Large saccular aneurysm of the right coronary artery
Gijs J. van Steenbergen, Florien Klein, Thomas P. Mast, Pieter-Jan Vlaar, Koen Teeuwen

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
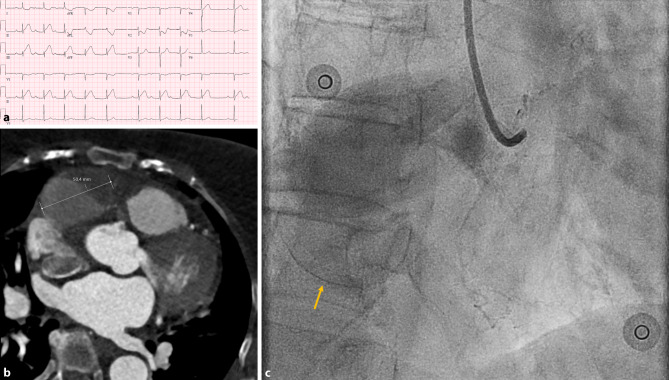 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKawasaki Disease and Coronary Complications · Coronary Artery Anomalies · Cardiac Structural Anomalies and Repair
An 81-year-old woman with no significant cardiovascular history experienced progressive, non-exertional chest pain. Following hospital admission, the electrocardiogram (ECG) revealed ST-segment elevation inferior, leading to a diagnosis of acute inferior myocardial infarction (Fig. 1a). Emergent coronary angiography revealed a giant saccular aneurysm in the proximal right coronary artery (RCA) with significant thrombus, resulting in occlusion (Fig. 1b; Video S1 in Electronic Supplementary Material [ESM]). A subsequent computed tomography scan demonstrated the aneurysm to measure 5 cm in size (Fig. 1c; Videos S2 and S3 in Electronic Supplementary Material [ESM]).Fig. 1. Multi-modality imaging of a giant saccular right coronary artery aneurysm. a Electrocardiogram showing ST elevations in the inferior leads and a third-degree atrioventricular block indicative of acute inferior wall myocardial infarction. b Coronary angiogram demonstrating a large saccular aneurysm in the proximal right coronary artery with a calcified wall (yellow arrow) that extends beyond the contrast-filled area, hinting at the presence of extensive thrombus (see also video S1 in Electronic Supplementary Material [ESM]). c The computed tomography angiogram showcases the saccular structure of the 5 cm aneurysm, and further confirms extensive thrombus formation (dark grey area). There was no contrast filling of the distal right coronary artery, indicating occlusion which corroborates with the findings on coronary angiography (see videos S2 and S3 in Electronic Supplementary Material [ESM])
Saccular coronary artery aneurysms, although rare, can cause severe clinical challenges. Therapeutic options vary based on the aneurysm’s size, location and shape, and can include endovascular coiling, surgical clipping, and the use of covered stents [1]. In our case, attempts to gain entry into the RCA were unsuccessful and prompted a conservative medical treatment. Given the presence of ectasia in both the left anterior descending artery and the circumflex artery, low-dose rivaroxaban was added to her existing antiplatelet therapy.
Supplementary Information
Video S1: Coronary angiogram Video S2: Computed tomography scan Video S3: 3D reconstruction based on computed tomography scan
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kawsara ANúñez GI Alqahtani F Management of Coronary Artery Aneurysms J Am Coll Cardiol Intv 2018111211122310.1016/j.jcin.2018.02.041 · doi ↗