Pericardial decompression syndrome
Um I Rubab, Shaikh Nissar

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
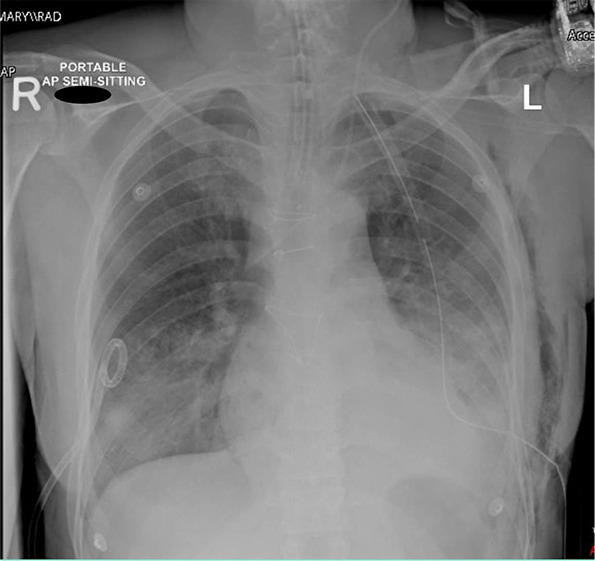 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLabor Law and Work Dynamics · Workplace Violence and Bullying · Criminal Justice and Penology
Background
The massive amount of pericardial fluid accumulation with or without cardiac tamponade needs drainage. Following the drainage procedure, there may be hemodynamic deterioration in the cardiac status of the patient, leading to transient left ventricular dysfunction and subsequent pulmonary edema. This phenomenon is called pericardial decompression syndrome (PDS).^1^ PDS is a potentially life-threatening complication associated with drainage of pericardial fluid either surgically or via image-guided drainage. It is often underreported, poorly understood, and often overlooked. It is an acute emergency, and intensivists, anesthetists, and surgeons should be aware of this rare clinical condition.
Case
Following open repair of the right subclavian artery pseudo aneurysm in a young patient, significant pericardial effusion occurred, necessitating surgical drainage that resulted in the removal of 1500 ml of transudate pericardial fluid. In the postoperative period, despite initial improvement and extubation, the patient experienced a decline, manifesting as acute pulmonary edema (Figure 1). As shown in Table 1, the patient was vitally unstable. This led to the need for reintubation and the initiation of vasopressor and diuretic therapy, ultimately diagnosed as PDS. Upon admission to the intensive care unit, the patient received supportive therapy and showed improvement within 48 hours. This progress enabled successful weaning of vasopressors and extubation of the trachea.
Conclusion
Patients who undergo either surgical or image-guided drainage for substantial pericardial effusion may experience the development of PDS. Early detection and management in the intensive care unit are crucial.
Conflict of Interest
Both authors have no conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.