A Surgeon's Challenge: Diagnosing and Managing Hidden Bile Duct Stones Post-cholecystectomy
Guangbin Chen, Ke Wang, Yanguang Sha, Dingbang Wang, Zhigang Liu

TL;DR
This case report highlights the challenges of diagnosing and treating hidden bile duct stones after gallbladder surgery.
Contribution
The report emphasizes the need for advanced imaging and multidisciplinary care in managing post-cholecystectomy bile duct stones.
Findings
Conventional preoperative diagnostics failed to detect the hidden bile duct stone.
ERCP with sphincterotomy successfully extracted the stone.
A multidisciplinary approach is crucial for optimal outcomes in such cases.
Abstract
This case report details the diagnostic and management challenges encountered with hidden bile duct stones post-cholecystectomy in a 58-year-old female patient. Despite a successful laparoscopic cholecystectomy, the patient developed sudden upper abdominal pain and jaundice, leading to the discovery of an impacted bile duct stone. The case underscores the limitations of conventional preoperative diagnostics and highlights the importance of advanced imaging techniques and a multidisciplinary approach for optimal outcomes. The successful extraction of the stone via endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy demonstrates the efficacy of this therapeutic strategy. This report emphasizes the need for heightened vigilance and comprehensive evaluation in the postoperative management of gallstone disease, contributing valuable insights into the complexities of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
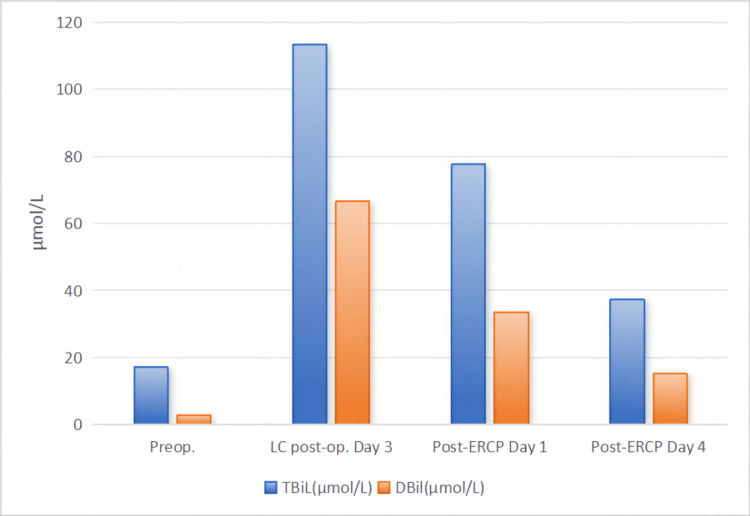 Figure 1
Figure 1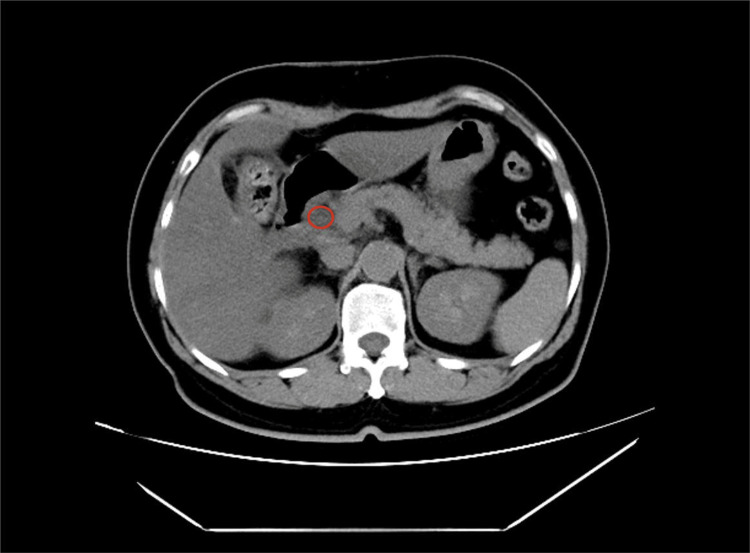 Figure 2
Figure 2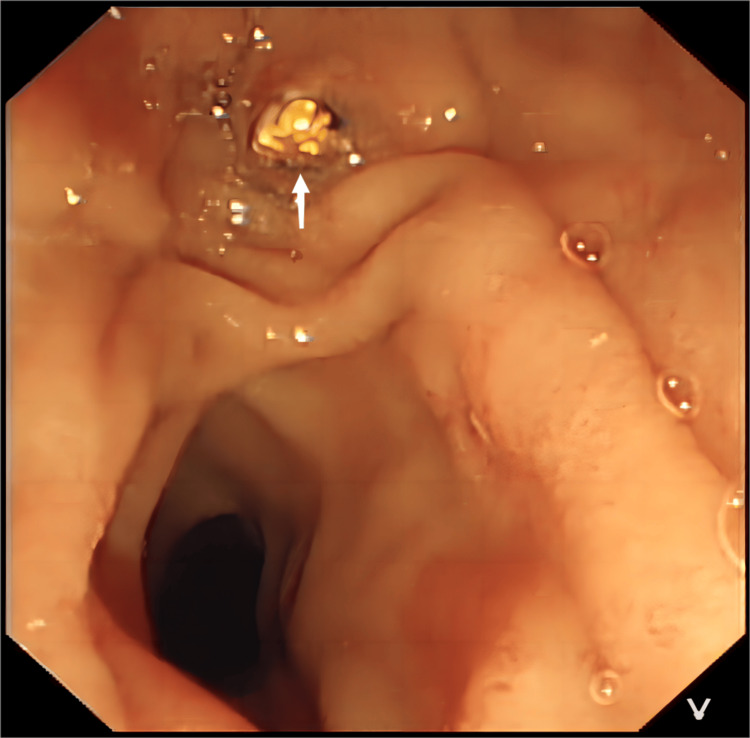 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments · Biliary and Gastrointestinal Fistulas
Introduction
In the realm of gallstone disease management, the post-cholecystectomy period poses unique challenges, particularly with the occurrence of hidden bile duct stones [1]. Despite the widespread adoption of laparoscopic cholecystectomy (LC) for its minimally invasive benefits, patients can still face significant postoperative complications, such as choledocholithiasis [2]. This condition not only complicates recovery but also necessitates a nuanced approach to diagnosis and treatment. Traditional diagnostic tools often prove inadequate for identifying these concealed stones, highlighting the need for advanced imaging techniques and a collaborative, multidisciplinary strategy for effective management [2,3]. This case report delves into the complexities of diagnosing and managing hidden bile duct stones post-cholecystectomy, underscoring the critical need for vigilance and comprehensive evaluation in achieving optimal patient outcomes.
Case presentation
A 58-year-old female patient was admitted to the hospital due to recurrent discomfort and bloating pain in the right upper abdomen for the past six months. The symptoms intensified with physical activity and after meals but subsided upon resting. The patient did not exhibit symptoms such as chills, high fever, nausea, or vomiting. Upon evaluation in our department, no significant signs of jaundice were observed in the skin or sclera. The patient's appetite, bowel movements, sleep, and mental state remained unaffected. Her medical history included hypertension and type II diabetes, which she managed for five years, and a prior surgical intervention for a left humerus fracture.
Diagnostic tests conducted upon admission revealed the following serological indicators: white blood cells (WBC) at 6.68×10^9^/L, neutrophil percentage (NEUT%) at 49.5%, and liver function tests indicating alanine aminotransferase (ALT) at 32 U/L, aspartate aminotransferase (AST) at 21 U/L, gamma-glutamyl transferase (γ-GT) at 24 U/L, alkaline phosphatase (ALP) at 108 U/L, total bilirubin (TBiL) at 17.1 μmol/L, direct bilirubin (DBil) at 2.8 μmol/L (Figure 1), and amylase (AMY) at 66 U/L. Tumor markers were within normal limits: alpha-fetoprotein (AFP) at 2.41 ng/ml, carcinoembryonic antigen (CEA) at 1.2 ng/ml, and carbohydrate antigen 19-9 (CA19-9) at 22 U/ml. An ultrasound examination revealed chronic cholecystitis, multiple gallstones with the largest measuring approximately 2.0×1.4 cm, and no significant dilation or abnormal echoes observed in the upper segment of the common bile duct.
Perioperative changes in bilirubin.Preop: preoperative; LC: laparoscopic cholecystectomy; op: operative; ERCP: endoscopic retrograde cholangiopancreatography; TBiL: total bilirubin; DBil: direct bilirubin
The patient underwent a routine LC on November 17, 2023, which was executed successfully. However, on the first postoperative day, she developed sudden upper abdominal pain and noticeable jaundice in the sclera and skin. A subsequent reevaluation of her liver function revealed significantly elevated levels: ALT at 615 U/L, AST at 541 U/L, γ-GT at 380 U/L, ALP at 325 U/L, TBiL at 113.3 μmol/L, and DBil at 44.0 μmol/L (Figure 1), with AMY at 516 U/L. An emergency abdominal CT scan suggested a common bile duct stone (Figure 2). Further investigation via endoscopic retrograde cholangiopancreatography (ERCP) identified an impacted stone at the duodenal papilla (Figure 3). An endoscopic sphincterotomy (EST) was performed, and the stone was successfully extracted using a basket. Following the procedure, the patient's symptoms were alleviated, and her liver function normalized (Figure 1).
Postoperative CT scan of the upper abdomen showed a stone (marked in red) in the lower part of the common bile duct.CT: computed tomography
Postoperative ERCP examination suggests an impacted stone (white arrow) at the duodenal papilla.ERCP: endoscopic retrograde cholangiopancreatography
Discussion
The management of choledocholithiasis, particularly when it presents after LC, poses a significant challenge to surgeons worldwide [4,5]. This case report underscores the complexities involved in diagnosing and treating hidden bile duct stones post-cholecystectomy, a scenario that is not uncommon but often underreported in clinical literature.
In recent years, the global incidence of gallbladder stones has seen a notable increase, attributed largely to dietary changes and improvements in quality of life [1,6,7]. Concurrently, the prevalence of choledocholithiasis, especially in the postoperative phase, has become a point of concern [1]. Our case highlights a patient who, following a seemingly successful LC, presented with symptoms indicative of bile duct obstruction. This situation underscores the critical need for a high index of suspicion for choledocholithiasis in patients post-cholecystectomy, especially when presenting with jaundice, abdominal pain, and elevated liver enzymes.
In most countries and regions, routine preoperative evaluations for cholecystectomy typically include liver function tests and abdominal ultrasound examinations [7-9]. If these indicators do not reveal abnormalities, further investigations, such as magnetic resonance cholangiopancreatography (MRCP), are often not pursued, particularly in cost-sensitive healthcare settings. However, as demonstrated in our case, these methods may not always be sufficient. The stone in question, measuring approximately 0.8 cm in diameter, was not detected by ultrasound examination preoperatively due to its floating nature in the lower segment of the common bile duct, coinciding with normal liver function tests at the time. This oversight brings to light the limitations of conventional diagnostic tools and the potential role of more advanced imaging techniques, such as MRCP, in the preoperative evaluation of gallstone disease.
The therapeutic strategies for managing choledocholithiasis post-LC include ERCP with sphincterotomy and stone extraction [9,10], which was successfully employed in our case. This method, while effective, is not without risks and underscores the importance of a multidisciplinary approach in the management of these patients. The decision-making process should involve a thorough evaluation of the risks and benefits, patient preferences, and the expertise available within the treating institution.
Conclusions
This case report serves as a critical reminder of the challenges and complexities in diagnosing and managing hidden bile duct stones post-cholecystectomy. It underscores the need for vigilance, the potential limitations of preoperative diagnostics, and the importance of considering advanced imaging techniques in the preoperative assessment of patients with gallstone disease. Moreover, it highlights the significance of a multidisciplinary approach in ensuring optimal outcomes for patients facing this complex condition.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A clinician's guide to gallstones and common bile duct (CBD): a study protocol for a systematic review and evidence-based recommendations Health Sci Rep Sebghatollahi V Parsa M Minakari M Azadbakht S 06202310.1002/hsr 2.1555 PMC 1049646037706014 · doi ↗ · pubmed ↗
- 2Choledocholithiasis: a review of management and outcomes in a regional setting Cureus Zouki J Sidhom D Bindon R Sidhu T Chan E Lyon M 015202310.7759/cureus.50223 PMC 1077346838192960 · doi ↗ · pubmed ↗
- 3Diagnosis and management of choledocholithiasis in the golden age of imaging, endoscopy and laparoscopy World J Gastroenterol Costi R Gnocchi A Di Mario F Sarli L 13382134012020142530907110.3748/wjg.v 20.i 37.13382 PMC 4188892 · doi ↗ · pubmed ↗
- 4Clinical spotlight review for the management of choledocholithiasis Surg Endosc Narula VK Fung EC Overby DW Richardson W Stefanidis D 148214913420203209595210.1007/s 00464-020-07462-2 · doi ↗ · pubmed ↗
- 5The role of laparoscopic ultrasonography in the evaluation of suspected choledocholithiasis. A single-center experience Medicina (Kaunas) Atstupens K Mukans M Plaudis H Pupelis G 56202010.3390/medicina 56050246 PMC 727926232443814 · doi ↗ · pubmed ↗
- 6Risk factors for gallstone disease in Shanghai: an observational study Medicine (Baltimore) Gu Q Zhou G Xu T 099202010.1097/MD.0000000000018754 PMC 722040132011459 · doi ↗ · pubmed ↗
- 7EASL clinical practice guidelines on the prevention, diagnosis and treatment of gallstones J Hepatol 1461816520162708581010.1016/j.jhep.2016.03.005 · doi ↗ · pubmed ↗
- 8Evidence-based clinical practice guidelines for cholelithiasis 2021 J Gastroenterol Fujita N Yasuda I Endo I 8018335820233745285510.1007/s 00535-023-02014-6PMC 10423145 · doi ↗ · pubmed ↗