Point of Care Ultrasound Identification and Aspiration of a Neck Lymph Node
Andrew Moore, Ali Mrad, Leonard Riley, Sonia M Castillo

TL;DR
This paper describes a case where point-of-care ultrasound was used to diagnose and aspirate a neck lymph node in a patient with lung cancer.
Contribution
The novelty lies in using real-time ultrasound-guided fine needle aspiration for tissue diagnosis in this clinical context.
Findings
Real-time ultrasound-guided fine needle aspiration successfully diagnosed recurrent lung adenocarcinoma.
The method provided a minimally invasive and effective tissue diagnosis for staging lung cancer.
Ultrasound-guided aspiration of neck lymph nodes can be a viable diagnostic option.
Abstract
The tissue diagnosis and staging of all types of lung cancer is foundational for prognosis and establishing the optimal treatment plan. In order to appropriately stage lung cancer, the highest stage should be established using the 8th edition TNM criteria, where tumor size (T), nodal involvement (N), and metastasis (M) are all taken into account. Establishing a tissue diagnosis may involve the use of CT guided biopsy, navigational bronchoscopy, endobronchial biopsy, EBUS, percutaneous lymph node biopsy and/or excisional biopsy of supraclavicular nodes. It is recommended to proceed with the method that is considered least invasive and provides the highest staging. We present a case of recurrent lung adenocarcinoma diagnosed with real time ultrasound-guided fine needle aspiration of a neck lymph node.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1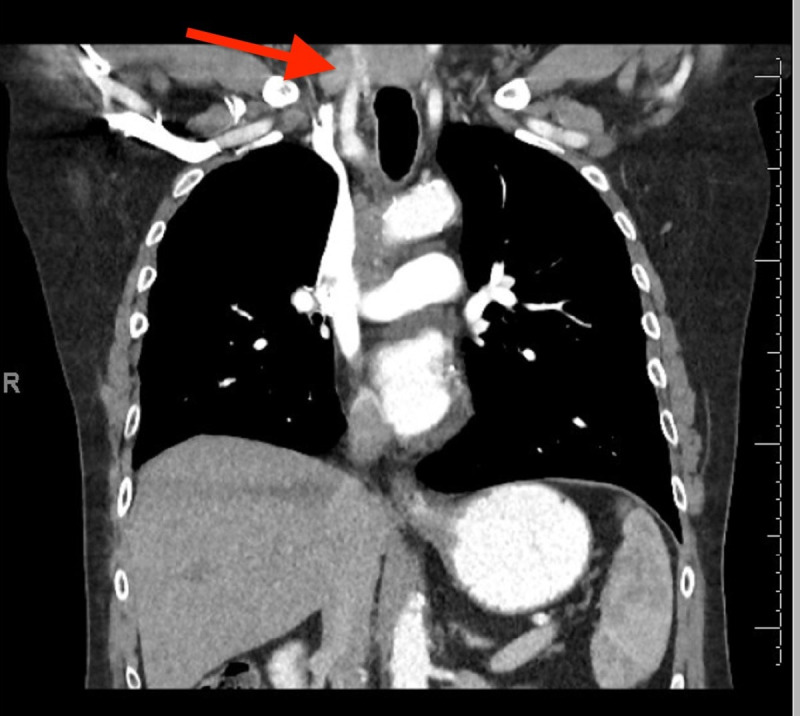 Figure 2
Figure 2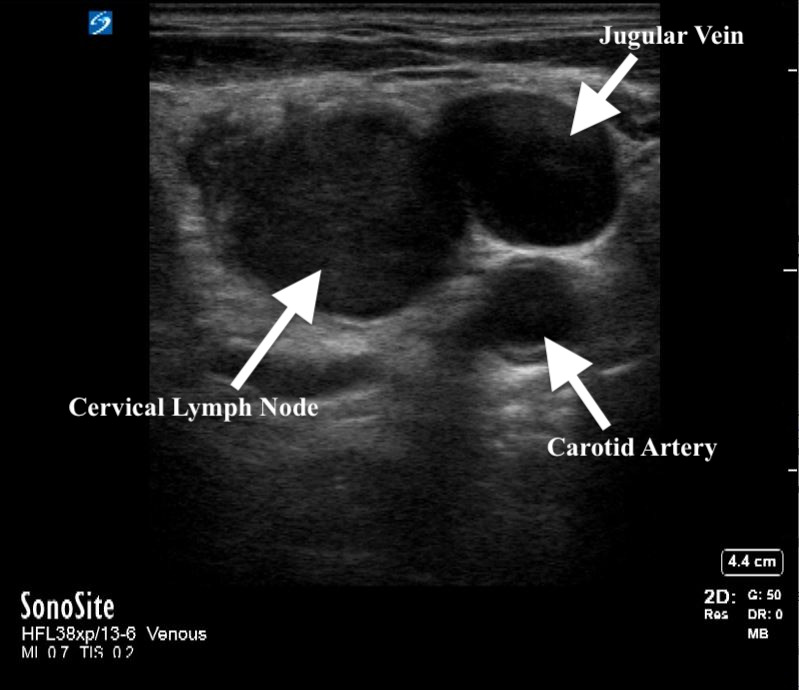 Figure 3
Figure 3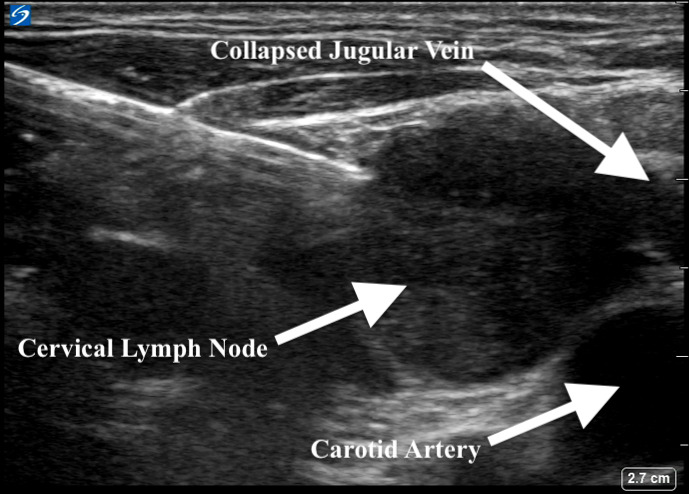 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Diagnosis and Treatment · Radiomics and Machine Learning in Medical Imaging · Head and Neck Cancer Studies
Case Presentation
A 68-year-old man with a history of orthotopic liver transplant maintained on immunosuppression, right upper lobe adenocarcinoma status post chemotherapy and right upper lobectomy eight years prior, and 45-pack-year history of tobacco disorder presented to the clinic for consultation of his chronic cough. As part of his investigation, he underwent a computed tomography (CT) of the chest that was notable for mediastinal lymphadenopathy in the subcarinal and paratracheal regions (Figure 1A and 1B). There was no reported axillary or supraclavicular adenopathy.
He was subsequently referred to pulmonary medicine for endobronchial ultrasound (EBUS) and transbronchial needle aspiration (TBNA) for both diagnostic and staging purposes. However, his scans were reviewed and notable for an enlarged right-sided supraclavicular lymph node, which was not palpable on exam (Figure 2). A point of care ultrasound (POCUS) assessment of his right supraclavicular region with a linear probe demonstrated the findings in Figure 3 and Videos S1 and S2. Based on the patient’s clinical history and findings from the images and videos, we proceeded with ultrasound-guided fine needle aspiration (FNA). This provided a diagnosis of lung cancer and provided staging in a safer and less invasive way than EBUS.
Figure 1: CT scan of the chest with contrast in the mediastinal window and transverse plane showing an enlarged (A) subcarinal and (B) lower right paratracheal lymph node.
CT scan of the chest with contrast in the mediastinal window and coronal plane showing an enlarged right supraclavicular lymph node.
Soft tissue ultrasound image showing an enlarged right supraclavicular lymph node.
Discussion
The tissue diagnosis and staging of all types of lung cancer is foundational for prognosis and establishing an optimal treatment plan. In order to appropriately stage lung cancer, the highest stage should be established using the 8th edition TNM criteria where tumor size (T), nodal involvement (N), and metastasis (M) are all taken into account 1 . Current guidelines for non-small cell lung cancer defines N0 disease as no regional lymph node involvement, N1 disease as involvement of ipsilateral peribronchial and/or ipsilateral hilar lymph nodes, N2 disease as involvement of the ipsilateral mediastinal and/or subcarinal lymph nodes, and N3 involvement of any of the following lymph node groups: contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular nodes 1, 2. In order to establish tissue diagnosis, sampling is needed and can involve the use of CT guided biopsy, navigational bronchoscopy, endobronchial biopsy, EBUS, percutaneous lymph node biopsy, and/or excisional biopsy of supraclavicular nodes. All methods come with their own safety and efficacy profile that include, but are not limited to, pneumothorax, bleeding, infection, bronchospasm, laryngospasm, hypoxemia, hypercarbia, and aspiration 3, 4. These risks are first mediated by proceeding with the method that is considered least invasive and provides the highest staging.
To evaluate the neck region, CT or ultrasound can be used. When evaluating lymph nodes, ultrasonographic characteristics that are more suggestive of malignancy include larger size (>5 mm), rounded shape (as opposed to oval or reniform), irregular borders, and lack of visible hilum 5. If suspicious nodes are found, further evaluation is needed through either percutaneous needle aspiration or open surgical biopsy. Factors limiting the use of surgical sampling include the need for an incision, bleeding, infection, potential need for sedation and missing the node of interest. All of these factors can be either reduced or eliminated with the use of percutaneous needle aspiration, which has demonstrated its utility in the literature 6, 7. While needle aspiration may have risk of bleeding because of its close proximity to the large neck vessels, it is exceedingly rare when done by a trained provider 8, 9, 10. In a study by El-Shaarawy and colleagues, a neck ultrasound in subjects with evidence of intrathoracic lymphadenopathy found abnormal neck lymph nodes in more than one third of patients 7. Additionally, they performed neck lymph node biopsies in eligible patients, which had a diagnostic yield of 92%, similar to previous reports 6, 7. Importantly, tissue sampling can be carried out by pulmonary physicians and avoids more imaging studies, procedures, and potential adverse effects from sedation and anesthesia 11, 12.
In our case, we were able to review the suspicious CT and noted the enlarged supraclavicular lymph node that failed to be reported on the formal read. This is a documented blind spot that has been demonstrated by Hassan et al., to miss 18% of cases of abnormally enlarged supraclavicular lymph nodes, with 55% of those being positive for malignancy. A critically important consideration for ensuring proper staging8, 13. Our initial plan was to pursue EBUS-TBNA to provide tissue sampling and mediastinal staging. However, upon further investigating our patient’s concerning CT findings with POCUS, a suspicious 15 mm right supraclavicular lymph node was found. After discussing the risks, benefits, and alternatives, a percutaneous lymph node biopsy was pursued. The results of our lymph node aspiration were consistent with the patient’s prior adenocarcinoma of the lung. He was referred to oncology and started on systemic chemotherapy.
Practically, suspicious neck lymph nodes are identified using a linear transducer. Lymph nodes are characterized as echodense structures surrounded by a clearly defined hyperechoic capsule that are not collapsible, may have a fatty central hilum, and do not show evidence of blood flow on color or spectral Doppler5. Once location is confirmed, the site is cleaned, a local anesthetic is applied, and if needed, additional sedation mirroring other routine subcutaneous procedures is provided. In our practice, sampling of the identified lymph is done under real-time ultrasound guidance and an in-plane needle approach with 3-5 passes using an 18, 21, or 22 gauge needle and 10 cc syringe assembled in a needle gun (Figure 4, Video S3). This is akin to a version of the traditional view seen with EBUS-TBNA sampling. Each pass is evaluated with rapid on-site examination by the cytopathology team in the procedure room.
Soft tissue ultrasound image showing an the enlarged right supraclavicular lymph node withthe needle visible in its entire length.
Supplementary Material
Video S1Linear probe with vascular settings evaluating the right supraclavicular region.
Video S2Linear probe with vascular settings evaluating the right supraclavicular region with color flow Doppler.
Video S3Linear probe with vascular settings with needle aspiration of the suspicious lymph node.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Goldstraw P Chansky K Crowley J The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer Journal of Thoracic Oncology 201611139512676273810.1016/j.jtho.2015.09.009 · doi ↗ · pubmed ↗
- 2El-Sherief A H Lau C T Wu C C Drake R L Abbott G F Rice T W International Association for the Study of Lung Cancer (IASLC) Lymph Node Map: Radiologic Review with CT Illustration Radio Graphics 2014346168016912531042310.1148/rg.346130097 · doi ↗ · pubmed ↗
- 3Eapen G A Shah A M Lei X Jimenez C A Morice R C Yarmus L Filner J Ray C Michaud G Greenhill S R Sarkiss M Casal R Rice D Ost D E American College of Chest Physicians Quality Improvement Registry, Education, and Evaluation (A Qu IRE) Participants. Complications, consequences, and practice patterns of endobronchial ultrasound-guided transbronchial needle aspiration: Results of the A Qu IRE registry Chest 201314341044105310.1378/chest.12-035023117878 PMC 3616680 · doi ↗ · pubmed ↗
- 4Stahl D L Richard K M Papadimos T J Complications of bronchoscopy: A concise synopsis Int J Crit Illn Inj Sci 201553189952655748910.4103/2229-5151.164995 PMC 4613418 · doi ↗ · pubmed ↗
- 5Satterwhite L G Berkowitz D M Parks C S Bechara I R Central Intranodal Vessels to Predict Cytology During Endobronchial Ultrasound Transbronchial Needle Aspiration Journal of Bronchology & Interventional Pulmonology 201118432232810.1097/LBR.0b 013e 31823577 d 123208626 · doi ↗ · pubmed ↗
- 6Kumaran M Benamore R E Vaidhyanath R Ultrasound guided cytological aspiration of supraclavicular lymph nodes in patients with suspected lung cancer Thorax 20056032292331574144110.1136/thx.2004.029223 PMC 1747328 · doi ↗ · pubmed ↗
- 7Prosch H Strasser G Sonka C Cervical Ultrasound (US) and US-guided Lymph Node Biopsy as a Routine Procedure for Staging of Lung Cancer Ultraschall Med 200728065986031760237010.1055/s-2007-963215 · doi ↗ · pubmed ↗
- 8Hassan M Nicholson T Taylor L Focused Neck Ultrasound and Lymph Node Sampling by Respiratory Physicians in Suspected Lung Cancer Respiration 2022101157623451522110.1159/000517922 · doi ↗ · pubmed ↗