The paramount of three-dimensional echocardiography in percutaneous closure of large oval perimembranous ventricular septal defect: a case report
Sisca Natalia Siagian, Yovi Kurniawati

TL;DR
This case report shows how 3D echocardiography helped successfully close a rare large oval-shaped heart defect that traditional methods failed to measure correctly.
Contribution
Highlights the use of 3D echocardiography for accurate sizing of oval-shaped perimembranous VSDs during transcatheter closure.
Findings
Conventional echocardiography underestimated the size of the oval-shaped VSD.
3D echocardiography provided accurate measurements leading to successful device closure.
Upsizing the device based on 3D imaging resulted in no residual defect or arrhythmia after 6 months.
Abstract
Ventricular septal defect (VSD) is the most common type of congenital heart abnormality with perimembranous VSD (pmVSD) accounting for ∼70% of all VSD. Nowadays, transcatheter closure is the first choice for suitable pmVSD. However, there was no report about closing the large oval-shaped VSD percutaneously. A 34-year-old male with known VSD was referred for transcatheter closure after failed attempts in other hospital. Patient had been diagnosed with VSD at a young age, but he was lost to follow-up. He presented with shortness of breath due to heart failure and pulmonary hypertension. The initial measurement of the defect was 6–7 mm by transthoracic echocardiography (TTE), transoesophageal echocardiography (TEE), and LV angiography. However, re-measurement using TEE and 3D echocardiography revealed that the VSD is oval with diameters of 18 mm × 6 mm. Initially, device No. 12/14 was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1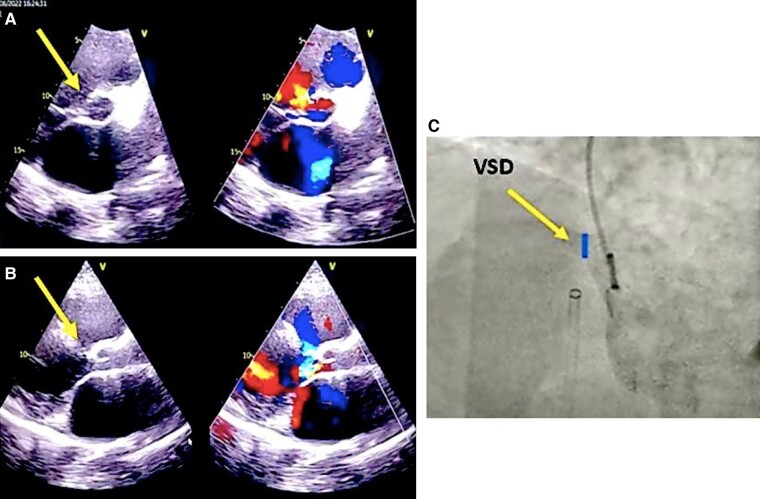 Figure 1
Figure 1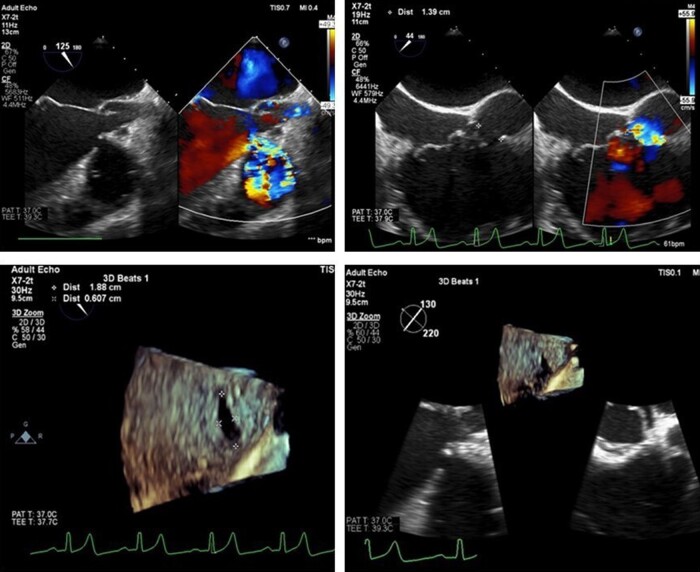 Figure 2
Figure 2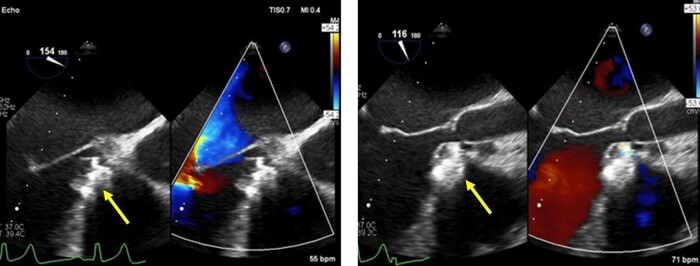 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEngineering Applied Research · Diverse Approaches in Healthcare and Education Studies
Introduction
Ventricular septal defect (VSD) stands as the predominant congenital cardiac anomaly, with perimembranous VSD comprising ∼70% of all VSD cases.^1^ Treatment modalities encompass surgical repair and percutaneous device closure.^2^ Notably, advancements in interventional techniques within cardiac catheterization have progressed significantly in recent years, rendering percutaneous closure the preferred option. Nevertheless, adherence to specific criteria and careful selection of the occluder’s appropriate size remain crucial considerations.^1,3,4^
Summary figure
Timeline of the case presentation
**
Case presentation
A 34-year-old male presented to our centre, reporting shortness of breath a year prior to his current admission, accompanied by a history of unsuccessful intervention at a previous hospital. During childhood, he experienced recurrent respiratory tract infections and was diagnosed with VSD at the age of 12. Unfortunately, he was lost to follow-up and did not receive appropriate treatment thereafter. One year ago, in June 2022, the patient sought medical attention at a private hospital due to heart failure symptoms, including breathlessness and oedema in extremities. Echocardiography and right heart catheterization confirmed perimembranous VSD with pulmonary hypertension, evidenced by a flow ratio of 2.14, pulmonary vascular resistance index 3.6 WU·m^2^, and resistance ratio 0.12. The defect size, measured via echocardiography and left ventricular angiography, was 6–7 mm (Figure 1). Despite medication, an attempt at VSD transcatheter closure proved unsuccessful, prompting consideration of surgical correction or a repeat percutaneous procedure at a tertiary centre with enhanced resources.
VSD assessment in the previous hospital, defect measurement from TEE (A and B) and LV angiography (C), pointed by the yellow arrows.
During the examination at our centre, the patient was compos mentis, with blood pressure of 134/70 mmHg, a regular heart rate of 79 beats per minute, respiratory rate of 30 breaths per minute, oxygen saturation levels of 97%, a temperature of 36.1°C, and weight/height of 94 kg/165 cm. Cardiac examination revealed normal first and second heart sounds, along with a pansystolic murmur, while lungs displayed no rales or wheezing. Other physical examinations yielded normal results. Laboratory tests were mostly within normal limits, except for slightly elevated ALT and AST. ECG indicated sinus rhythm with a heart rate of 75 beats per minute and biventricular hypertrophy. Chest X-ray illustrated cardiomegaly with left ventricular hypertrophy. Echocardiography detailed a large VSD (6–7 mm) with a transVSD pressure gradient of 37 mmHg, mild tricuspid regurgitation (transvalvular gradient of 36 mmHg), moderate mitral regurgitation, and dilated left atrium and ventricle. Left ventricular systolic function was diminished, with an ejection fraction ranging from 42–50% (Teich and eyeballing) and 46% (Simpson), while the left ventricle dimensions at end-diastolic and end-systolic were 92 and 72 mm, respectively.
Considering the heightened surgical risk due to decreased ejection fraction and pulmonary hypertension, the patient was deliberated for transcatheter VSD closure with a larger device after consultation with our surgical team. Three-dimensional transoesophageal echocardiography (3D TEE) revealed an oval-shaped VSD with diameters of 18 × 6 mm (Figure 2). Despite using the Lifetech HeartR occluder No. 12/14 based on the newly measured size and previous closure attempts, the device proved unstable with a significant peripheral residual shunt, persisting even after two repositioning attempts. To address this, we opted to upsize the device to Lifetech HeartR occluder No. 16/18, acknowledging the potential risk of atrioventricular (AV) block due to AV node disturbance. The delivery sheath was carefully inserted, followed by the device, with TEE guiding each step of the procedure. Deployment on one side was followed by the other. Post-procedural assessment indicated the device stowed in place with satisfactory ECG and haemodynamics, leading to the decision to release the device. Over the subsequent 6 months, the patient exhibited a well-seated device with no residual shunt, valve impingement, or AV block (Figure 3).
3D echocardiography showing oval-shaped pmVSD with diameter of 18 × 6 mm.
Post-procedural TEE. Device Lifetech 16/18 seated well with no residual of VSD right after the intervention and also during follow-up 1 week and 6 months afterward.
Discussion
The natural progression of VSD is contingent upon factors such as its size, location, and the relative resistances in the pulmonary and systemic vascular beds.^1^ Perimembranous defects may, in some cases, spontaneously decrease in size or close through an aneurysm.^2^ In the case presented, the patient was lost to follow-up, allowing the large defect to persist into adulthood. Upon returning to the hospital after decades with dyspnoea, further evaluation revealed heart failure with reduced ejection fraction and pulmonary hypertension. Given the increased risk associated with surgical closure, the balance leaned towards transcatheter closure, supported by advancements in cardiac imaging modalities and techniques, along with diverse occlusion systems. The transcatheter closure of perimembranous VSDs has gained acceptance, although it remains a challenging procedure.^3,4^
Measurements of defect size and distance from the aortic and tricuspid valve are typically confirmed using both angiography and echocardiography.^5^ Most centres use angiography to confirm the size, location, and shunt magnitude, which is the most accurate modality for intraoperative guidance.^6^ Of all the variables considered for device selection, the location, morphology, as well as length and thickness of the edges of the defect are the most important ones.^7^ In our centre, both angiography and TEE were used. Notably, TEE emerged as superior in measuring the defect size, as evidenced by the unexpected discovery of an oval-shaped VSD with diameters of 18 × 6 mm using 3D TEE.
Generally, the selected device is 1–2 mm larger than the maximal diameter of the defect as assessed by TEE and angiography.^7^ Initial attempts with an occluder No. 12/14 were unsuccessful, leading to device dislodgment. A subsequent attempt with the same device resulted in an unstable position with a significant residual peripheral shunt. Re-evaluation of the defect size using 3D TEE prompted the use of a larger device occluder No. 16/18. However, this choice introduced the potential risk of manipulating or causing mechanical trauma to the AV node, possibly inducing AV block or bundle branch block.^8^ After careful consideration of risks and benefits, we proceeded with the procedure, preparing for a transcutaneous pacemaker. The intervention proved successful, with a stable device position, no residual shunt, or complications. A follow-up six months later revealed the patient without complaints and good outcomes, without any delayed complication.
This case underscores the significance of a good and accurate evaluation of a defect before and during a procedure with echocardiography, particularly 3D TEE. Transoesophageal echocardiography holds the most important role in the success of this simple yet complex procedure of transcatheter closure of large oval-shaped perimembranous VSD. While 3D TEE has been widely used in assisting transcatheter ASD closure, its role in percutaneous VSD closure has yet to be fully explored. Balloon sizing is hardly ever used since the interventricular septum is regarded to be a non-stretchable structure.^9^ This case also showed the lack of knowledge on the closure of an oval-shaped VSD. Studies or reports on oval-shaped VSDs are limited, and there is no specific recommendation or guideline on the closure of this type of defect. Therefore, further studies are required for the establishment of recommendations on transcatheter oval shape VSD closure as well as the device selection for this specific defect.
Conclusion
This study brings attention to the rarity of large oval VSD that posed a significant challenge for closure using conventional measurements with echocardiography and fluoroscopy. The successful outcome was achieved through a comprehensive evaluation of the size and shape of the oval VSD using 3D TEE. This highlights the potential superiority of 3D TEE over fluoroscopy in determining the appropriate device size, particularly in unconventional cases such as oval-shaped VSDs. The findings underscore the evolving role of advanced imaging modalities in enhancing the precision and success of transcatheter closure procedures for complex cardiac defects.
Supplementary Material
ytae170_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shaddy RE, Penny DJ, Feltes TF, Cetta F, et al Moss and Adams’ heart disease in infants, children and adolescents including the fetus and young adult. 10th ed. Philadelphia: Wolters Kluwer; 20221.
- 2Bride P, Kaestner M, Radermacher M, Vitanova K, von Scheidt F, Scharnbeck D, et al Spontaneous closure of perimembranous ventricular septal defects: a janus-faced condition. CASE (Phila) 2020;4:103–105. 10.1016/j.case.2019.08.005.32337401 PMC 7175755 · doi ↗ · pubmed ↗
- 3Haddad RN, Daou L, Saliba Z. Device closure of perimembranous ventricular septal defect: choosing between Amplatzer occluders. Front Pediatr 2019;7:300. 10.3389/fped.2019.00300.31475122 PMC 6707042 · doi ↗ · pubmed ↗
- 4Behzad A . Transcatheter closure of congenital VS Ds: tips and tricks. In: Burak P (ed.), Angiography. Rijeka: Intech Open; 2019. p Ch. 7. 10.5772/intechopen.83641. · doi ↗
- 5Aal AA, Hassan HM, Ezzeldin D, El Sayed M. Impact of percutaneous ventricular septal defect closure on left ventricular remodeling and function. Egypt Heart J 2021;73:86. 10.1186/s 43044-021-00215-z.34637037 PMC 8511205 · doi ↗ · pubmed ↗
- 6Fusco F, Borrelli N, Palma M, Sarubbi B, Scognamiglio G. Imaging of ventricular septal defect: native and post-repair. In J Cardiol Congenit Heart Dis 2022;7:100335. 10.1016/j.ijcchd.2022.100335. · doi ↗
- 7Sadeghian H, Savand-Roomi Z. Ventricular septal defect device closure. In: Sadeghian H, Savand-Roomi Z (ed.), Echocardiographic atlas of adult congenital heart disease. Cham: Springer International Publishing; 2015. p 169–170. 10.1007/978-3-319-12934-1_54. · doi ↗
- 8Chen Q, Cao H, Zhang G-C, Chen L-W, Li Q-Z, Qiu Z-H. Atrioventricular block of intraoperative device closure perimembranous ventricular septal defects; a serious complication. BMC Cardiovasc Disord 2012;12:21. 10.1186/1471-2261-12-21.22458934 PMC 3337292 · doi ↗ · pubmed ↗