Incidentally found parotid gland lesion in 18F-FDG PET/CT for staging evaluation of patients with hepatocellular carcinoma: remote possibility of metastatic tumor or second primary salivary gland malignancy
Jin Hyung Jung, Yoon Se Lee, Young Ho Jung, Seung-Ho Choi, Soon Yuhl Nam, Hyo Jung Cho, Minsu Kwon

TL;DR
This study finds that parotid gland lesions seen in PET/CT scans of liver cancer patients are mostly benign and not linked to cancer spread.
Contribution
The study provides new insights into the clinical significance of parotid incidental lesions in hepatocellular carcinoma staging.
Findings
Parotid incidental lesions in HCC patients were mostly benign and not metastatic.
PIL incidence was higher in HCC patients compared to healthy controls.
Age, sex, and viral markers were significant risk factors for PILs in HCC patients.
Abstract
We primarily aimed to evaluate whether parotid incidental lesion (PIL) in 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) for staging evaluation of patients with hepatocellular carcinoma (HCC) would represent a possibility of extrahepatic metastasis or second primary malignancy (SPM). Additionally, we explored the incidence of PIL in HCC patients and examined any associated risk factors. We retrospectively analyzed patients with HCC who underwent 18F-FDG PET/CT at our institution from 2010 to 2022. The pathological findings of PILs in HCC patients were investigated for confirmatory identification of the risk of HCC metastasis or SPM in parotid gland. Healthy controls received 18F-FDG PET/CT for health screening were also enrolled to compare the incidence of PILs with HCC patients. Various parameters associated with patient demographics and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
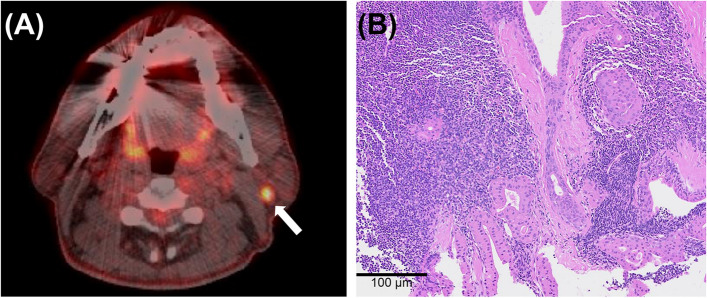 Figure 1
Figure 1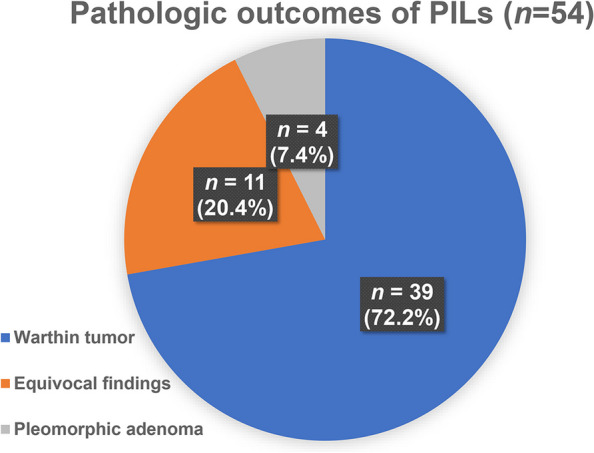 Figure 2
Figure 2- —http://dx.doi.org/10.13039/501100003725National Research Foundation of Korea
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Tumors Diagnosis and Treatment · Head and Neck Cancer Studies · Medical Imaging Techniques and Applications
Background
^18^F-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (^18^F-FDG PET/CT) is a commonly employed imaging modality for staging various malignancies. PET/CT has excellent discriminative power to determine if the primary cancer has metastasized; however, sometimes a non-specific increase in FDG uptake is identified in the form of an incidentaloma, causing ambiguity in staging or requiring further diagnostic evaluation or consultation. In particular, FDG-avid benign tumors (e.g., Warthin tumor and oncocytoma) often occur in the parotid gland, wherein non-specific FDG uptake occasionally increases in the lymph nodes (LNs) or nearby parapharyngeal space. These spaces can therefore cause diagnostic difficulties for patients with cancer who undergo PET/CT [1]. According to the literature, parotid lesions, including incidentaloma, are found in 2.1% of patients with head and neck cancer during PET/CT scans, reporting 0.4% to 1.1% of cancers originating from outside the head and neck region is not uncommon [2–4].
Liver cancer is the sixth most common cancer in South Korea, and the major histopathology is hepatocellular carcinoma (HCC) [5]. At the time of diagnosis, HCC has often already reached an advanced stage, so accurately staging the cancer during initial evaluation is critical to determine the treatment modality and prognosis of the patients. Extrahepatic metastasis (EHM) is observed in approximately 13% of patients with HCC. In this case, the prognosis is extremely poor and a multidisciplinary approach is required to determine therapeutic strategies, it is therefore necessary to thoroughly check for metastasis before treatment [6, 7]. EHM primarily occurs in the lungs, bones, and intra-abdominal LNs or organs, but exactly when it occurs in the head and neck area remains undetermined [8]. Especially in HCC patients planning for hepatectomy or liver transplantation, it is crucial to assess the presence of EHM through PET/CT. In clinical practice, the discovery of parotid incidental lesion (PIL) in these patients is occasionally noted; however, there is a lack of prior research on whether these PILs represent important malignant conditions such as EHM of HCC or secondary primary malignancies (SPMs) in the salivary glands.
A remote lesion discovered incidentally during the staging step of a patient complicates the diagnostic process, delays treatment, and causes psychological anxiety for the patient. Therefore, investigating the frequency and histological examination results of the PIL observed on PET/CT in patients with HCC for whom no prior studies have been conducted will provide a guide for patient diagnosis and treatment decision-making. This study therefore aimed to analyze the frequency of PILs identified on PET/CT during HCC patient staging and investigate the pathological results of these lesions. In addition, we endeavored to analyze the characteristics of patients with HCC that affect the frequency of PILs.
Materials & methods
Patients and variables
We retrospectively analyzed the electronic medical records of patients with HCC who had undergone ^18^F-FDG PET/CT scans at our single tertiary referral hospital from 2010 to 2022. Patients with recurrent HCC or with a history of head and neck area malignancies, including primary parotid cancers, were excluded. The additional radiographs (including computed tomography, magnetic resonance image, or ultrasonography) and pathological evaluation of PILs through fine needle aspiration cytology or core needle biopsy in HCC patients were introduced to identify the risk of HCC metastasis or SPM in parotid gland. We also set a control group comprising patients who underwent ^18^F-FDG PET/CT scans for health screening during the same period to investigate the incidence of PIL compared with patients with HCC. To analyze the characteristics of HCC affecting the frequency of PILs, we inspected patient demographics (age, sex, smoking history, alcohol consumption amount) and HCC-associated parameters (tumor size as well as stage based on the Surveillance, Epidemiology, and End Results [SEER] classification, and alpha-fetoprotein [AFP] levels). Furthermore, we investigated whether the presence of hepatitis B virus (HBV) and hepatitis C virus (HCV) viral markers would affect the incidence of PIL, considering the previously reported association between head and neck squamous cell carcinoma and chronic HBV and HCV infections [9, 10]. This study was conducted with the approval of the Institutional Review Board of the hospital (IRB No. 2022–1684), and the requirement for patient consent was waived due to the retrospective nature of the analysis.
Statistical analysis
Fisher's exact test or Student’s t-test was performed to compare the characteristics between patients with HCC and healthy controls with PIL. Logistic regression analysis was used to analyze the odds ratio (OR) of PIL in the patients with HCC. All statistical analyses were performed using IBM SPSS (ver. 22.0; IBM Corp, Armonk, NY), and statistical significance was defined as a two-sided P-value of less than 0.05.
Results
Incidence and pathologic findings of PIL
Table 1 presents the demographics of all the patients. During the study period, 17,674 patients with HCC and 2,090 healthy individuals who underwent health checkups were enrolled. Among them, PET/CT scans revealed PIL in 485 (2.7%) patients with HCC (a representative case depicted in Fig. 1) and 23 (1.1%) in the control cohort, and the incidence of PIL was significantly higher in the patients with HCC (p < 0.001). We also performed statistical analysis by matching the two groups, given the differences in the age and sex distributions. The analyses revealed that 6,380 HCC group patients and 1,595 control group patients were matched at a 4:1 ratio. Even after matching, the occurrence of PIL in the HCC group (n = 118, 1.85%) was higher than in the control group (n = 15, 0.94%) (OR = 1.985, 95% CI: 1.157 − 3.406, p = 0.013, Table 1). Table 1. Characteristics of subjects in each groupHCC group (n = 17,674)Control group (n = 2,090)PAge (year), mean ± SD58.7 ± 10.255.3 ± 10.3 < 0.001Sex, male/female14,315 (81) / 3359 (19)920 (44) / 1170 (56) < 0.001Smoking historyneverever or currentunknown946 (5.4)3542 (20)13,186 (74.6)686 (32.8)226 (10.8)1178 (56.4) < 0.001Alcohol intakeneversocial or heavyunknown3131 (17.7)6599 (37.3)7944 (45)221 (10.6)16 (0.8)1853 (88.7) < 0.001HBsAgnegativepositiveunknown10,606 (60)1886 (10.7)5155 (29.2)N/AN/AAnti-HCV antibodynegativepositiveunknown12,253 (64.4)239 (13.5)5155 (29.2)N/AN/AAFP (ng/ml), mean ± SD10,121.1 ± 91,585.4N/AN/ASEER stageDM ( −)DM ( +)unknown15,580 (88.2)1007 (5.7)1086 (6.2)N/AN/APIL485 (2.7)23 (1.1) < 0.001**HCC group (n = 6,380)****Control group (n = 1,595)****OR (95% CI)**PPIL^a^118 (1.85)15 (0.94)1.985 (1.157 − 3.406)0.013Data expressed as number (%)AFP alpha-fetoprotein, CI confidence interval, DM distant metastasis, HBsAg hepatitis B surface antigen, HCC hepatocellular carcinoma, HCV hepatitis C virus, N/A not assessable, OR odds ratio, SD standard deviation, SEER surveillance, epidemiology, and end result, PIL parotid incidental lesion^a^After matching at a 4:1 ratio to adjust for differences in age and sex distribution between the two groupsFig. 1A representative patient case. A A representative case with a 50-year-old male undergoing staging workup for HCC having a focal hypermetabolic lesion in the left parotid gland (white arrow) with a maximum standardized uptake value of 5.5 on ^18^F-fluorodeoxyglucose positron emission tomography/computed tomography. B A core needle biopsy of the left parotid gland confirmed the presence of a Warthin tumor (hematoxylin & eosin stain, original magnification × 100)
Out of 485 cases of PIL, in instances where the PET/CT interpreting physician recommended further evaluation for differential diagnosis, additional radiographs and tissue examinations were conducted. However, actual histopathological confirmations were performed in only 54 (11.1%) cases.. The most common pathologic finding was Warthin tumor (n = 39, 73.6%), followed by equivocal results (e.g., lymphoid tissue, abscess, necrotic tissue, reactive hyperplasia, or acellular tissue [n = 11, 8.8%]), and pleomorphic adenoma (n = 4, 7.6%); however, no malignant lesions were observed, including EHM of HCC (Fig. 2).Fig. 2. The pathological outcomes of parotid incidental lesions (PIL, n = 54)
Risk factors for PIL in HCC patients
We performed another comparison within patients with HCC to investigate the risk factors associated with the presence of PIL. Risk factors included older age, male sex, and HBsAg and anti-HCV positivity (all p < 0.001). In the logistic regression analysis, age (OR = 1.028, 95% CI: 1.019 − 1.037, p < 0.001), male sex (OR = 3.082, 95% CI: 2.181 − 4.357, p < 0.001), HBsAg positivity (OR = 6.891, 95% CI: 5.447–8.717, p < 0.001), and anti-HCV positivity (OR = 3.776, 95% CI: 2.328 − 6.125, p < 0.001) significantly increased the risk of PILs. However, initial tumor size, AFP level, and SEER stage did not yield any statistically significant association with PIL presence (Table 2). Table 2. Univariate and logistic regression analyses on parameters affecting the prevalence of parotid incidental lesionVariables****PIL ( +) (n = 485)PIL ( −) (n = 12,199)P**OR (95% CI)**PAge (years), mean ± SD61.4 ± 9.758.6 ± 10.3 < 0.0011.028 (1.019–1.037) < 0.001Sex, male/female450 (92.8) / 35 (7.2)13,865 (80.7) / 3324 (19.3) < 0.0013.082 (2.181–4.357) < 0.001HBsAg, positive/negative156 (53.2) /137 (46.8)1730 (14.2) / 10,469 (85.8) < 0.0016.891 (5.447 − 8.717) < 0.001Anti-HCV, positive/negative19 (6.5) / 274 (93.5)220 (1.8) / 11,979 (98.2) < 0.0013.776 (2.328–6.125) < 0.001AFP (µg/mL), mean ± SD8.772 ± 84.927.455 ± 73.980.7641 (1 − 1)1HCC size (cm), mean ± SD4.5 ± 3.54.6 ± 8.90.9320.999 (0.983 − 1.015)0.932SEER stage, DM( −)/DM( +)290 (93.5) / 16 (5.5)11,518 (94.4) / 599 (4.9)0.6561.173 (0.732 − 1.879)0.507Data expressed as number (%)Blood tests about HBsAg, Anti-HCV, and AFP were performed within 3 months before PET/CTAFP alpha-fetoprotein, DM distant metastasis, HBsAg hepatitis B surface antigen, HCC hepatocellular carcinoma, HCV hepatitis C virus, PIL parotid incidental lesion, SEER surveillance epidemiology and end result
Discussion
In patients with HCC, tumor stage is used to predict the clinical course and determine the treatment method. EHM of HCC is not uncommon, and the probability of identifying EHM is higher in patients with advanced intrahepatic HCC. The prognosis of these patients is poor, and a systemic agent such as sorafenib is the only therapeutic option [11]. To accurately determine the HCC stage, a test for EHM is required, for which ^18^F-FDG PET/CT is an established tool [12, 13]. Moreover, upstaging reportedly occurred in 5.9% patients with HCC, among which EHM was identified in 1.4% when PET/CT was performed before the initial treatment, consequently leading to the changed treatment policy in 9.9% of those patients [14, 15]. Therefore, PET/CT should be actively considered in patients with HCC, especially when planning surgical treatment for curative purposes, such as hepatectomy or liver transplantation.
According to a recent systematic review, the overall prevalence of PIL in various primary tumor staging examinations using ^18^F-FDG PET/CT was 0.74%, with a significantly higher frequency observed in patients with lung cancer [16]. In our study, PIL was detected in 2.7% of patients with HCC, showing a higher prevalence compared with other non-head and neck primary cancers, and a higher likelihood of detection in patients with head and neck cancer (2.1%) [3]. The etiology of HCC primarily includes hepatitis virus infection, as well as factors such as male sex, old age, smoking, and alcohol consumption, which are also risk factors for primary parotid tumors [17]. Therefore, it is presumed that the higher frequency of such risk factors in the HCC group compared to the control group, might have contributed to the difference in PIL incidence. However, even after adjusting for the aforementioned common risk factors, the higher frequency of PIL in the HCC group compared to the control group suggests that HCC itself may increase the incidence of PIL.
According to the aforementioned systematic review by Thompson and colleagues, the majority of tumors found in cases wherein histological confirmation was available were benign, such as Warthin tumor (cystadenoma). However, malignant lesions were identified in approximately 30% of cases, including metastatic LNs and primary parotid gland malignancies [16]. In contrast, among the 54 patients in our study who underwent histological confirmation for PIL, no malignant lesions were found. Case reports of HCC metastasis to the head and neck region are rarely confirmed justly in the literature. While metastasis to the oral or pharyngeal mucosa is occasionally reported, there was only one case of metastasis to the parotid gland reported [18–22]. Collectively, while the incidence of PIL in patients with HCC on PET/CT is relatively higher, the likelihood of detecting malignant lesions, including EHM of HCC, appears to be extremely low.
In our study, we confirmed that PIL was highly likely to be identified if the patient with HCC had risk factors such as male sex, old age, positive HBsAg, or anti-HCV. An interesting observation is that the frequency of PIL was higher in HCC cases with positive markers for hepatitis viruses. Hepatitis virus infection is a proven risk factor for the development of another extrahepatic primary malignancy [23, 24]. This is attributed to the presence of factors such as hepatitis B virus X protein, which can lead to genetic instability and an immunosuppressive condition, thereby increasing the risk of developing malignancies in other organs [25]. Our study was initiated based on previous literature suggesting that hepatitis virus infection also increases the risk of developing head and neck cancer [9, 10]. We therefore wondered whether the presence of PIL in hepatitis virus-positive patients with HCC could lead to a higher risk not only for EHM but also for the development of secondary primary salivary gland cancer. However, in our study, we did not observe any cases of EHM or primary salivary gland cancer in the PIL confirmed through tissue examination. Most of the non-malignant lesions were salivary gland-origin benign tumors, with Warthin tumors being the most commonly observed among them. Warthin tumor is associated with predisposing factors such as male sex, old age, and heavy smoking. Recently, there have been reports linking it to infections of human papillomavirus or Epstein–Barr virus, as well as associations with chromosomal instability [26, 27]. Considering these factors, it is also plausible to speculate about a potential association between Warthin tumor development and hepatitis virus infection to explain the phenomenon of an increased frequency of PIL and benign salivary gland tumors in HCC patients with positive hepatitis virus markers. Despite the insights gained from our study, further research is warranted to gain a comprehensive understanding of the underlying mechanisms contributing to the higher incidence of PIL in HCC patients.
The main limitation of this study is its retrospective nature. The inability to ascertain the status of patients who did not undergo histological examinations is a crucial limitation of our study. Given the retrospective design of this study, when the PET/CT interpreting physician did not recommend additional tests for differential diagnosis among the 485 cases of PIL, most patients were not referred separately to the otolaryngology department or did not undergo further testing for PIL. This made it challenging to assess their condition. And the comparison of incidence rates and identification of risk factors for PIL were conducted in different populations, which subsequently led to the limited data set and comparisons. Additionally, the use of ^18^F-FDG PET/CT scans in patients with HCC is somewhat limited to those scheduled for surgical treatment owing to the insurance system and liver cancer treatment guidelines in our country. Another limitation of our study would be lack of analysis the relationship between quantitative FDG uptake of variety benign parotid tumors. However, our study represents the first report confirming the relatively higher incidence and totally benign pathologic results of PIL in patients with HCC. Our study can offer valuable guidance on the need for additional examinations and otolaryngology consultations, especially in patients with HCC who are candidates for urgent hepatectomy or liver transplantation.
Conclusion
We observed that ^18^F-FDG PET/CT scans identified PIL more frequently in patients with HCC compared with healthy controls, with a prevalence of 2.7% and 1.1%, respectively. Several factors influence the incidence of PIL in patients with HCC, including older age, male sex, positive HBsAg status, and positive anti-HCV status. Notably, all of PIL detected and tissue-confirmed in patients with HCC was benign, given that no malignant lesions, including EHM, were identified. Therefore, the presence of PIL should not impede or delay the treatment process for patients with HCC. Additionally, we suggested that for future swift and straightforward differential diagnoses of PIL, the development of additional protocols within the PET/CT imaging could be beneficial.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rassekh CH Cost JL Hogg JP Hurst MK Marano GD Ducatman BS Positron emission tomography in Warthin's tumor mimicking malignancy impacts the evaluation of head and neck patients Am J Otolaryngol 20153625926310.1016/j.amjoto.2014.11.00825523505 · doi ↗ · pubmed ↗
- 2Makis W Ciarallo A Gotra A Clinical significance of parotid gland incidentalomas on (18)F-FDG PET/CT Clin Imaging 20153966767110.1016/j.clinimag.2015.03.01125888252 · doi ↗ · pubmed ↗
- 3Seo YL Yoon DY Baek S Lim KJ Yun EJ Cho YK Incidental focal FDG uptake in the parotid glands on PET/CT in patients with head and neck malignancy Eur Radiol 20152517117710.1007/s 00330-014-3397-125182627 · doi ↗ · pubmed ↗
- 4Üstün F Taştekin E TaşA Altun GD The Clinical Significance of Incidental Parotid Uptake in a PET/CT Study: A Diagnostic Algorithm Curr Med Imaging Rev 20191532633310.2174/157340561466617121316024431989884 · doi ↗ · pubmed ↗
- 5Chon YE Jeong SW Jun DW Hepatocellular carcinoma statistics in South Korea Clin Mol Hepatol 20212751251410.3350/cmh.2021.017134153973 PMC 8273634 · doi ↗ · pubmed ↗
- 6Kanda M Tateishi R Yoshida H Sato T Masuzaki R Ohki T Extrahepatic metastasis of hepatocellular carcinoma: incidence and risk factors Liver Int 2008281256126310.1111/j.1478-3231.2008.01864.x 18710423 · doi ↗ · pubmed ↗
- 7Lee HS Management of patients with hepatocellular carcinoma and extrahepatic metastasis Dig Dis 20112933333810.1159/00032757221829026 · doi ↗ · pubmed ↗
- 8Uka K Aikata H Takaki S Shirakawa H Jeong SC Yamashina K Clinical features and prognosis of patients with extrahepatic metastases from hepatocellular carcinoma World J Gastroenterol 20071341442010.3748/wjg.v 13.i 3.41417230611 PMC 4065897 · doi ↗ · pubmed ↗