Unmasking May-Thurner Syndrome: A Case Report of Massive Deep Vein Thrombosis
Khalid A Alshehri, Adnan A Bahashwan, Abdulaziz Y Fakieha, Hatem E Alkhamisi, Mohammed M Albladi

TL;DR
This case report describes a rare cause of deep vein thrombosis in a woman with no risk factors, highlighting the importance of considering anatomical issues like May-Thurner syndrome.
Contribution
The paper presents a rare clinical case of May-Thurner syndrome causing deep vein thrombosis without traditional risk factors.
Findings
A 42-year-old woman with no medical history developed left leg symptoms due to massive deep vein thrombosis.
Imaging confirmed May-Thurner syndrome as the underlying cause of the thrombosis.
Treatment with anticoagulation, thrombolysis, and stent placement led to improvement and no recurrence.
Abstract
Deep venous thrombosis is a significant medical condition that results in life-threatening complications such as pulmonary embolism. Various factors can contribute to the formation of deep venous thrombosis, including prolonged immobility, surgery, and specific health conditions. May-Thurner syndrome is an underrecognized cause of deep venous thrombosis due to the compression of the left common iliac vein by the right common iliac artery. It poses diagnostic challenges due to its varied clinical presentations. This report discusses a 42-year-old female with no notable medical history who presented with acute onset of left leg swelling, pain, and discoloration. Despite the absence of common risk factors for deep venous thrombosis, investigations revealed a massive left-sided deep venous thrombosis. Additional imaging studies revealed the diagnosis of May-Thurner syndrome, manifesting as…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1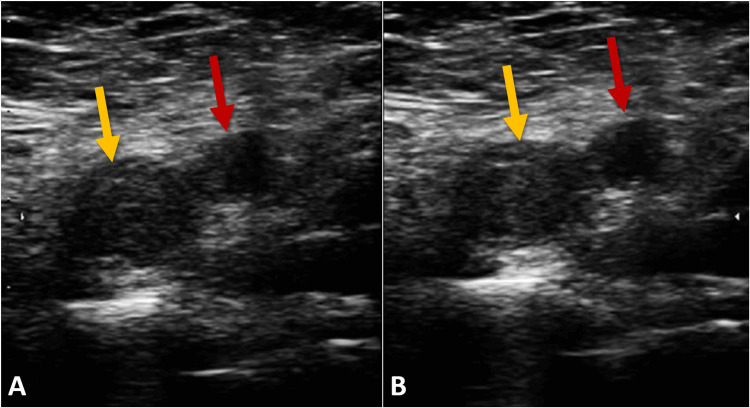 Figure 2
Figure 2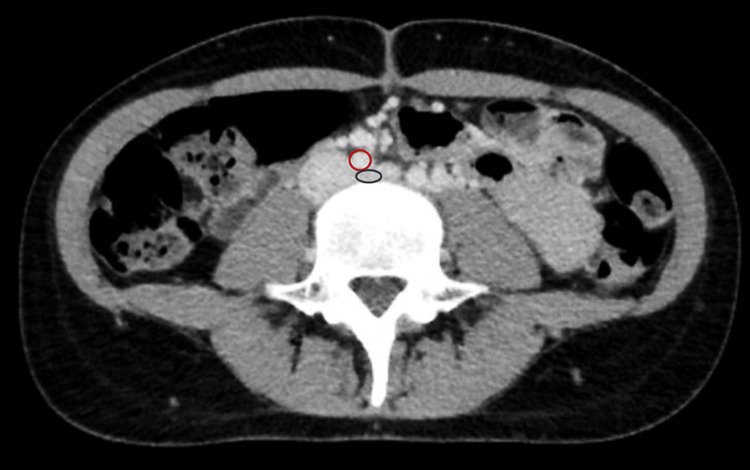 Figure 3
Figure 3| Laboratory Test | Units | Result | Reference Range |
| Hemoglobin | g/dL | 13.2 | 12.0 - 15.5 |
| White Blood Cell Count | x 109/L | 7.4 | 4.0 - 11.0 |
| Platelet Count | x 109/L | 250 | 150 - 400 |
| Prothrombin Time | seconds | 13 | 11 - 14 |
| International Normalized Ratio | ratio | 1.0 | 0.8 - 1.2 |
| Activated Partial Thromboplastin Time | seconds | 30 | 25 - 35 |
| Creatinine | mg/dL | 0.9 | 0.6 - 1.2 |
| Alanine Aminotransferase | U/L | 22 | 7 - 56 |
| Aspartate Aminotransferase | U/L | 24 | 8 - 48 |
| Total Bilirubin | mg/dL | 0.9 | 0.1 - 1.2 |
| Albumin | g/dL | 4.2 | 3.5 - 5.0 |
| Blood Urea Nitrogen | mg/dL | 14 | 6 - 20 |
| D-dimer | mg/L | 0.8 | 0 - 0.5 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Diagnosis and Treatment of Venous Diseases · Central Venous Catheters and Hemodialysis
Introduction
Deep vein thrombosis is a critical medical condition that can lead to life-threatening complications, such as pulmonary embolism, highlighting the importance of timely diagnosis and management [1]. The etiology of deep vein thrombosis is multifactorial, with risk factors including prolonged immobilization, surgery, malignancy, inherited thrombophilia, and hormonal therapy [2]. Despite its relatively common occurrence, certain cases of deep vein thrombosis arise from less common anatomical abnormalities, presenting a diagnostic challenge [1,2].
May-Thurner syndrome, also known as iliac vein compression syndrome, is one such underrecognized condition that predisposes individuals, especially young women, to left-sided deep vein thrombosis. This syndrome results from compression of the left common iliac vein by the overlying right common iliac artery, leading to chronic venous stasis and increased risk of thrombosis [3]. The clinical presentation of May-Thurner syndrome can vary widely, from asymptomatic to severe limb swelling and pain [3]. Given its nonspecific presentation and the potential for significant morbidity, awareness, and understanding of May-Thurner syndrome are crucial for healthcare providers [1,3]. This report describes a case of massive left-sided deep vein thrombosis where subsequent investigations revealed the underlying diagnosis of May-Thurner syndrome, highlighting the importance of considering anatomical variations in the differential diagnosis of unexplained deep vein thrombosis.
Case presentation
We present a case of a 42-year-old female patient with no significant past medical history, who came to the emergency department complaining of a three-day history of progressive swelling, pain, and a bluish discoloration of her left leg. The onset of symptoms was acute, with the patient noting that she awoke with mild discomfort that worsened significantly over the following days. She denied any recent travel, surgery, trauma, or history of thromboembolic events. The patient also reported no use of tobacco, alcohol, or illicit drugs and had no family history of clotting disorders.
Upon physical examination, her left leg was notably swollen, measuring 3 centimeters larger in circumference than the right leg at the level of the thigh. Pitting edema extended up to the mid-thigh, and the skin over the left leg appeared cyanotic and was warm to the touch (Figure 1). The patient’s vital signs were within normal limits, with a heart rate of 78 beats per minute, blood pressure of 125/80 mmHg, respiratory rate of 16 breaths per minute, and a temperature of 98.6℉. The remainder of the physical examination was unremarkable.
Comparative photograph of the patient's legsThis photograph presents a side-by-side comparison of the patient's legs, highlighting the left leg's pronounced swelling, discoloration, and apparent venous distension relative to the right leg. The left leg demonstrates significant clinical manifestations of deep vein thrombosis, including increased circumference, a bluish-purple skin discoloration indicative of cyanosis, and visible venous congestion.
Initial laboratory work-up showed a complete blood count with a hemoglobin level of 13.2 g/dL, a white blood cell count of 7.4 x 109/L, and a platelet count of 250 x 109/L. The coagulation profile revealed a prothrombin time of 13 seconds (international normalized ratio: 1.0) and an activated partial thromboplastin time of 30 seconds. The chemistry panel indicated normal kidney and liver function, with a creatinine level of 0.9 mg/dL and alanine aminotransferase of 22 U/L (Table 1).
Suspecting deep vein thrombosis, a Doppler ultrasound of the lower extremities was performed, revealing an extensive thrombus in the left common and external iliac veins, which was indicative of a left-sided massive deep vein thrombosis (Figure 2). The unusual extent and location of the thrombosis, especially in a patient lacking overt risk factors, prompted further investigation into an underlying etiology.
Color Doppler ultrasound of the femoral veinThis color Doppler ultrasound image showcases the femoral vein (yellow arrow) and the femoral artery (red arrow), highlighting their normal anatomical positions without compression (A). The inability of the femoral vein to collapse under applied compression (B) indicates a critical diagnostic sign of deep vein thrombosis.
A computed tomography venogram was subsequently performed, which showed significant compression of the left common iliac vein by the overlying right common iliac artery, along with an extensive thrombus extending from the left common iliac vein into the inferior vena cava (Figure 3). These findings were diagnostic of May-Thurner syndrome, an anatomical condition where the left common iliac vein is compressed by the right common iliac artery, leading to venous stasis and thrombosis.
Computed tomography venogram showing May-Thurner syndromeA computed tomography venogram clearly highlights the significant compression of the left common iliac vein (blue circle) by the overlying right common iliac artery (red circle), providing a vivid visualization of the anatomical anomaly characteristic of May-Thurner syndrome. This illustrates the cause of the patient's deep vein thrombosis.
Management commenced with the initiation of anticoagulation therapy using low molecular weight heparin, with a transition to oral anticoagulants planned. Considering the severity of the thrombosis and the anatomical challenge posed by May-Thurner syndrome, the patient underwent catheter-directed thrombolysis followed by stent placement in the left common iliac vein to relieve the venous compression and prevent recurrent thrombosis. The hospital course was marked by a minor complication of mild bleeding at the catheter insertion site, which was managed conservatively.
The patient demonstrated significant symptomatic improvement, with a reduction in limb swelling. Over a six-month follow-up period, she remained symptom-free, with no evidence of recurrent thrombosis or post-thrombotic syndrome, as monitored through regular anticoagulation checks, Doppler ultrasound examinations, and clinical evaluations.
Discussion
The complexities involved in diagnosing and managing May-Thurner syndrome, particularly in the context of a massive left-sided deep vein thrombosis, underscore a significant interplay between rare anatomical anomalies and prevalent vascular disorders. This case adds to the growing corpus of evidence emphasizing the need for a high degree of clinical suspicion for May-Thurner syndrome in patients presenting with unexplained lower extremity deep vein thrombosis, especially in the absence of traditional predisposing factors [2,4].
May-Thurner syndrome is characterized by the extrinsic compression of the left common iliac vein by the overlying right common iliac artery, predisposing individuals to venous stasis and thrombosis [1-3]. This phenomenon, initially described by May and Thurner in 1957, suggests that the chronic pulsation of the artery against the vein, coupled with compression against the lumbar vertebrae, leads to intimal hyperplasia and subsequent venous obstruction [3,4].
The differential diagnosis for deep vein thrombosis includes a variety of conditions such as cellulitis, lymphedema, and ruptured Baker's cyst [2-5]. However, in cases of left-sided deep vein thrombosis lacking apparent risk factors, the differential diagnosis narrows, emphasizing the relevance of May-Thurner syndrome. The clinical similarities between these conditions and May-Thurner syndrome-associated deep vein thrombosis often obscure the diagnostic pathway, underscoring the necessity for high clinical suspicion and the appropriate use of diagnostic imaging [4,5].
The diagnostic process in this case highlights the essential role of imaging in revealing the underlying cause of deep vein thrombosis. While Doppler ultrasound remains the first-line diagnostic tool for deep vein thrombosis, its limitations in visualizing the pelvic veins necessitate further imaging to identify May-Thurner syndrome [2-4]. Here, computed tomography venography was instrumental in confirming the presence of deep vein thrombosis and in identifying the anatomical compression indicative of May-Thurner syndrome.
Managing deep vein thrombosis induced by May-Thurner syndrome requires a nuanced approach that addresses both the immediate thrombotic event and the underlying venous compression [1,4]. This case illustrates an integrated management strategy encompassing anticoagulation, catheter-directed thrombolysis, and venous stenting. Literature suggests that while anticoagulation is crucial for preventing further thrombus formation, it does little to correct the underlying venous obstruction [2-4]. Catheter-directed thrombolysis and stenting not only address acute symptoms but also aim to prevent long-term complications by restoring venous flow [3,5].
Conclusions
In conclusion, this case not only sheds light on the diagnostic and therapeutic challenges associated with May-Thurner syndrome but also emphasizes the critical need for awareness of anatomical considerations in vascular medicine. By detailing the relationship between anatomical anomalies and thrombotic risk, this discussion contributes to a deeper understanding of May-Thurner syndrome and advocates for a more comprehensive and aggressive management strategy. Future research should aim to refine diagnostic criteria, improve management guidelines, and clarify the long-term outlook for patients with May-Thurner syndrome, thereby enhancing patient outcomes in this underrecognized population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1May-Thurner syndrome: history of understanding and need for defining population prevalence J Thromb Haemost Harbin MM Lutsey PL 5345421820203182170710.1111/jth.14707 · doi ↗ · pubmed ↗
- 2May-Thurner syndrome: a case report and a concise review Cureus Al Sinani A Al Saadi W Al Harthi S Al Hajriy M 013202110.7759/cureus.16256 PMC 834626334373817 · doi ↗ · pubmed ↗
- 3May-Thurner syndrome: a case report and review of the literature Case Rep Vasc Med Kalu S Shah P Natarajan A Nwankwo N Mustafa U Hussain N 740182201320132350966410.1155/2013/740182 PMC 3590570 · doi ↗ · pubmed ↗
- 4May-Thurner syndrome Cardiovasc Diagn Ther Poyyamoli S Mehta P Cherian M Anand RR Patil SB Kalva S Salazar G 110411111120213481596110.21037/cdt.2020.03.07PMC 8569277 · doi ↗ · pubmed ↗
- 5May-Thurner syndrome: an interesting presentation of recurrent, unprovoked deep vein thrombosis Cureus Phillips-Smith BA Jatana J Carter E Machani S Wickel DJ 015202310.7759/cureus.43491 PMC 1049966337719504 · doi ↗ · pubmed ↗