonus.
Prior to admission, the patient was not taking any medications, supplements, or illicit drugs. The results of the main laboratory testing are summarized in Table 1. Lumbar puncture revealed WBC 1 cu/mm, red blood cell 0 cu/mm, protein 62 mg/dL, glucose 41 mg/dL, and no viral or bacterial organism was identified. It was negative for antinuclear antibody, venereal disease research laboratory (VDRL), oligoclonal bands, myelin basic protein, and autoimmune encephalitis panel (Table 2).
Initially, Miller-Fischer syndrome was a main differential diagnosis; however, it could not explain the patient's altered mental status and recurrent seizures. Additionally, a 16-hour EEG showed nonspecific mild diffuse disturbance of cerebral function. Brain MRI was normal except for artifact due to her cochlear implant (Figure 1), but computed tomography angiogram (CTA) of the brain showed diffuse severe narrowing of the anterior and posterior circulation, which led to the diagnosis of RCVS (Figure 2).
Brain MRI of the patientA: No acute intracranial abnormalities observed on MRI of the brain without contrast; B: Right cerebellum markedly limited secondary to artifact from a cochlear implant (orange arrow)
CTA of the brainA: Mild to moderate diffuse narrowing of the ACAs and MCAs (orange arrows); B: Mild to moderate diffuse narrowing of MCAs and PCAs (orange arrows)CTA: Computed tomography angiography, ACAs: Anterior cerebral arteries, MCAs: Middle cerebral arteries, PCAs: Posterior cerebral arteries
Given the persistent encephalopathy due to RCVS, the patient was transferred to the neuroscience ICU (NSICU) for close monitoring of her symptoms and intensive medical therapy, including anti-seizure medications and nimodipine as a vasodilatory agent. Fortunately, serial CTA brain showed improving vasospasm, and daily transcranial Doppler revealed improving velocity. The patient was discharged on hospital day 29 with two weeks of nimodipine and levetiracetam 500 mg twice daily.
Discussion
The present report describes a challenging case of RCVS in the setting of a patient with known eclampsia. While clinicians tend to associate peripartum seizures with eclampsia as in this case, persistent seizures beyond 48 hours postpartum require an alternate diagnosis such as intracerebral hemorrhage, subarachnoid hemorrhage, encephalitis, encephalopathy, CNS vasculitis, epilepsy, or postpartum angiopathy [2]. In particular, RCVS is a rare yet reversible cause of peripartum seizures with encephalopathy. It manifests as reversible cerebral vasoconstriction, typically occurring within the initial three weeks postpartum [3]. Reversible cerebral vasoconstriction syndrome has been linked to various factors, including pregnancy, migraines, vasoconstrictive drugs, aneurysms, and neurosurgical procedures. Diagnostic imaging with CTA reveals a widespread reduction in the caliber of cerebral vessels and their branches.
The optimal treatment for RCVS remains uncertain, but existing studies recommend calcium channel blockers such as verapamil or nimodipine. Additionally, intravenous magnesium therapy is suggested for its vasodilatory effects [4-6]. The study by Marsh et al. indicates a potential superiority of verapamil among calcium channel blockers [6]; however, the effectiveness of nimodipine in addressing vasoconstriction has been observed in McIlroy et al.'s study [7]. Further randomized controlled trials are required to establish a definitive treatment approach. Previous studies report a good prognosis with self-limited symptoms and complete recovery within three months [8]. Recurring episodes of RCVS in future pregnancies are uncommon [9].
Early diagnosis and treatment are essential to reduce the risk of stroke associated with RCVS [10]. However, as in the present case, symptoms of RCVS are nonspecific, and patients tend to be prematurely diagnosed and treated as a more common syndrome, such as eclampsia. It is essential to thoroughly assess the situation and consider other possible explanations to avoid premature closure.
Conclusions
Reversible cerebral vasoconstriction syndrome encompasses a spectrum of disorders marked by the transient constriction of cerebral arteries, leading to multifocal narrowing. Despite the generally favorable clinical prognosis associated with RCVS, it is crucial to acknowledge the potential for severe complications, including major strokes that can result in significant disability or even mortality in some cases. Recognition of RCVS as a potential diagnosis becomes particularly imperative in patients presenting with prolonged altered mental status, and its consideration is paramount in specific clinical scenarios, such as pregnancy. In addition, the optimal treatment for RCVS is unclear but existing studies recommended calcium channel blockers such as nimodipine or verapamil. The multifaceted nature of RCVS underscores the importance of a comprehensive medical history, including the identification of potential triggers or predisposing factors, for a more accurate and timely diagnosis. Clinicians should remain vigilant to the manifestations of RCVS, as early intervention and management can significantly impact the overall clinical outcome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Reversible cerebral segmental vasoconstriction Stroke Call GK Fleming MC Sealfon S Levine H Kistler JP Fisher CM 11591170191988304607310.1161/01.str.19.9.1159 · doi ↗ · pubmed ↗
- 2Eclampsia in the 21st century Am J Obstet Gynecol Bartal MF Sibai BM 0226202210.1016/j.ajog.2020.09.03732980358 · doi ↗ · pubmed ↗
- 3Reversible cerebral vasoconstriction syndrome, Part 1: epidemiology, pathogenesis, and clinical course AJNR Am J Neuroradiol Miller TR Shivashankar R Mossa-Basha M Gandhi D 139213993620152559320310.3174/ajnr.A 4214 PMC 7964694 · doi ↗ · pubmed ↗
- 4Reversible segmental cerebral vasoconstriction (Call-Fleming syndrome): are calcium channel inhibitors a potential treatment option?Cephalalgia Nowak DA Rodiek SO Henneken S Zinner J Schreiner R Fuchs HH Topka H 2182222320031266219010.1046/j.1468-2982.2003.00507.x · doi ↗ · pubmed ↗
- 5Magnesium for treatment of reversible cerebral vasoconstriction syndrome: case series Neurohospitalist Mijalski C Dakay K Miller-Patterson C Saad A Silver B Khan M 111113620162736629410.1177/1941874415613834 PMC 4906552 · doi ↗ · pubmed ↗
- 6The need for a rational approach to vasoconstrictive syndromes: transcranial Doppler and calcium channel blockade in reversible cerebral vasoconstriction syndrome Case Rep Neurol Marsh EB Ziai WC Llinas RH 161171820162772178010.1159/000447626 PMC 5043170 · doi ↗ · pubmed ↗
- 7Severe postpartum headache and hypertension caused by reversible cerebral vasoconstriction syndrome: a case report A A Case Rep Mc Ilroy E Sethuraman R Woograsingh R Nelson-Piercy C Gilbert-Kawai E 289291920172869703010.1213/XAA.0000000000000595 · doi ↗ · pubmed ↗
- 8Reversible cerebral vasoconstriction syndrome: literature review Egypt J Neurol Psychiatr Neurosurg Ribas MZ PaticciéGF de Medeiros SD de Oliveira Veras A Noleto FM Dos Santos JC 55920233664743610.1186/s 41983-023-00607-9PMC 9833030 · doi ↗ · pubmed ↗