Unmasking tuberculosis: Isolated hilar adenopathy in an asymptomatic immunocompetent adult
Aasir M. Suliman, Mushtaq Ahmad, Mustafa A. Al-Tikrity, Ibrahim Rashid

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
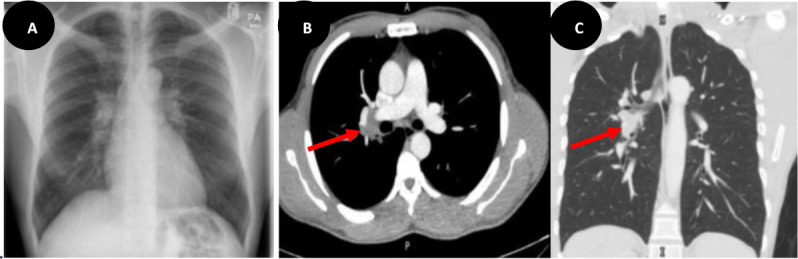 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Infectious Diseases and Tuberculosis · Diagnosis and treatment of tuberculosis
Background
Isolated mediastinal lymphadenopathy is a common manifestation of tuberculosis (TB) in children and adults with human immunodeficiency virus (HIV) infection. However, it is rare in immunocompetent adults without a parenchymal lung lesion, and presents a diagnostic problem due to the low diagnostic yield of sputum examination and the wide range of differential diagnoses.^1,2^
Case Presentation
A 36-year-old, previously healthy and asymptomatic male was found to have prominent hilar shadows during a routine chest X-ray (Figure 1A) conducted for immigration screening. Subsequent computed tomography (CT) chest imaging confirmed a single enlarged right hilar lymph node (Figure 1B and C) without additional parenchymal abnormalities. Sputum samples for acid-fast bacilli (AFB) smear, AFB polymerase chain reaction (PCR), and TB culture were all negative. Hilar tuberculous adenopathy was conclusively confirmed by endoscopic bronchial ultrasound (EBUS) with a positive fine needle aspiration (FNA) for AFB PCR. Notably, the serum HIV antigen/antibody test showed a non-reactive result. Consequently, the patient began a 6-month course of anti-tubercular treatment.
Conclusion
Isolated tuberculous mediastinal lymphadenopathy in immunocompetent adults is uncommon and may be underdiagnosed, given that patients are often asymptomatic until there is mass effect and compression of adjacent structures.^2^ The differential diagnosis of a mediastinal mass is broad and poses a common challenge in clinical practice. This case highlights the importance of considering TB as a potential etiology in adults with mediastinal lymphadenopathy without lung parenchymal involvement, even if the patient is asymptomatic or immunocompetent. Early recognition is crucial to initiate prompt treatment, avoid unnecessary invasive procedures, and achieve better outcomes.
Conflict of Interest
The authors declare that they have no known competing financial or personal interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Iyengar KB Kudru CU Nagiri SK Rao ACK Tuberculous mediastinal lymphadenopathy in an adult BMJ Case Reports 2014;2014:bcr 201320071810.1136/bcr-2013-200718 PMC 390232324419636 · doi ↗ · pubmed ↗
- 2Maguire S Chotirmall SH Parihar V Cormican L Ryan CO’Keane C Isolated anterior mediastinal tuberculosis in an immunocompetent patient BMC Pulmonary Medicine 2016;16:2410.1186/s 12890-016-0175-726842759 PMC 4739107 · doi ↗ · pubmed ↗