Cutaneous Eruption in a Crohn’s Disease Patient Under Tumor Necrosis Alpha Inhibitor Treatment: A Rare Case of Syphilis
Georgia Bellou, Eirini Zaharopoulou, Anastasios Giannoukos, Olga Kosmopoulou, Maria Tzouvala

TL;DR
A Crohn’s disease patient on anti-TNFα therapy developed a skin rash, which was diagnosed as syphilis and successfully treated with penicillin.
Contribution
This case highlights the rare but important possibility of syphilis as a cutaneous manifestation in immunosuppressed patients.
Findings
A 28-year-old Crohn’s patient on infliximab developed a painless, non-pruritic exanthema.
Diagnosis of early secondary syphilis was confirmed via fluorescent treponemal antibodies-absorbed test.
Treatment with benzathine penicillin G resolved the skin eruption within weeks.
Abstract
Reaching a diagnosis of a cutaneous eruption in a Crohn’s disease (CD) patient treated with anti-tumor necrosis factor alpha (anti-TNFα) can be challenging. Differential diagnosis must include extra-intestinal manifestations of CD, adverse reactions to the therapy itself as well as infectious diseases with cutaneous manifestations. We report the case of a 28-year-old man on infliximab for Crohn’s colitis, who presented with painless, non-pruritic genital and body exanthema. After a thorough evaluation, early secondary syphilis was confirmed with a fluorescent treponemal antibodies-absorbed test. Intramuscular (IM) benzathine penicillin G 2.4 million units in a single dose was administered and clinical manifestations resolved completely within a couple of weeks.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1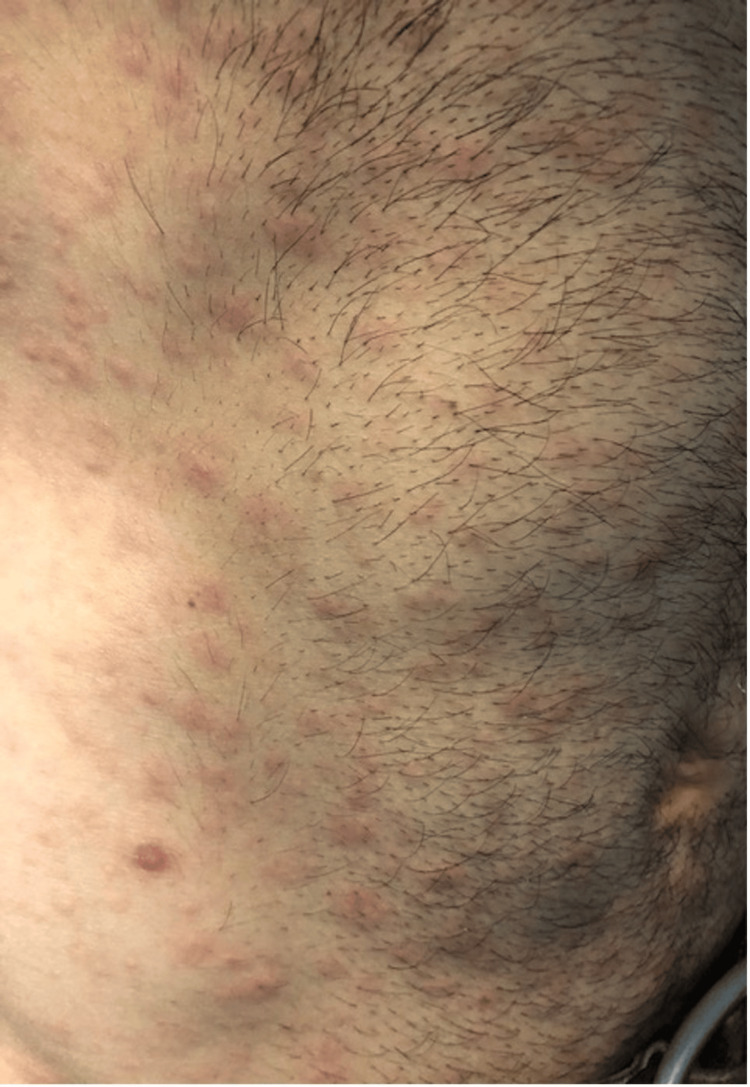 Figure 2
Figure 2 Figure 3
Figure 3| Reference | Disease | Drug | Neurological manifestation | Treatment |
| Bettenworth et al. [ | Ulcerative colitis | Infliximab | No | Penicillin 10 million IV IU 14 days |
| Kase et al. [ | Psoriasis vulgaris | Infliximab | Yes (emotional lability and excitability) | Penicillin 24 million IV IU 10 days and ceftriaxone 28 days |
| Asahina et al. [ | Rheumatoid arthritis | Initially, adalimumab but changed to infliximab on suspicion of paradoxical reaction | No | Amoxicillin (no dose or treatment duration specified) |
| Bories-Haffner et al. [ | Ankylosing spondylitis | Infliximab | No | Penicillin 24 million of IV IU 15 days |
| Assikar et al. [ | Ankylosing spondylitis | Etanercept | Yes (hypomanic episode) | IV penicillin 14 days (no dose specified) |
| Iglesias Plaza et al. [ | Ankylosing spondylitis | Golimumab | No | Penicillin G 2.4 million IM total 3 doses and due to positive pharyngeal PCR for Neisseria gonorrhoeae ceftriaxone 250 mg IV and azithromycin 1 g PO |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune and Inflammatory Disorders · Immunodeficiency and Autoimmune Disorders · Syphilis Diagnosis and Treatment
Introduction
Crohn’s disease is an idiopathic, chronic inflammatory bowel disease (IBD) affecting the gastrointestinal tract. It is also characterized by extra-intestinal manifestations (EIMs) which may include the skin in 2-34% of IBD patients. The most common skin EIMs associated with CD are pyoderma gangrenosum and erythema nodosum. Other rare cutaneous EIMs include metastatic CD affecting the perineum, feet, legs, penis and vulva, leukocytoclastic vasculitis, Sweet syndrome, cutaneous polyarteritis nodosa, and epidermolysis bullosa acquisita. Furthermore, increased occurrence of psoriasis has been described among patients with CD, although it is not considered an EIM of the disease itself. Treatment for CD includes immunosuppressive medications, such as biologics and novel small molecules. A commonly used biologic agent is an anti-tumor necrosis factor alpha (anti-TNFα) monoclonal antibody which is associated with cutaneous adverse events such as psoriasiform rash or eczema and opportunistic dermatologic infections as well such as pityriasis rosea, dermatophytes, herpes, and Staphylococcus aureus [1-3].
Thus, a CD patient treated with anti-TNFα agents who presents with a cutaneous eruption requires a thorough clinical approach and syphilis should always be included in the differential diagnosis as it is considered “The Great Imitator.”
Syphilis is an infectious disease caused by the spirochete Treponema pallidum and is primarily transmitted sexually by contact with the infectious lesions, as well as vertically from mother to fetus and via blood and blood products. The disease is characterized by three stages manifesting with clinical symptoms, primary, secondary, and tertiary syphilis, with latent asymptomatic stages in between. Primary syphilis typically manifests with a painless and highly contagious ulcer at the site of insertion, usually occurring on the external genitalia, perineum, and anus, and known as chancre. Secondary syphilis appears six to 12 weeks after the primary infection when the spirochete spreads systemically through the bloodstream. Clinical manifestations of the secondary stage may include non-specific symptoms such as fever, fatigue, generalized lymphadenopathy, as well as syphilitic dermatitis and condylomata lata which are characteristic of this stage. If left untreated, tertiary syphilis may develop and involvement of the cardiovascular system, central nervous system, and other internal organs occurs [4,5]. It has been reported that in patients on immunosuppressive therapy, syphilis may present with an accelerated clinical course and develop rapidly tertiary syphilis [6,7].
Case presentation
We herein present a case of a 28-year-old male patient with CD treated with anti-TNFα immunosuppressive therapy (Infliximab 5 mg/kg every eight weeks), for six years, in clinical and endoscopic remission, presented with a sudden cutaneous eruption of salmon-colored non-pruritic lesions. The rash appeared in the beginning on his external genitalia (Figure 1) seven weeks after the last infliximab infusion and expanded on the trunk (Figure 2) upper and lower limbs, (Figure 3), including the palms and soles, and was accompanied by mild diffuse arthralgia and elevated inflammatory markers (WBC: 10.830, ESR: 73 mm/h, CRP: 92.5 mg/l {upper normal limit 3 mg/l}).
Salmon-colored lesions on external genitaliaImage credit: Georgia Bellou
Salmon-colored lesions on the trunkImage credit: Georgia Bellou
Salmon-colored lesions on the limbsImage credit: Georgia Bellou
Infliximab infusion was temporarily withheld. After the initial dermatologic consultation, we performed viral assays including antibodies for Epstein-Barr, Cytomegalovirus, Coxsackie, Echo, and HIV, as well as microbiological and immunological assays including antibodies for Toxoplasma, throat strep test for detection of streptococcal group A antigen, lupus anticoagulant, anti-cardiolipin antibodies and venereal disease research laboratory test for detection of Treponema pallidum antibodies which were all negative.
The type and the distribution of the rash, combined with the gradual clinical deterioration of the patient with fatigue and arthralgia raised again the suspicion of early secondary syphilis which was eventually confirmed with a fluorescent treponemal antibodies-absorbed test.
Following diagnosis, we thoroughly interviewed the patient, who could not recall a primary syphilitic chancre, but he admitted frequent unprotected sexual intercourse. Intramuscular (IM) benzathine penicillin G 2.4 million units in a single dose was administered and clinical manifestations resolved completely within a couple of weeks. Three weeks post-treatment, inflammatory markers returned to normal and infliximab infusion was resumed without relapse of the infection after an 18-month follow-up.
Discussion
A cutaneous eruption in a Crohn’s disease patient under anti-TNFα therapy can be challenging. Differential diagnosis must include extra-intestinal manifestations of Crohn’s disease, adverse reactions to the therapy itself, as well as infectious diseases with cutaneous manifestations. In such cases, medical history is of great importance, as well as the fact that this group of patients may exhibit an accelerated clinical course when infected due to immunosuppressive therapy.
Our patient presented with a generalized maculopapular rash, affecting the palms and soles, accompanied by non-specific symptoms, and elevated inflammatory markers, and manifested seven weeks after infliximab infusion. The patient was in clinical and endoscopic remission, thus disease exacerbation and EIMs associated with it were ruled out. The type and the distribution of the rash helped to narrow down the differential diagnosis and exclude other EIMs and drug-induced adverse reactions. Furthermore, patients treated with biologics are immunosuppressed, and thus the risk of infections is higher in such individuals. Despite the fact that non-treponemal tests were negative, the clinical picture raised high suspicion of early secondary syphilis which was eventually confirmed by fluorescent treponemal antibodies-absorbed test.
In our literature review using PubMed, we found only six cases of syphilis under anti-TNFα and they were mainly treated with intravenous penicillin even in the absence of neurologic symptoms (Table 1) [2,6-10].
However, treatment guidelines for primary and secondary syphilis recommend benzathine penicillin G 2.4 million units intramuscularly in a single dose among the general population and persons with HIV infection. Treatment guidelines for immunosuppressed individuals or patients under biologics are not available. We administered our patient the recommended regimen, with excellent response and no relapse after long follow-up [11].
Conclusions
In conclusion, the clinical approach to a Crohn’s disease patient with cutaneous lesions under anti-TNFα treatment is complex. Acquisition of a thorough medical history is critical for reaching the correct diagnosis early, initiate appropriate treatment and avoid serious complications in immunocompromised patients. Diagnostic work-up should include infectious diseases, such as syphilis, when clinical course is suspicious. Hence, an interdisciplinary approach is fundamental. Treatment options for syphilis in patients on biologic therapy induce skepticism, since there are no specific guidelines for such cases, so far.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sleisenger and Fordtran's gastrointestinal and liver disease Philadelphia Elsevier 2020 https://www.us.elsevierhealth.com/sleisenger-and-fordtrans-gastrointestinal-and-liver-disease-2-volume-set-9780323609623.html
- 2Secondary syphilis occurring under anti-TN Falpha therapy Joint Bone Spine Bories-Haffner C Buche S Paccou J 3643657720102045280210.1016/j.jbspin.2010.02.023 · doi ↗ · pubmed ↗
- 3Review article: dermatological complications of immunosuppressive and anti-TNF therapy in inflammatory bowel disease Aliment Pharmacol Ther Moran GW Lim AW Bailey JL 100210243820132409946710.1111/apt.12491 · doi ↗ · pubmed ↗
- 4Syphilis 6 2023 Morris S 2023 https://www.msdmanuals.com/professional/infectious-diseases/sexually-transmitted-infections-stis/syphilis
- 5Fascinating molecular and immune escape mechanisms in the treatment of ST Is (syphilis, gonorrhea, chlamydia, and herpes simplex)Int J Mol Sci Scurtu LG Jinga V Simionescu O 23202210.3390/ijms 23073550 PMC 899880535408911 · doi ↗ · pubmed ↗
- 6Advanced-stage syphilis unmasking after immunomodulator therapy in a patient with ulcerative colitis Am J Gastroenterol Bettenworth D Floer M Krummenerl T Wehrmann W Schärer L Heidemann J 14414510720122221804010.1038/ajg.2011.330 · doi ↗ · pubmed ↗
- 7Rapidly developed neurosyphilis in a psoriasis patient under treatment with infliximab: a case report Acta Derm Venereol Kase K Ishii-Osai Y Sumikawa Y Yoneta A Himeno D Kakutani Y Yamashita T 3513529520152511139710.2340/00015555-1932 · doi ↗ · pubmed ↗
- 8Secondary syphilis following tumor necrosis factor-α inhibitor treatment for rheumatoid arthritis J Dermatol Asahina A Ishii N Tohma S 1992013920122146336410.1111/j.1346-8138.2011.01243.x · doi ↗ · pubmed ↗