Neoadjuvant nivolumab plus chemotherapy followed by resection for superior sulcus tumour with high PD‐L1 expression: A case report
Takahito Nakaya, Yoshimitsu Hirai, Hiroaki Akamatsu, Fumiyoshi Kojima, Hideto Iguchi, Aya Fusamoto, Yumi Yata, Takahiro Nagai, Daiki Kitahara, Toshiaki Takakura, Yoshiharu Nishimura, Nobuyuki Yamamoto

TL;DR
A 76-year-old man with a lung tumor near the shoulder had successful treatment using immunotherapy plus chemotherapy before surgery, leading to complete removal of the tumor.
Contribution
This case report presents a new treatment approach for superior sulcus tumors using neoadjuvant chemo-immunotherapy followed by minimally invasive surgery.
Findings
Neoadjuvant nivolumab plus chemotherapy led to a pathologic complete response in a superior sulcus tumor.
The tumor was successfully resected with minimal invasion through a modified thoracotomy.
No residual tumor cells were found in the resected specimen.
Abstract
The standard treatment for resectable non‐small cell lung cancer (NSCLC) located in the superior sulcus is neoadjuvant chemoradiotherapy followed by highly invasive resection. Based on the results of the CheckMate 816 trial, which showed a marked improvement in the efficacy of neoadjuvant chemo‐immunotherapy, we report a case of minimally invasive resection after neoadjuvant nivolumab plus chemotherapy for superior sulcus NSCLC, resulting in a pathologic complete response. The patient was a 76‐year‐old man with a 65‐mm right superior sulcus tumour diagnosed as squamous cell carcinoma with 95% PD‐L1. After two courses of neoadjuvant nivolumab plus chemotherapy, the tumour was completely resected through an 11‐cm right lateral thoracotomy with second rib resection and first rib preservation. No residual tumour cells were observed in the specimen, and the patient had a pathologic complete…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
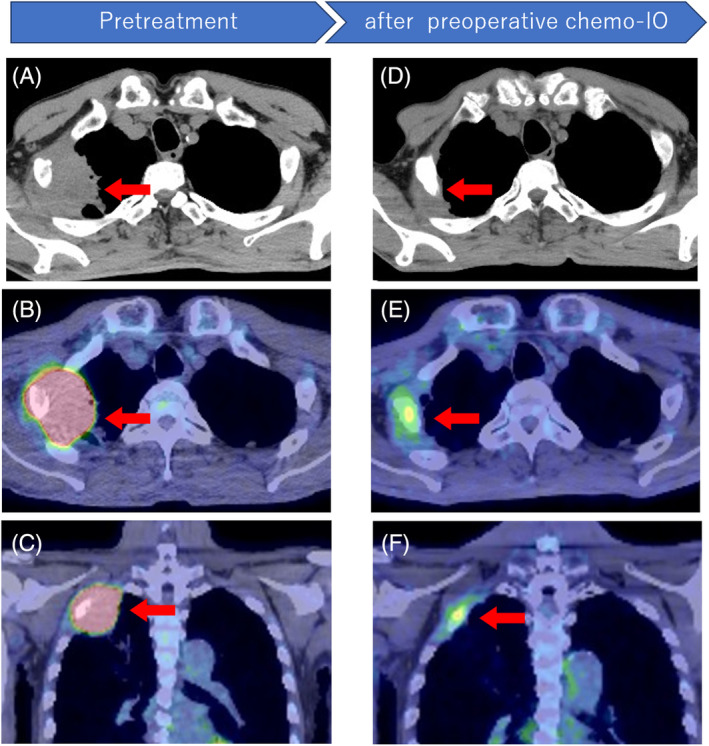 FIGURE 1
FIGURE 1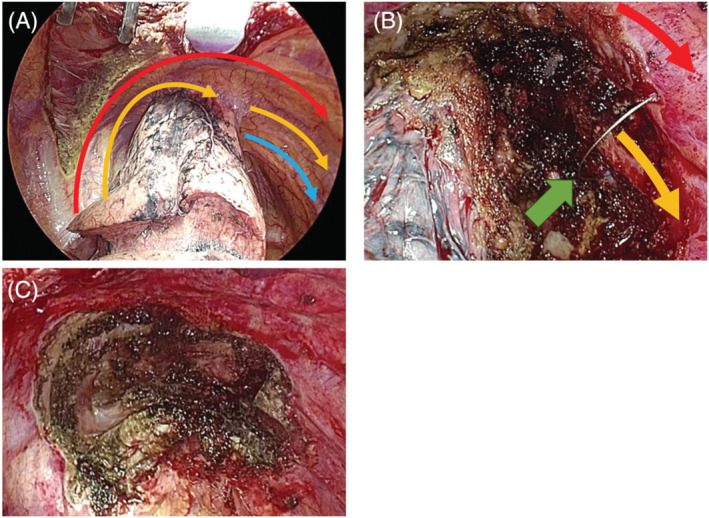 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Diagnosis and Treatment · Salivary Gland Tumors Diagnosis and Treatment · Lung Cancer Treatments and Mutations
INTRODUCTION
Neoadjuvant chemoradiotherapy, followed by resection, is recommended for patients with non‐small cell lung cancer (NSCLC) involving the chest wall located in the superior sulcus.1 However, the typical surgical procedure for superior sulcus tumour (SST) with dorsal superior rib resection is highly invasive. The CheckMate 816 trial revealed that neoadjuvant nivolumab plus chemotherapy is a new treatment strategy for resectable NSCLC,2 but its efficacy in SST is unclear. Here, we report a case of SST with high PD‐L1 expression in a patient who underwent complete resection via minimally invasive surgery after receiving neoadjuvant nivolumab plus chemotherapy.
CASE REPORT
A 76‐year‐old man with right‐sided chest pain was referred to our hospital. Computed tomography (CT) showed a 65‐mm tumour located in the apical pulmonary region, which invaded the chest wall and showed osteolytic changes in the second rib (Figure 1A). Positron emission tomography‐computed tomography (PET‐CT) revealed a high maximum standardized uptake of fluorodeoxyglucose (FDG) in the tumour and no other affected lymph nodes or organs on whole‐body imaging (Figure 1B,C). After transbronchial lung biopsy, the tumour was diagnosed as squamous cell carcinoma of the lung with PD‐L1 expression of 95% by immunohistochemistry (22c3, Dako). Neoadjuvant chemotherapy (carboplatin [AUC 6], paclitaxel [200 mg/m^2^], and nivolumab [200 mg/body]) was started and after two courses of treatment, the tumour size shrank from 65 mm to 21 mm (Figure 1D) and areduction of FDG uptake was observed reduction of maximum standardized FDG uptake was observed on PET‐CT (18.8–3.71, Figure 1E,F). Despite good local control, the patient's general condition deteriorated slightly. Therefore, we decided to perform a resection.
Computed tomography (CT) at first visit to our hospital in axial view (A), Positron emission tomography‐computed tomography (PET‐CT) at first visit to our hospital in axial (B) and coronal view (C), CT after neoadjuvant nivolumab and chemotherapy in axial view (D), PET‐CT after neoadjuvant chemo‐immunotherapy in axial (E) and coronal view (F).
The patient was placed in the left lateral position under general anaesthesia using a double‐lumen endotracheal tube. The surgical procedure was performed through an 11‐cm right lateral thoracotomy at the fourth intercostal space between the middle and posterior axillary lines. Because the lung adhesions were limited to tumour invasion, it was determined that resection of the first rib was not necessary and no additional open chest surgery was performed (Figure 2A). The second rib was resected dorsally using Riehl and Kellison forceps and ventrally using a line saw guided by an indwelling needle sheath (Figure 2B). The periostea of the first and third ribs were dissected in the extrapleural layer along with the resected second rib, and the portion of the chest wall invaded with tumour was resected from within the chest cavity. Subsequently, with the resected chest wall attached to the lung, a right upper lobectomy and mediastinal lymph node dissection were performed, and the tumour was removed en bloc (Figure 2C). The operative time was 316 min and blood loss was 165 mL. Postoperative pain meditation was as usual, effective and well pain control was obtained. The drainage tube was removed on the third postoperative day, and the patient was discharged on the eighth day without postoperative complications. Histopathological findings showed no residual tumour, and the patient was diagnosed with pathologic complete response (pCR; residual viable tumour: 0%). Surgical margins were negative. After three postoperative months, the patient is alive without postoperative complications, and remained in good general condition.
Intraoperative view. Arrows show the location of ribs. Blue arrow: first rib, yellow arrow: second rib, red arrow: third rib, green arrow: line saw.
DISCUSSION
Because local control is difficult with resection alone, neoadjuvant chemoradiotherapy followed by resection is the standard treatment for SST.1 Even if chemoradiotherapy causes substantial tumour shrinkage, it often provokes inflammation and fibrosis around the tumour, making resection difficult. Rusch et al. reported the results of neoadjuvant chemoradiotherapy in patients with SST in the Intergroup Trial 0160 study,3 with a pCR rate of 36%. In contrast, the CheckMate 816 trial showed a comparable pCR rate, even though this regimen did not include radiotherapy. The pCR rate of nivolumab plus chemotherapy was 44.7% in patients in whom PD‐L1 was expressed in more than 50% of the tumour.1
In this case, the tumour showed 32% radiological shrinkage, and more importantly, we successfully resected the tumour using a less invasive method. Because radiotherapy was omitted, estimating the extent of tumour invasion during surgery without adhesions or fibrosis caused by radiotherapy proved beneficial. Resection for SST with dorsal high‐rib resection usually requires a large skin incision and extensive muscle resection, such as high posterolateral thoracotomy,4 which results in postoperative pain and a limited range of motion of the upper extremities. In this case, we prepared with high posterolateral thoracotomy and minimally invasive approach. As expected, the excellent intraoperative visual field enabled second rib resection to be performed within the thoracic cavity using a minimally invasive approach, and pCR was achieved (residual viable tumour: 0%). Although observation of recurrence required long‐term follow‐up, the patient had no postoperative complications such as postoperative pain and a limited range of motion of the upper extremities. This treatment strategy may have resulted in a good postoperative course.
AUTHOR CONTRIBUTIONS
Takahito Nakaya: Conceptualization; writing‐original draft and visualization. Yoshimitsu Hirai: Supervision and writing‐original draft and review and editing and visualization. Hiroaki Akamatsu, Fumiyoshi Kojima, Hideto Iguchi, Aya Fusamoto, Yumi Yata, Takahiro Nagai, Daiki Kitahara, Toshiaki Takakura, Yoshiharu Nishimura, Nobuyuki Yamamoto: Project administration and writing‐review and editing.
CONFLICT OF INTEREST STATEMENT
Hiroaki Akamatsu, Honoraria; Amgen Inc, AstraZeneca K.K., Boehringer Ingelheim Japan Inc., Bristol‐Myers Squibb, Chugai Pharmaceutical Co. Ltd., Eli Lilly Japan K.K., MSD K.K., Nippon Kayaku. Co. Ltd., Novartis Pharma K.K., Ono Pharmaceutical Co. Ltd., Pfizer Inc, Takeda Pharmaceutical Co. Ltd. and Taiho Pharmaceutical Co. Ltd. Advisory role; Amgen Inc, and Janssen Pharmaceutical K.K., Sandoz. Research funding; Amgen Inc, Chugai Pharmaceutical Co. Ltd. and MSD K.K.. Nobuyuki Yamamoto, Honoraria; AbbVie Inc., Accuray Japan K.K., Amgen K.K., AstraZeneca K.K., Boehringer Ingelheim Japan Inc., Chugai Pharmaceutical Co. Ltd., Daiichi Sankyo Co., Ltd., Eli Lilly Japan K.K., Guardant Health Japan Corp., Janssen Pharmaceutical K.K., Merck Biopharma Co., Ltd., Miyarisan Pharmaceutical Co., Ltd., MSD K.K., Kyorin Pharmaceutical Co., Ltd., Novartis Pharma K.K., Ono Pharmaceutical Co. Ltd., Pfizer Inc, Takeda Pharmaceutical Co. Ltd. and Taiho Pharmaceutical Co. Ltd., Terumo Corp., Tsumura & Co.. Advisory role; Amgen K.K., AstraZeneca K.K., Chugai Pharmaceutical Co. Ltd., Eli Lilly Japan K.K., MSD K.K., Novartis Pharma K.K., Ono Pharmaceutical Co. Ltd. Research funding; AbbVie Inc., Amgen K.K., Asahi Kasei Corporation, AstraZeneca K.K., A2 Healthcare Corporation, Boehringer Ingelheim Japan Inc., Bristol‐Myers Squibb K.K., Chugai Pharmaceutical Co. Ltd., EPS Holdings, Inc., IQVIA Services Japan K.K., Janssen Pharmaceutical K.K., Mebix, Inc., MSD K.K., Novartis Pharma K.K., Ono Pharmaceutical Co. Ltd., Taiho Pharmaceutical Co. Ltd.. Data safety Monitoring Board: AstraZeneca K.K. All other authors declare no conflict of interest.
ETHICS STATEMENT
The authors declare that appropriate written informed consent was obtained for the publication of this manuscript and accompanying images.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Postmus PE , Kerr KM , Oudkerk M , Senan S , Waller DA , Vansteenkiste J , et al. Early and locally advanced non‐small‐cell lung cancer (NSCLC): ESMO clinical practice guidelines for diagnosis, treatment and follow‐up. Ann Oncol. 2017;28(4):iv 1–iv 21. 10.1093/annonc/mdx 222 28881918 · doi ↗ · pubmed ↗
- 2Forde PM , Spicer J , Lu S , Provencio M , Mitsudomi T , Awad MM , et al. Neoadjuvant Nivolumab plus chemotherapy in Resectable lung cancer. N Engl J Med. 2022;386:1973–1985. 10.1056/NEJ Moa 2202170 35403841 PMC 9844511 · doi ↗ · pubmed ↗
- 3Rusch VW , Giroux DJ , Kraut MJ , Crowley J , Hazuka M , Winton T , et al. Induction chemoradiation and surgical resection for superior sulcus non‐small‐cell lung carcinomas: long‐term results of southwest oncology group trial 9416 (intergroup trial 0160). J Clin Oncol. 2007;25:313–318. 10.1200/JCO.2006.08.2826 17235046 · doi ↗ · pubmed ↗
- 4Shaw RR , Paulson DL , Kee JL . Treatment of superior sulcus tumor by irradiation followed by resection. Ann Surg. 1961;154:29–40. 10.1097/00000658-196107000-00003 17859668 PMC 1465837 · doi ↗ · pubmed ↗