Assessing and Improving the Care of Patients With Heart Failure in Ghana: Protocol for a Prospective Observational Study and the Ghana Heart Initiative-Heart Failure Registry
Felix Awindaogo, Emmanuel Acheamfour-Akowuah, Alfred Doku, Collins Kokuro, Francis Agyekum, Isaac Kofi Owusu

TL;DR
This study aims to improve heart failure care in Ghana by collecting data on patient outcomes and treatment patterns.
Contribution
The study introduces a prospective observational study and registry to assess heart failure in Ghana, where data is currently scarce.
Findings
The study will collect data on heart failure epidemiology and treatment outcomes from 5000 patients across nine hospitals.
Results will inform future heart failure prevention and management strategies in Ghana.
Abstract
Heart failure (HF) is a leading cause of morbidity and mortality globally, with a high disease burden. The prevalence of HF in Ghana is increasing rapidly, but epidemiological profiles, treatment patterns, and survival data are scarce. The national capacity to diagnose and manage HF appropriately is also limited. To address the growing epidemic of HF, it is crucial to recognize the epidemiological characteristics and medium-term outcomes of HF in Ghana and improve the capability to identify and manage HF promptly and effectively at all levels of care. This study aims to determine the epidemiological characteristics and medium-term HF outcomes in Ghana. We conducted a prospective, multicenter, multilevel cross-sectional observational study of patients with HF from January to December 2023. Approximately 5000 patients presenting with HF to 9 hospitals, including teaching, regional, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
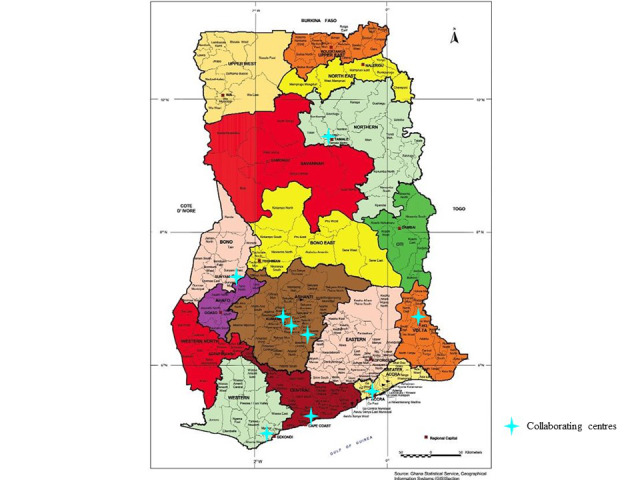 Figure 1
Figure 1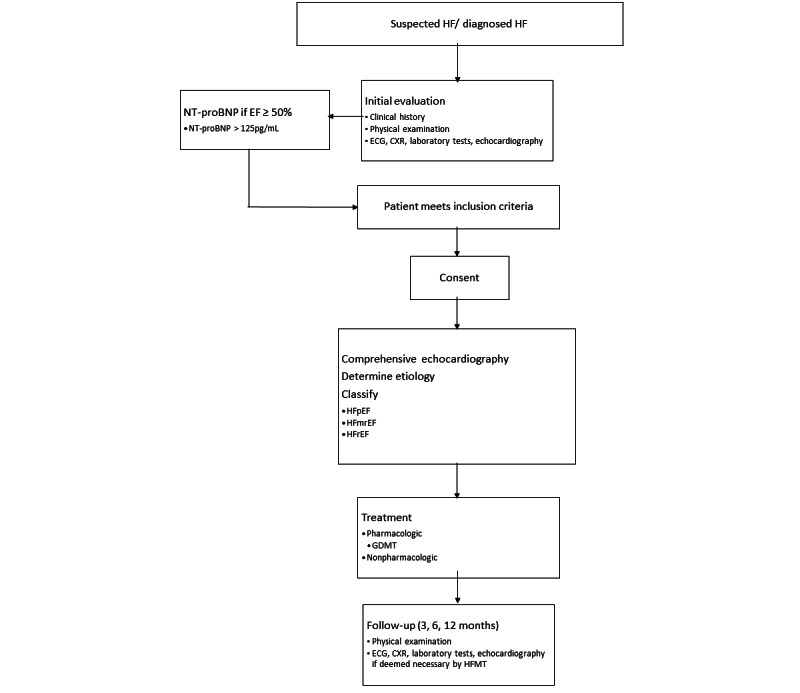 Figure 2
Figure 2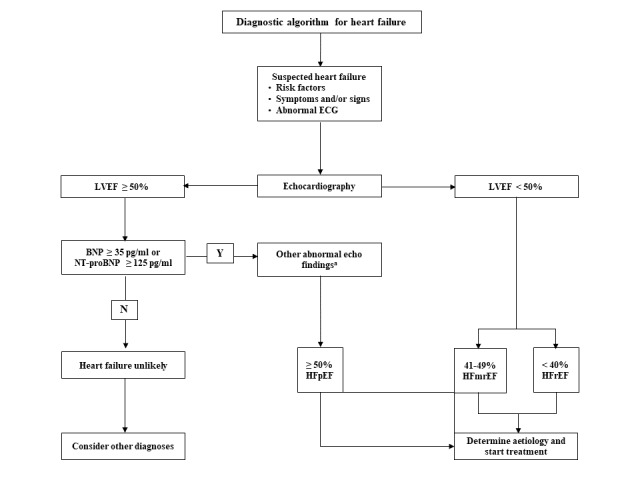 Figure 3
Figure 3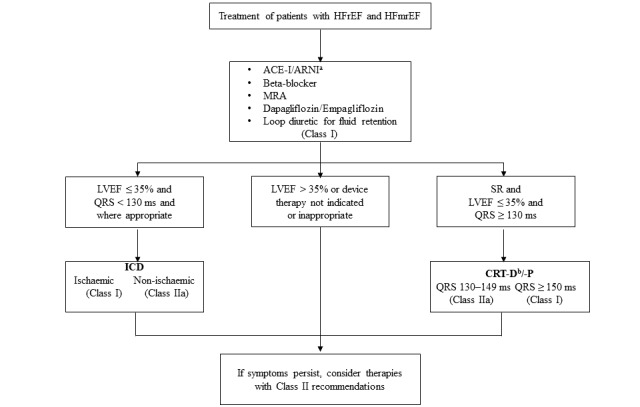 Figure 4
Figure 4| Etiology of HF | Clinical characteristics | Specific investigations |
| Hypertension [ |
Persistent elevated systolic BPa ≥140 mm Hg and diastolic BP ≥90 mm Hg Presence of HMODb Current or previous use of antihypertensive medications |
24-hour ambulatory BP Plasma metanephrines and renal artery imaging Serum renin and aldosterone TTEc |
| Coronary artery disease [ |
HF and ACSd A pre-existing history of CCSe Features suggestive of significant CADf on coronary angiography or other imaging |
Invasive coronary angiography CTg coronary angiography Imaging stress tests (echo, nuclear, and CMRh) |
| Valvular heart disease [ |
Primary valve disease, for example, aortic stenosis Secondary valve disease, for example, functional regurgitation Congenital valve disease, for example, bicuspid aortic valve and mitral valve prolapse |
TTE/ TEEi/ stress echo CT/ CMR |
| Rheumatic heart disease [ |
Primary valve disease, for example, mitral stenosis and mitral regurgitation Atrial fibrillation |
TTE/ TEE/ stress echo |
| Dilated cardiomyopathy [ |
Unexplained dilated cardiac chambers with increased left ventricular mass index |
CMR, genetic testing Trace elements, toxicology, LFTsj |
| Arrhythmia-induced cardiomyopathy [ |
Mean heart rate above 100 beats per minute Atrial fibrillation Premature ventricular contractions burden equal to or greater than 10% No other cause of LV dysfunction identified |
Ambulatory ECG recording Electrophysiology study, if indicated |
| Congenital heart disease |
History of congenital heart disease Incidental diagnosis of congenital heart disease during investigation for HF |
TTE/ TEE CMR |
| Other etiologies of HF [ |
Clinical features diagnostic of restrictive cardiomyopathy, arrhythmogenic cardiomyopathy, peripartum cardiomyopathy, endomyocardial fibrosis, cor pulmonale, infiltrative cardiomyopathy, pericardial disease, LV noncompaction cardiomyopathy, and toxin-induced cardiomyopathy. |
Serum electrophoresis and serum free light chains. Echo, CMR, CT-PETk, endomyocardial biopsy, Serum angiotensin-converting enzyme, fluorodeoxyglucose-PET, and chest CT Right and left heart catheterization |
|
| 2022 | 2023 | 2024 | |||||||||||||
|
| December | January | February | March | April | May | June | July | August | September | October | November | December | January-June | June | |
| Training for KBTH and KATH | ✓ |
|
|
|
|
| ✓ |
|
|
|
|
|
|
|
| |
| Training for other sites |
|
|
|
|
|
|
| ✓ |
|
| ✓ |
|
|
|
| |
| Sensitization workshops for KBTH and KATH | ✓ |
|
|
|
| ✓ |
|
|
|
|
|
|
|
|
| |
| Sensitization workshops for other sites |
|
|
|
|
|
|
| ✓ |
|
| ✓ |
|
|
|
| |
| Enrollment and data collection |
| ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
|
| |
| Establishment of HF clinics |
| ✓ |
|
|
|
|
| ✓ |
|
|
|
|
|
|
| |
| Follow-up |
|
|
| ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| |
| Preliminary data analysis and reporting |
|
|
|
|
|
|
|
|
| ✓ |
|
|
|
|
| |
| End of enrollment |
|
|
|
|
|
|
|
|
|
|
|
|
| ✓ |
| |
| Data analysis |
|
|
|
|
|
|
|
| ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| |
| End of study |
|
|
|
|
|
|
|
|
|
|
|
|
|
| ✓ | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHeart Failure Treatment and Management · Congenital Heart Disease Studies · Cardiovascular Function and Risk Factors
Introduction
Overview
Heart failure (HF) is a costly, multifaceted, and life-threatening syndrome characterized by significant morbidity and mortality. Globally, HF affects 64 million people, with a prevalence of 1%-2% of adults in the general population and an estimated incidence of 1-20 cases per 1000 person-years [1].
Sub-Saharan Africa (SSA) has no population-based data; however, in-hospital prevalence ranges from 9.4% to 42.5% [2,3]. HF in SSA mainly affects young people and middle-aged individuals, occurring in people aged between 36 and 62.4 years [4]. It poses a substantial disease burden, with high mortality, rehospitalization rates, and health care costs, primarily attributable to readmissions and prolonged hospitalization periods of 11-13 days [3,5,6].
HF contributes significantly to Ghana’s cardiovascular disease burden, with a worse prognosis and a more malignant course [7,8]. It is a leading cause of death among Ghanaian adults; yet, there is a paucity of data on the epidemiological profiles, treatment patterns, and survival rates of patients with HF in Ghana [9-11]. Single-center studies indicate a high prevalence of HF in Ghana [7,8,12].
The diagnosis of HF in most patients is primarily based on clinical manifestations due to the limited availability of diagnostic equipment. Ghana has few cardiologists, who are mainly located in tertiary hospitals [13]. In addition, there is a lack of HF education and training for physicians and nonphysician health workers. While HF management teams or multidisciplinary teams for HF management are the gold standard model for the delivery of care, these teams are nonexistent in Ghana, and most health facilities lack resources for long-term patient follow-up, such as diagnostic equipment, dedicated HF clinics, and protocols [14-17].
A national network of heart failure management teams (NNHFMT) will be established as part of the Ghana Heart Initiative’s efforts to improve cardiovascular disease care in Ghana to help mitigate the burden of HF. The NNHFMT is tasked with building the capacity of both secondary and tertiary levels of care to promptly and effectively identify and manage HF by creating heart failure management teams (HFMTs) and establishing a national registry for HF and HF clinics that will be integrated with routine clinical services to provide long-term follow-up and care. The establishment of HF clinics and a national registry will fill a significant gap in HF care and research by providing the most recent epidemiological, management patterns, and medium-term outcomes data on HF.
Objectives
The primary objective of this study is to determine the epidemiological characteristics and medium-term outcomes of HF in Ghana by outlining the epidemiological and clinical characteristics of patients with HF in Ghana, identifying the underlying causes, evaluating the medium-term outcomes of HF in Ghana, and identifying the factors that predict hospitalization and mortality in patients with HF in Ghana. This study also aims to build capacity in the care of patients with HF and form the basis for a national registry for HF in Ghana.
Methods
Overview
An NNHFMT consisting of physicians, nurses, and researchers from 9 collaborating hospitals in Ghana was constituted to achieve the study objectives, with each institutional HFMT led by a cardiologist, 2 supporting cardiologists or physicians, and 2 nurses. The HFMTs will establish HF clinics and integrate them into the routine services of their hospitals; recruit patients with HF and manage them per guidelines and algorithm; and create awareness and train other personnel in the 9 centers on the diagnosis and management of HF. These institutions include 5 teaching hospitals, 3 regional hospitals, and 1 municipal hospital. They include the Korle-Bu Teaching Hospital (KBTH), Komfo Anokye Teaching Hospital (KATH), Tamale Teaching Hospital (TTH), Ho Teaching Hospital (HTH), Cape Coast Teaching Hospital (CCTH), Bono Regional Hospital, Presbyterian Hospital-Agogo, Kumasi South Hospital, and the Effia Nkwanta Regional Hospital (Figure 1) [18].
Map of Ghana showing the location of collaborating centers. Source: Ghana Statistical Service, 2020.
Study Design
This is a prospective, multicenter, and multilevel observational study of patients with HF. Patients presenting with HF will be recruited and evaluated according to a standardized protocol. Guideline-directed treatment for HF will then be prescribed after the diagnosis has been confirmed. The study will conduct a serum N-terminal pro-brain natriuretic peptide (NT-proBNP) and transthoracic echocardiogram for all participants for free, while the cost of treatment and other investigations will be borne by study participants as in routine care. Patients will be followed up prospectively for 6 months to determine the medium-term outcomes of interventions (Figure 2).
Patients will be recruited through the collaborating institutions’ emergency rooms, admission wards, and established HF clinics from January to December 2023. The HFMTs of the 2 leading teaching hospitals in Ghana, KBTH and KATH, will be trained using a facilitators’ training manual, which will be developed from current international HF guidelines. KBTH and KATH will then provide mentorship and training to the other collaborating hospitals. The HFMT of KBTH will train members of the HFMTs from the TTH, HTH, and Effia-Nkwanta Regional Hospital, while the HFMT of KATH will also train the HFMTs of CCTH, Bono Regional Hospital, Presbyterian Hospital-Agogo, and Kumasi South Hospital. The study will begin in the KBTH and KATH in January 2023, while the other 7 sites will begin recruitment in July 2023, and all areas will end enrollment in December 2023.
Chart outlining study design.
Study Population
Study participants will include patients aged 13 years or older who present with HF in the collaborating hospitals and consent to participate in the study. Patients with a life expectancy less than the expected duration of the registry due to non-HF comorbidities will be excluded.
Based on our estimation of a sample size of 5000 participants, we would be able to determine the mortality and hospitalization rate at 6 months with a 95% CI and a precision of ±1%. Each participating center will recruit 556 participants.
Recruitment of Study Participants
Participants will be recruited through the various departments or units of the collaborating institutions. All patients diagnosed with HF or suspected of having HF will be referred to the HFMTs for evaluation and enrollment. A total of 2 sensitization workshops will be organized at collaborating institutions during the study period: 1 before participants’ enrollment and 1 midway through participant recruitment.
Data Collection
Data collection comprises administering questionnaires, reviewing medical records, physical examinations, imaging investigations, including chest x-rays and echocardiography, electrocardiography, and laboratory tests. The methods for data collection in this study are identical in all locations, following standardized operating manuals and tools.
Diagnosis of HF
The diagnosis of HF will be made using a modified diagnostic algorithm adopted from the 2021 European Society of Cardiology Guidelines to diagnose and treat acute and chronic HF (Figure 3) [19]. The diagnosis of HF will be made based on the presence of typical symptoms of HF and objective evidence of cardiac dysfunction and categorized into three phenotypes: (1) heart failure with reduced ejection fraction (HFrEF), (2) heart failure with mildly reduced ejection fraction (HFmrEF), and (3) heart failure with preserved ejection fraction (HFpEF) based on the left ventricular ejection fraction (LVEF) [19].
All patients with typical symptoms and specific signs of HF and LVEF≤40% will be categorized as HFrEF, while patients with LVEF of 41%-49 % will be categorized as HFmrEF.
HFpEF will be diagnosed in patients presenting with typical symptoms and specific signs of HF and LVEF≥50%, the presence of elevated natriuretic peptides (NT-proBNP≥125 pg/mL), and objective evidence of cardiac structural and functional abnormalities consistent with the presence of left ventricular (LV) diastolic dysfunction or raised LV filling pressures. Objective evidence of structural or functional abnormalities includes the following:
LV mass index ≥95 g/m^2^ (female), ≥115 g/m^2^ (male), and a relative wall thickness >0.42.Left atrial volume index >34 mL/m^2^ in sinus rhythm (SR) and the presence of atrial fibrillation (AF) left atrial volume >40 mL/m^2^.E/e’ ratio at rest >9.NT-proBNP >125 (SR) or >365 (AF) pg/mL OR BNP >35 (SR) or >105 (AF) pg/mL.Pulmonary artery systolic pressure >35 mm Hg or tricuspid regurgitant velocity at rest >2.8 m/second.
Modified diagnostic algorithm for heart failure (HF). BNP: brain natriuretic peptide; ECG: electrocardiogram; HFmrEF: heart failure with mildly reduced ejection fraction; HFpEF: heart failure with preserved ejection fraction; HFrEF: heart failure with reduced ejection fraction; LVEF: left ventricular ejection fraction.
Etiology of HF
The etiology of HF will be determined based on the history, physical examination, laboratory, electrocardiographic, echocardiographic findings, and other imaging modalities (Table 1).
Treatment of HF
A modified treatment algorithm adopted from the 2021 European Society of Cardiology Guidelines for treating acute and chronic HF (Figure 4) will be used in the treatment of patients [19].
Modified treatment algorithm for treating HFrEF and HFmrEF. a: a replacement for ACE-I/ARB (angiotensin receptor blocker); ACE-I: angiotensin-converting enzyme inhibitor; ARNI: angiotensin receptor-neprilysin inhibitor; CRT-D: cardiac resynchronisation therapy with a defibrillator; CRT-P: cardiac resynchronisation therapy pacemaker; HFmrEF: heart failure with mildly reduced ejection fraction; HFrEF: heart failure with reduced ejection fraction; ICD: implantable cardioverter-defibrillator; MRA: mineralocorticoid receptor antagonist; ms: milliseconds; SR: sinus rhythm.
Data Handling and Analysis
The KoboCollect toolbox (v2022.4.4; [30]) will be used to capture data and upload it onto a cloud database that is only accessible to the principal investigator and the data manager. Collated data will be exported into SPSS (package 2016; SPSS Inc) for statistical analysis. Tables, bar charts, and pie charts will be used to present the data. For continuous variables, the central tendency and spread measures will be calculated using the mean (SD), and IQR. Categorical variables will be reported as numbers and percentages. Multivariable regression models will be used explore the relationships between variables and rehospitalization and death. We will perform a Kaplan-Meier analysis to estimate the survival and death rate of patients with HF. The Cox regression analysis will determine the relationship between the risk of death in an individual and selected variables and the significance of these variables. Missing values will be handled based on the type and frequency of missing values. A P value <.05 will be considered statistically significant.
Timelines
The table of timelines (Table 2) below summarizes the key activities of the study from the start to the end of the study.
Ethical Considerations
Ethical approval has been obtained from the Ethical and Institutional Review Boards of Korle-Bu Teaching Hospital (STC/IRB/000150/2022), Cape Coast Teaching Hospital (CCTHERC/EC/2023/019), Tamale Teaching Hospital (TTH/R&D/SR/229), Ho Teaching Hospital (HTH-REC (30) FC_2023), and Komfo Anokye Teaching Hospital (KATH IRB/AP/166/22). All participants will be informed about the study, its objectives, and the data collection methods. Consent will be obtained from participants who agree to be part of the study and are assured of strict confidentiality and anonymity. Participants will also be informed that participation in the study is entirely voluntary, and all the services they receive at the clinic will continue as usual whether they decide to participate or not. A unique study number will be assigned to each participant, and the collected data will be deidentified. Only the assigned unique number will be used on study documents related to participants. Participants will also be informed that they can withdraw from the study at any time they choose without consequences.
Results
This intervention will generate the necessary information on the etiology of HF, clinical presentations, the diagnostic yield of various tools, and management outcomes. In addition, it will build the necessary capacity and support for HF management in Ghana. As of July 30, 2023, the training of the various health workers in all 9 hospitals has been completed. The KATH and the KBTH acted as supervisory sites and supported the training at 4 and 3 sites, respectively. Preliminary analyses will be conducted by the end of the second quarter of 2024, and results are expected to be publicly available by the middle of 2024.
The test-run of the research and registry instruments and modifications have been completed. Medical equipment (echocardiogram machines and NT-proBNP devices) has been calibrated and distributed to all sites.
Discussion
Overview
HF is one of the leading causes of hospital admissions in developing countries and is predicted to experience the most rapid growth worldwide [2,7,31,32]. This prospective study will answer many clinical questions about HF in Ghana. First, this study will address a notable data scarcity in HF care and research in Ghana by establishing a national HF registry, thus creating a vehicle for the accrual of large, comprehensive, and contemporary data encompassing the sociodemographic, clinical profiles, causes of HF, management of HF, and determinants of outcomes such as mortality and hospitalizations of patients with HF in Ghana. In addition, a national HF registry will also provide a good opportunity to evaluate adherence to current guidelines and response to treatment among patients with HF in Ghana.
Clinical registries play a crucial role in gathering real-world data, essential for developing evidence for best clinical practice, measuring outcomes, providing feedback to clinicians, and enhancing the quality of care [1,33]. HF registries, like the Swedish Heart Failure Registry, have played a significant role in advancing knowledge and improving the management of HF. Established in 2000 and implemented nationwide in Sweden by 2003, this registry has yielded valuable research outcomes that have led to notable improvements in the understanding and care of patients with HF and under-treatment detection [1]. The NAtional TUnisian REgistry of Heart Failure (NATURE-HF) contributed valuable data that have the potential to enhance the treatment and overall prognosis of individuals with HF in North Africa [34]. Valuable data were also derived from the Abeokuta Heart Failure Clinical Registry of patients presenting with acute HF in Abeokuta, Nigeria, including acute HF presenting at a relatively younger age, commoner in men, and associated with severe symptoms [35].
While the acquisition of realistic data will address the data gap, this pragmatic study will provide capacity building for the management of HF by enhancing the skills and knowledge of health care providers in diagnosing and treating HF and making diagnostic equipment, including echocardiography, electrocardiograms, and point-of-care NT-proBNP devices, available to participating hospitals. Furthermore, participating institutions’ HFMTs and HF clinics will broaden the prospect for specialist HF care and long-term follow-up in their regions.
Although numerous HF guidelines are available to aid in managing patients with HF, their generalizability presents variable challenges, as these guidelines may not be appropriate for managing HF in countries with limited health care resources [19]. Therefore, we anticipate that this study will serve as a significant milestone in establishing a standardized approach to managing HF in Ghana and the wider SSA region.
The study will address a notable void within Ghana’s ever-evolving HF care and research domain. The study will generate novel and indispensable data that will improve HF care, serve as a foundation for teaching, develop locally tailored HF guidelines, and establish HF research programs.
Strengths and Limitations of This Study
This pragmatic, prospective, multicenter study will generate the most extensive contemporary data on HF in Ghana. The study will also enhance the knowledge and skills of health personnel in diagnosing and managing HF. The project is also designed to establish HF clinics and provide diagnostic services as part of routine health care services in participating hospitals. This study will describe associations rather than establish causality owing to its observational design.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Savarese G Becher PM Lund LH Seferovic P Rosano GMC Coats AJS Global burden of heart failure: a comprehensive and updated review of epidemiology Cardiovasc Res 20231181732723287 10.1093/cvr/cvac 01335150240652762735150240 · doi ↗ · pubmed ↗
- 2Gtif I Bouzid F Charfeddine S Abid L Kharrat N Heart failure disease: an African perspective Arch Cardiovasc Dis 202111410680690 10.1016/j.acvd.2021.07.00134563468 S 1875-2136(21)00133-934563468 · doi ↗ · pubmed ↗
- 3Ogah OS Adebiyi A Sliwa K Rescigno G Firstenberg MS Heart failure in Sub-Saharan Africa Topics in Heart Failure Management 2019 London, UK Intech Open 6199
- 4Agbor VN Essouma M Ntusi NAB Nyaga UF Bigna JJ Noubiap JJ Heart failure in sub-Saharan Africa: a contemporaneous systematic review and meta-analysis Int J Cardiol 201825720721510.1016/j.ijcard.2017.12.04829506693 S 0167-5273(17)35196-329506693 · doi ↗ · pubmed ↗
- 5Adidja NM Agbor VN Aminde JA Ngwasiri CA Ngu KB Aminde LN Non-adherence to antihypertensive pharmacotherapy in Buea, Cameroon: a cross-sectional community-based study BMC Cardiovasc Disord 2018181150 10.1186/s 12872-018-0888-z 3004160610.1186/s 12872-018-0888-z 30041606 PMC 6056997 · doi ↗ · pubmed ↗
- 6Mensah GA Roth GA Sampson UKA Moran AE Feigin VL Forouzanfar MH Naghavi M Murray CJL Mortality from cardiovascular diseases in sub-Saharan Africa, 1990-2013: a systematic analysis of data from the Global Burden of Disease Study 2013 Cardiovasc J Afr 2015262 Suppl 1S 6S 10 10.5830/CVJA-2015-0362596295025962950 PMC 4557490 · doi ↗ · pubmed ↗
- 7Appiah LT Sarfo FS Agyemang C Tweneboah HO Appiah NABA Bedu-Addo G Opare-Sem O Current trends in admissions and outcomes of cardiac diseases in Ghana Clin Cardiol 20174010783788 10.1002/clc.227532869276028692760 PMC 6490361 · doi ↗ · pubmed ↗
- 8Bonsu KO Owusu IK Buabeng KO Reidpath DD Kadirvelu A Clinical characteristics and prognosis of patients admitted for heart failure: a 5-year retrospective study of African patients Int J Cardiol 201723812813510.1016/j.ijcard.2017.03.01428318656 S 0167-5273(17)31424-928318656 · doi ↗ · pubmed ↗