Partial Splenic Embolization in a Patient with Hemophilia A and Severe Thrombocytopenia: A Case Report
Tomofumi Nakamura, Mitsuhiro Uchiba, Hirotomo Nakata, Takao Mizumoto, Toru Beppu, Shuzo Matsushita

TL;DR
A patient with hemophilia A and severe low platelet count successfully underwent a minimally invasive procedure to improve his quality of life.
Contribution
This case report demonstrates the effectiveness of partial splenic embolization in managing thrombocytopenia in a hemophilia A patient with multiple viral infections.
Findings
Partial splenic embolization increased platelet counts and improved quality of life in a hemophilia A patient.
The procedure allowed the patient to safely undergo HCV treatment without serious complications.
Long-term stability was achieved without major infections or platelet count relapses.
Abstract
We report a patient with hemophilia A who underwent partial splenic embolization (PSE) for severe thrombocytopenia secondary to portal hypertension-induced splenomegaly, resulting in a stable long-term quality of life. The patient was diagnosed with hemophilia A and unfortunately contracted human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV) from blood products. He subsequently developed progressive splenomegaly due to portal hypertension from chronic HCV, resulting in severe thrombocytopenia. PSE was performed because he had occasional subcutaneous bleeding and needed to start interferon (IFN) and ribavirin (RBV) treatment for curing his HCV infection at that time. His platelet counts increased, and no serious adverse events were observed. Currently, he continues to receive outpatient treatment, regular factor VIII (FVIII) replacement therapy for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
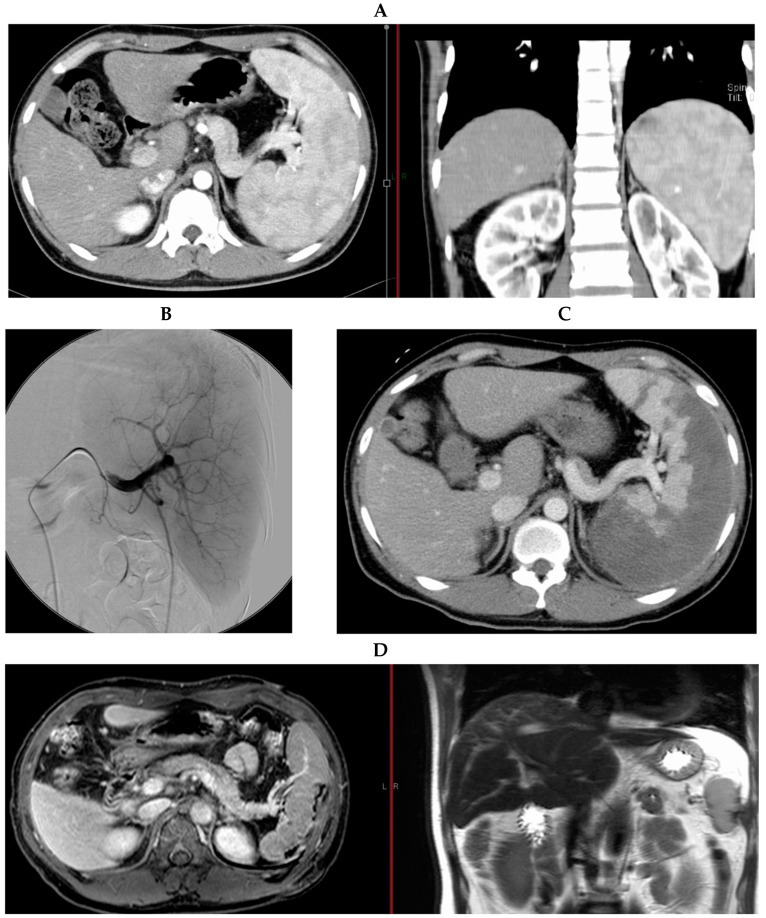 Figure 1
Figure 1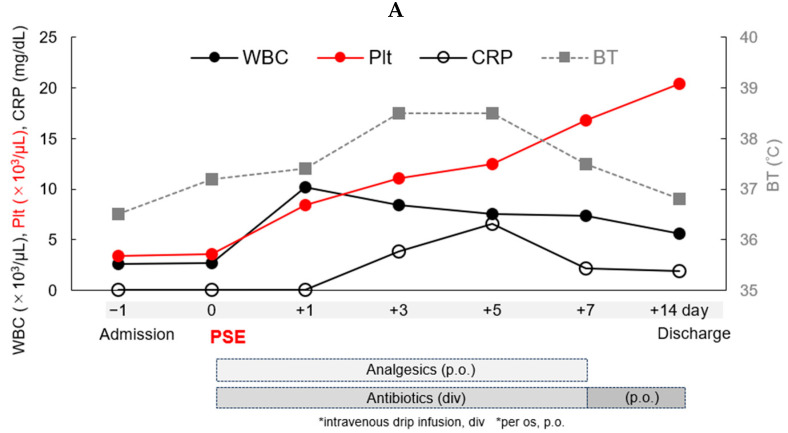 Figure 2
Figure 2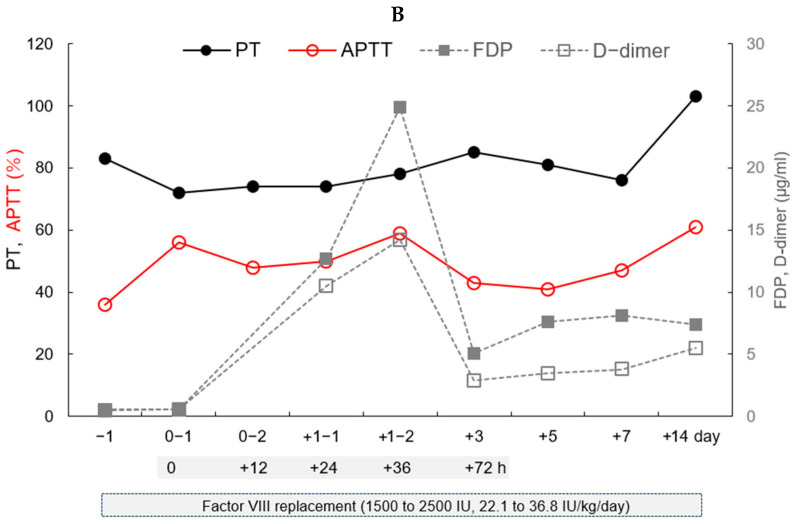 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransportation Planning and Optimization · Traffic Prediction and Management Techniques · Vehicle emissions and performance
1. Introduction
Hemophilia A (classical hemophilia) is an inherited bleeding disorder caused by a congenital deficiency or lack of coagulation factor VIII (FVIII) [1]. FVIII plays an important role in the coagulation process to control bleeding. Hemophilia A is an X-linked recessive genetic disorder that primarily affects males; however, female carriers of the gene may also be symptomatic [2]. In recent years, the development of several improved coagulation factor products has made it easier to control the coagulation process in patients with hemophilia A, and the quality of life for these patients has improved dramatically [3,4]. Nevertheless, hemostatic management of patients with hemophilia A who have traumatic bleeding injuries or undergo major surgery requires monitoring and adequate coagulation factor replacement. In addition, patients with hemophilia A need to receive care and support, including bleeding control and a recovery plan prepared by a medical team, including hematology specialists. The patient in this case study underwent partial splenic embolization (PSE), which has been developed as a minimally invasive treatment to avoid side effects such as severe abdominal pain, fevers, bacterial infections, and splenic abscesses.
Here, we present a male patient in his 40s who receives outpatient treatment for hemophilia A and human immunodeficiency virus (HIV) infection. He underwent PSE for severe thrombocytopenia caused by portal hypertension-induced splenomegaly due to chronic hepatitis C virus (HCV) infection when he was in his 20s [5]. To our knowledge, only one other partial case report of a patient with hemophilia A treated with PSE has been reported [6].
2. Case Report
At present, a male patient in his 40s is an outpatient at our hospital for the treatment of hemophilia A with efraloctocog alfa (Eloctate^®^, Biogen, Cambridge, MA, USA), and HIV infection with maraviroc (Celsentri^®^, Tokyo, Japan), lamivudine (Epivir^®^, ViiV Healthcare, Brentford, UK), and darunavir/cobicistat (Prezcobix^®^, Johnson & Johnson Innovative Medicine, Beerse, Belgium). When he was a child, his hemophilia A was classified as severe. He has received several types of recombinant FVIII replacement therapy for more than 20 years, depending on his bleeding symptoms and FVIII trough and peak levels. Now, efraloctocog alfa (30 IU/kg, two or three times per week) is being administered, resulting in the estimated 72 h trough and peak values of 2.6% and 71%, respectively. FVIII inhibitors are never detected. He unfortunately contracted hepatitis B (HBV), HCV, and HIV infections from blood products in the 1980s. He had severe thrombocytopenia that progressed (Table 1); occasional subcutaneous bleeding occurred despite adequate FVIII replacement therapy. Splenomegaly (Figure 1A) secondary to portal hypertension from chronic HCV was suspected as the cause of his severe thrombocytopenia and subcutaneous bleeding. Additionally, he needed to be treated with interferon (IFN) and ribavirin (RBV) to cure his HCV infection at that time.
When the patient was in his 20s, considering the risk of bleeding and neutralizing anti-FVIII antibodies induced by the high-dose administration of recombinant FVIII through invasive splenectomy, he underwent PSE in our hospital for management of his thrombocytopenia and subcutaneous bleeding, and initiation of IFN and RBV treatment for curing his HCV infection. No secondary abnormal findings such as esophageal/gastric varices secondary to portal hypertension were found on preoperative examination. A catheter was inserted into the femoral artery, and angiography was performed to visualize the splenic artery and segment for PSE (Figure 1B). Embolization of the splenic artery was performed, and a gelatin sponge was placed to slow the blood flow to prevent acute side effects.
After the procedure, contrast-enhanced computerized tomography (CT) confirmed that the splenic embolization area was approximately 90% (Figure 1C). His clinical course during hospitalization is shown in Figure 2. Administration of antibiotics and analgesics was begun post PSE, and left hypochondriac pain and a fever of approximately 38 °C appeared post PSE from Day 0. After Day 7, his pain, fever, and laboratory data gradually improved (Figure 2A). To achieve adequate hemostasis and per hemophilia management guidelines [7], 1500 to 2500 IU (22.1 to 36.8 IU/kg) of recombinant FVIII, Recombinate, was administered daily during hospitalization. His coagulation status was readily monitored through the activated partial thromboplastin time (APTT) instead of through FVIII activity because we did not see FVIII activity immediately, and other data such as the thrombin time (PT), fibrinogen degradation products (FDPs), and D-dimer levels were also monitored during hospitalization (Figure 2B). Post PSE, his platelet count increased from 4.0 × 10^4^ on Day 0 to 2.0 × 10^5^ /µL on Day 14. FDP and D-dimer levels were highest 36 h post PSE at 24.9 and 14.2 μg/mL, respectively, and decreased by 72 h. Slightly elevated levels of FDPs and D-dimer continued until Day 14. The patient showed no signs of inadequate splenic artery embolization, acute infection, or bleeding from the embolized spleen. The patient was discharged from the hospital in a stable condition on Day 14. No neutralizing anti-FVIII antibodies induced by the higher dose of continuous recombinant FVIII replacement were detected after the PSE.
Several months later, the patient started IFN and RBV treatment for his HCV infection and subsequently achieved a sustained virologic response. Magnetic resonance imaging (MRI) performed 5 years post PSE (Figure 1D) showed no liver tumor, and the spleen was normal in size. Currently, the patient receives regular treatments at our hospital for his hemophilia A and HIV infection and has experienced no serious side effects or deterioration in his quality of life.
3. Discussion
The patient’s HIV infection has been under control since the introduction of highly active antiretroviral therapy (HAART). However, we suspected that he had splenomegaly due to chronic HCV infection but without a cirrhotic pattern of fibrosis. The main cause of portal hypertension is cirrhosis of the liver [8], which accounts for approximately 80% of cases. Some cases of cirrhosis caused by HBV and HCV can be controlled with antiviral drugs. Peg-IFN and RBV treatment for curing his HCV also increased his sustained virologic response (SVR). Unfortunately, his splenomegaly progressed, leading to thrombocytopenia and subcutaneous bleeding despite adequate FVIII replacement therapy. Therefore, we opted for the minimally invasive treatment of PSE for his splenomegaly instead of a splenectomy.
PSE has attracted attention as a minimally invasive treatment to improve hypersplenism caused by portal hypertension; it may also preserve some of the important splenic functions compared to total splenectomy. This method was first reported by Maddison [9] in 1973 as total splenic embolization in patients with ruptured esophageal varices who were difficult to treat with other conservative methods. In 1979, Spigos et al. [10] reported on the safety of partial splenic embolization combined with prophylactic administration of antibiotics, which resulted in a sharp decrease in serious complications. PSE was considered to be a safe and reliable treatment method suitable for complications related to portal hypertension-induced splenomegaly. Moreover, a technique called the Takatsuka method [11] has also been reported, in which an estimated embolization rate can be calculated by embolizing the spleen in each of five subregions; with this method, thrombosis of the splenic terminal artery can be delayed until embolization by using an expandable metal coil as an embolization material. In 2014, Shimizu et al. reported that this method of PSE enabled the induction of regular-dose IFN therapy in patients without hemophilia A who had HCV cirrhosis [12]. Risk factors or therapeutic factors of PSE for thrombocytopenia in patients with cirrhosis have also been reported [13].
Patients with hemophilia in the era of inadequate factor VIII replacement therapy have problems with hemarthrosis, and vascular embolization of the joints in these patients has been frequently reported. As shown in Table 2, effective and minimally invasive treatments for patients with hemophilia also include vascular embolization for acute bleeding (spontaneous, postoperative, and traumatic), preoperative embolization for pseudotumors, and the efficacy of prostatic artery embolization for enlarged prostate [14,15,16,17,18,19,20,21,22].
When monitoring the coagulation status of the patient receiving FVIII replacement therapy after this PSE, the FDP and D-dimer levels decreased by 72 h without serious conditions such as disseminated intravascular coagulation. The patient showed no evidence of acute bacterial infection, bleeding from the necrotic spleen, or neutralizing anti-FVIII antibodies. These results suggest that patients with hemophilia A can safely undergo PSE with adequate FVIII replacement and administration of antibiotics.
In 2002, the British Committee for Standards in Haematology reported the uptake of guidelines for the prevention and treatment of infections in patients with an absent or dysfunctional spleen [23]. However, vaccines against encapsulated organisms such as pneumococcus, Haemophilus influenzae, and meningococcus were rarely administered in one survey of post-splenectomy patients in Japan [24], where guidelines existed only for splenectomies in patients with immune thrombocytopenia at the time. Our case study’s patient has not been vaccinated. His spleen is of a normal size, there are no Howell–Jolly bodies in his peripheral blood to suggest asplenia or hyposplenia [25], and his CD4 T cell count is normal, but we consider that these vaccines should be recommended.
4. Conclusions
Here, we first report in detail the general condition and coagulation status of a patient with hemophilia A who underwent PSE. PSE should be a useful minimally invasive treatment for patients with hemophilia for the management of complications associated with splenomegaly or thrombocytopenia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Berntorp E. Fischer K. Hart D.P. Mancuso M.E. Stephensen D. Shapiro A.D. Blanchette V. Haemophilia Nat. Rev. Dis. Primers 202174510.1038/s 41572-021-00278-x 34168126 · doi ↗ · pubmed ↗
- 2Bryant P. Boukouvala A. Mc Daniel J. Nance D. Hemophilia A in females: Considerations for clinical management Acta Haematol.202014328929410.1159/00050388931825922 · doi ↗ · pubmed ↗
- 3Marchesini E. Morfini M. Valentino L. Recent advances in the treatment of hemophilia: A review Biologics 20211522123510.2147/BTT.S 25258034163136 PMC 8214539 · doi ↗ · pubmed ↗
- 4Mannucci P.M. Hemophilia therapy: The future has begun Haematologica 202010554555310.3324/haematol.2019.23213232060150 PMC 7049365 · doi ↗ · pubmed ↗
- 5Hayashi H. Beppu T. Shirabe K. Maehara Y. Baba H. Management of thrombocytopenia due to liver cirrhosis: A review World J. Gastroenterol.2014202595260510.3748/wjg.v 20.i 10.259524627595 PMC 3949268 · doi ↗ · pubmed ↗
- 6Ahire D.S. Partial splenic artery embolization therapy in hemophilia A with decompensated cld causing hypersplenism: Caution to hepatologists-a case report J. Clin. Exp. Hepatol.20188 S 133S 13410.1016/j.jceh.2018.06.520 · doi ↗
- 7Bolton-Maggs P.H. Perry D.J. Chalmers E.A. Parapia L.A. Wilde J.T. Williams M.D. Collins P.W. Kitchen S. Dolan G. Mumford A.D. The rare coagulation disorders-review with guidelines for management from the United Kingdom Haemophilia Centre Doctors’ Organisation Haemophilia 20041059362810.1111/j.1365-2516.2004.00944.x 15357789 · doi ↗ · pubmed ↗
- 8Ginès P. Krag A. Abraldes J.G. SolàE. Fabrellas N. Kamath P.S. Liver cirrhosis Lancet 20213981359137610.1016/S 0140-6736(21)01374-X 34543610 · doi ↗ · pubmed ↗