Surgical smoke: a matter of hygiene, toxicology, and occupational health
Nurettin Kahramansoy

TL;DR
Surgical smoke produced during operations contains harmful particles and pathogens, posing significant health risks to medical staff and requiring better ventilation and safety measures.
Contribution
This paper highlights the composition and health risks of surgical smoke and emphasizes the need for improved hygiene and occupational safety practices.
Findings
Surgical smoke contains carcinogenic, mutagenic, and teratogenic particles, many of which bypass standard masks.
The smoke can carry viruses like SARS-CoV-2, influenza, and HIV, posing infection risks to surgical staff.
Effective smoke removal requires source-directed aspiration systems to protect the surgical team.
Abstract
The use of devices for tissue dissection and hemostasis during surgery is almost unavoidable. Electrically powered devices such as electrocautery, ultrasonic and laser units produce surgical smoke containing more than a thousand different products of combustion. These include large amounts of carcinogenic, mutagenic and potentially teratogenic noxae. The smoke contains particles that range widely in size, even as small as 0.007 µm. Most of the particles (90%) in electrocautery smoke are ≤6.27 µm in size, but surgical masks cannot filter particles smaller than 5 µm. In this situation, 95% of the smoke particles which pass through the mask reach deep into the respiratory tract and frequently cause various symptoms, such as headache, dizziness, nausea, eye and respiratory tract irritation, weakness, and abdominal pain in the acute period. The smoke can transport bacteria and viruses that…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
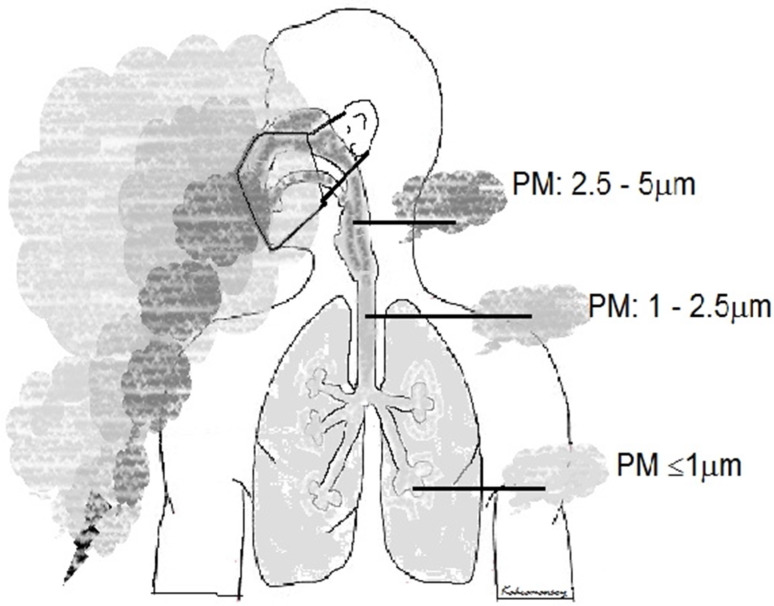 Figure 1
Figure 1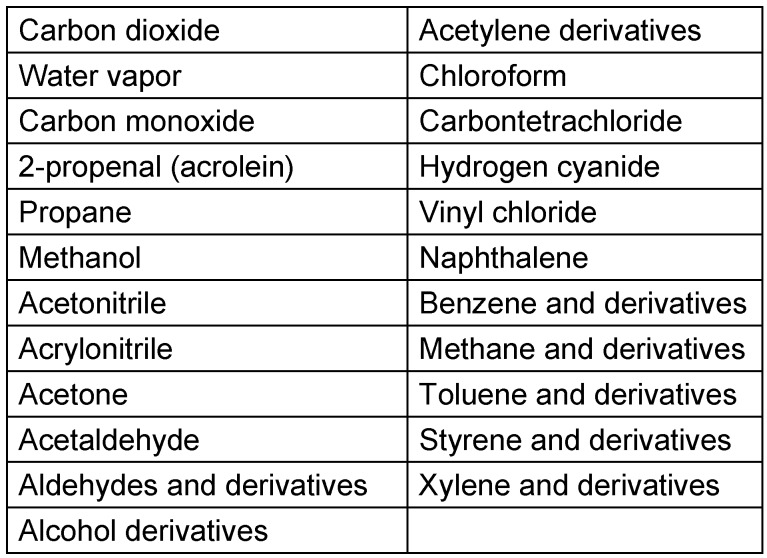 Figure 2
Figure 2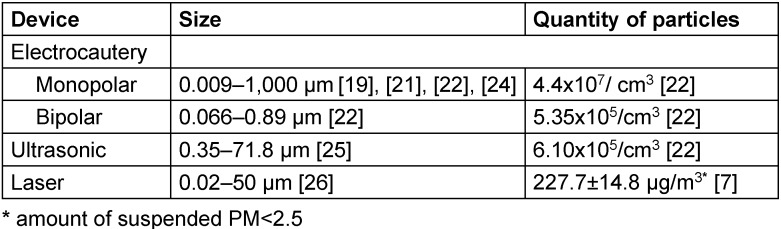 Figure 3
Figure 3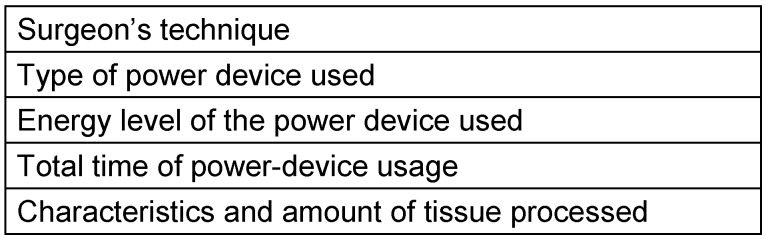 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and healthcare impacts · Infection Control and Ventilation · Climate Change and Health Impacts
Introduction
When the author of this article complained to the manager who formerly was an active surgeon that surgical smoke emitted during surgery clinically affected him, causing symptoms, the manager (inactive surgeon) replied: ‘sometimes I miss the smell of that smoke’. His lack of awareness of the danger of the smoke prompted the author to review this topic. Such lack of awareness lays the foundation for a process that can ultimately lead to various symptoms and diseases. The fact that some characteristics of surgical smoke are little-known or insufficiently understood seems to be the most important barrier to awareness. Therefore, the aim of this study was to review the current knowledge about surgical smoke.
We know that using electrically powered devices for tissue dissection and hemostasis is almost unavoidable during surgical procedures. These include electrocautery devices, ultrasonic scalpels, and laser ablation units. These devices generate by-products which are mostly termed “surgical smoke”. However, terms such as plume, aerosol and vapor are also used. The latter (vapor, aerosol and plume) are mostly preferred for larger particles suspended in the air and are produced by processes other than combustion [1], [2].
Method
The PubMed database of the US National Library of Medicine was searched for the MeSH terms ‘surgical’ and ‘smoke’, and the term ‘surgical smoke’ with other terms such as ‘plume, vapor, exposure, characteristics, particulate matter, ventilation, and operating room’. English-language literature was checked by title and abstract for eligibility according to the aim of this study. Then full texts of potentially eligible studies were assessed. A number of the most frequently cited review studies were used as a guide to the original reports. To obtain the most recent knowledge, articles published within the last five years were selected; however, earlier articles with quantitative analyses were not neglected.
Contents of surgical smoke
Chemical combustion products
Most of the substances in surgical smoke have been known for many years [1], [3], [4], [5], [6]. In the last decade, 150 types of chemical compounds were mentioned, but today 1,064 types of volatile organic compounds (VOCs) are reported. It is not difficult to foresee that this number will increase with technological development [7], [8].
The main components found in surgical smoke are CO_2_ (44.4%), water vapor (31.8%), 2-propenal (syn. acrolein; 10.7%), and propane (8.3%) (Table 1 (Tab. 1)) [9]. Some compounds (methanol, methane, ethane, ethylene, acetone, formaldehyde, 1,3-butadiene, hydrogen cyanide, benzene, methylpropene, toluene) are also detected in large quantities [6], [8], [10], [11], [12], [13], [14]. Aldehyde derivatives (e.g., formaldehyde), toluene, 1–2 dichloroethane, benzene and acrylonitrile are among the compounds of greatest concern [4], [6], [15]. Formaldehyde, benzene, and 1,3-butadiene (carcinogenic group 1), propane, ethylene (and derivates in carcinogenic groups 1 to 3), 2-propenal (acrolein), styrene, methane, and ethane (and derivates in carcinogenic group 2A), ethylbenzene, methylpropene, 1,2-dichloroethane, toluene, and acrylonitrile (carcinogenic group 2B), as well as heptane and vinyl acetylene are known not only to be carcinogenic but also mutagenic [9], [12], [13], [14], [16], [17], [18].
Particles
In addition to chemical compounds, the smoke contains cells, cell particles, erythrocytes and hemoglobin [19], [20]. The particles exist in different sizes and amounts that vary greatly depending on the method used for the tissue ablation and dissection. Most particles created by electrocautery are as small as 0.007 µm in size; while the ultrasonic scalpel leads to the formation of larger particles [3], [16], [19], [21], [22], [23], [24], [25]. The size of particles produced by the laser are detected range more widely, from very small to large sizes [7], [26]. Electrocautery also creates smaller particles in higher quantity and concentration, in addition to large particles with high total weight [23] (Table 2 (Tab. 2)). It is easy for the small particles [particulate matter (PM) <2.5 µm (PM_2.5_)] to remain suspended in the air for a time, while the suspension of PM >10 µm does not last long.
Malignant cells have been identified among the suspended particles and cells [27]. Due to their size, bacteria (2–3 µm), viruses (0.02–0.2 µm), and proteins (≤0.001 µm) can also be found suspended in surgical smoke [3], [28], [29]. Essentially, transmission of bacteria by the smoke and their infectivity have been demonstrated experimentally and clinically. For example, inoculation of the smoke into bacterial culture showed that 5 of 13 smoke samples contained coagulase-negative staphylococci [30]. In an experimental spine surgery study, bacteria were detected in 95% of swabs from a smoke sample, and one or more bacteria consistent with tissue swabs grew in 84% of these samples [31].
The presence and transport of viruses or chromosomal particles in surgical smoke has been investigated for quite some time. Viruses that have high risk of pathogenicity and are most emphasized in terms of transmission are hepatitis B virus (HBV) (0.045 µm), human papillomavirus (HPV), human immunodeficiency virus (HIV) (0.01–0.13 µm), and SARS-CoV-2 (0.125 µm) [29], [32]. HBV was detected by PCR in surgical smoke in 10 of 11 HBV-positive patients [33]. Moreover, in these cases, closed surgical methods such as laparoscopic or robotic surgery, which reduce the amount of smoke released into the environment, were used [33].
HPV DNA was detected in the surgical smoke of 2 of 7 cases treated with a CO_2_ laser [34]. The reason that HPV DNA was not detected in more smoke samples may be the long smoke-collection tube, to the interior of which the virus or its DNA probably adhere. In a study of 24 patients with high-grade squamous intraepithelial lesions of the cervix who underwent excision with loop electrocautery, the smoke contained HPV in 4 patients [35]. HPV subtype was the same in the tissue and in the smoke sample. Only in one experimental study was coronavirus RNA detected in surgical smoke proportionate to the viral load of the tissue (1/10^6^–1/10^5^), but the virus was reported to be inactive [36]. There is just one publication on HIV; it stated that HIV DNA could not be detected in the vaporous debris. However, wash culture of the tube through which the plume was transported revealed the presence of p24 HIV gag antigen at the end of the first week in 3 of the 12 samples and at the end of the 14^th^ day in 1 of the 12 samples [37]. This result indicates that the HIV virus is transported by surgical smoke.
Factors influencing surgical smoke amount and composition
The amount of smoke varies greatly, depending on many factors (Table 3 (Tab. 3)). By employing a conservative approach and technique for tissue dissection and hemostasis, the frequency of power-device use can be limited, thus limiting the amount of smoke. Table 2 (Tab. 2) shows that different power devices produce particles in different amounts and concentrations.
Electrocautery devices produce higher smoke concentrations and smaller particles, 90% of which are ≤6.27 µm in size [24]. Monopolar electrocautery devices produce the highest amount and concentration of particles [19], [21], [22], [25], [38]. The smoke concentration emitted by the monopolar device is 82 and 721 times higher than that of bipolar and ultrasonic devices, respectively [22]. The amount of particles smaller than 2.5 µm (PM <2.5) produced by monopolar electrocautery is quite high (up to 2,258 µg/m^3^) [39], [40], [41]. The average size of the particles in laser smoke is 0.07 µm, and 77% are <1.1 µm [3]. Bipolar electrocautery and ultrasonic devices produce less smoke [22], [25], [41].
Another factor affecting the amount of particles is the energy level of the device used. That is, as the energy level increases, more smoke (especially PM <2.5) is produced, and the amount of particles increases with the extension of the diathermy period [10], [26], [42], [43]. Other factors that determine the amount of smoke and particle size are the characteristics of the tissue processed. More smoke and smaller particles are generated during the dissection and hemostasis of dense tissues such as liver, kidney and muscle [9], [21], [23], [24]. These situations vary even within a tissue itself. For example, different amounts of smoke, particles and chemical compounds are released from the different tissue components (subcutaneous tissue, fat, mammary gland and breast-tumor tissues) during breast surgery [10]. The general opinion is that many factors affect the amount and content of surgical smoke; however, this is mentioned as a limitation of some studies [44].
Factors affecting the exposure of the surgical team to smoke
There are several factors – other than those limiting smoke formation – which influence the exposure of the operating-theater staff (Table 4 (Tab. 4)), as explained below.
Surgical methods
Significantly more fine (PM<2.5) and large particles are present in the smoke of open colorectal surgery compared to that of the laparoscopic method [41]. A study reports that the total amount of VOCs in the smoke produced in open surgery is slightly higher than the amount in the smoke from thoracoscopic surgery [8]. However, almost all of the selected VOCs (especially pentadiene, crotonaldehyde, g-butyrolactone) were found to be significantly higher in the smoke generated during open surgery [8]. Interestingly, higher concentrations of acetonitrile and acetaldehyde were measured during thoracoscopy [8]. Another study stated that a high amount of acetaldehyde, propionaldehyde and formaldehyde still existed in the smoke produced by laparoscopic surgery, even if the smoke was filtered. Furthermore, the amount of formaldehyde was reported to be above the determined upper limit of risk (0.016 ppm) [15]. Dense smoke (245.7 µg/m^3^) is generated during open surgery. However, if the smoke generated during laparoscopic surgery is discharged into the operating theater from the trocar valve, the smoke exits as a spray with high pressure and concentration (517.5 µg/m^3^), which actually increases the smoke exposure of the operating staff [39].
Mintz et al. [45] believed that the risk of SARS-CoV-2 transmission by smoke in laparoscopic surgery is less than that in open surgery. In contrast, others have suggested a return to open vs instead laparoscopic surgery during the COVID-19 pandemic, as there may be less risk of aerosols with faster operating times [46]. Up to now, no study has demonstrated the ability of the virus SARS-CoV-2 to be transmitted during a surgical procedure whether open or laparoscopic [47]. Even if laparoscopic surgery is associated with a lower risk of surgical-site infections, a shorted healing time and lower risk for incisional hernia, an advantage of open surgery may be the isobaric setting around the surgical field. However, during any use of electrocoagulation, tissue-specific aerosols may develop. Kwark’s study [33] found that surgical smoke contained HBV in 10 of 11 hepatitis B patients who underwent laparoscopic or robotic surgery.
Insufflation
Laparoscopic, minimally invasive techniques produce aerosols derived from the induced pneumoperitoneum. The risk of an aerosol carryover is reduced by insufflation-systems equipped with smoke-gas elimination (smoke evacuation) and defined CO_2_ feeding and discharge; therefore, these systems are to be preferred for patients with COVID-19 [46]. Alternatively, it is recommended that older insufflator-instruments are used which have disposable smoke gas-filters (acc. to ISO 29463) with a Luer-taper connection to remove smoke-gases by filtering [48].
Trocar valve
Accordingly, evacuation of the contaminated smoke at high speed and concentration from the trocar valve into the operating theater may increase the risk of transmission compared to the open surgery.
Proximity to the source of surgical smoke
The place where the smoke is most concentrated is undoubtedly its source. Smoke density attains a maximum in the area up to ~150 cm from the source of the smoke [49]. Therefore, the surgeon, who is closest to the smoke source is most exposed to smoke (3,000 µg/m^3^, 10^5^ particles/cm^3^) [9], [21], [38], [50], [51], followed by the residents and nurses around the operation table. While performing surgery on HPV-related cervical pathologies, gynecologists have an increased risk of HPV transmission they are close to the smoke source [52].
Although some publications claim exposure to surgical smoke is equal for all staff in the operating theater [8], [21], [53], the present author points out that those authors reached their conclusion based on the smoke-sample collection methods used during the studies (such as long smoke transfer lines) and the use of ventilation systems in the operating theater which aspirate from the ceiling (conventional) or blow from the ceiling (laminar flow) [21], [53]. For example, Kocher et al. [8] concluded that the surgeon and other operating theatre personnel had similar exposures, but they measured the average concentration of VOC to be the highest, at 272.69 parts per billion (ppb) per volume (max. 8,991 ppb), near the surgeon. The present author finds this conclusion controversial, because those authors evaluated only the distribution of the average maximum amount of the VOCs they selected, not the total distribution of all substances.
Surgical masks
The characteristics of the mask used by the operating theater team affect the severity of exposure to smoke and the risk of possible microorganism transmission. Depending on the characteristics of the mask, 20% to 100% of particles smaller than 1 µm penetrate through it [54]. Mostly surgical masks are used during surgery. It is known that surgical masks cannot filter particles <5 µm. This means the smoke passes almost completely through the mask and reaches to the airways of the surgical team (Figure 1 (Fig. 1)) [28], [55], [56].
Additionally, the effect of the surgical mask is close to null because it is not properly tied during the operation and does not completely close the airways [54], [56], [57]. Thus, particles, most of which are smaller than 5 µm, can reach deep into the respiratory tract (Figure 1 (Fig. 1)) [28]. The limited effect of the surgical mask may be to stop substances and droplets larger than 5 µm. An experimental study reported that 99.80% of the ineffective viral RNA carried by surgical smoke is filtered out by the surgical mask, which clearly contradicts the above information [36]. In a study reporting that surgical masks reduced droplet-borne SARS-COV-2 transmission by 42%. This rate seems possible based merely on the droplet size being >5 µm [58]. N95 masks, defined as filtering face-piece (FFP) respirators, filter much smaller particles (at least 95% of 0.3 µm particles) but are not as effective (99%) as FFP3 and N100 masks [32], [55], [56]. The limitations of the use of N95 and N100 masks are that they fit tightly to the face, making breathing difficult, causing temporary facial damage, and are relatively expensive.
Removing the surgical smoke from the breathing zone
Removal from the source
Passive or active smoke-removal methods are available. Active evacuation of the smoke as soon as it emerges from its origin can be performed by a central aspiration system or a mobile device with a filter via the suction line located close to the smoke’s origin [50], [59]. In such a case, the total amount of VOCs is 3,000 µg/m^3^ (8,700 particles/cm^3^) around the operating table decreases to approximately 175 µg/m^3^ (1,600 particles/cm^3^) by using a smoke evacuation system (SES) [50], [59]. Some authors state that the use of SES does not significantly reduce the total amount of VOCs, but they did detect a significant decrease in some specific VOCs [8]. Those authors mentioned acrylonitrile, pentadiene, methyl-2-butenalin, hydrogen cyanide, formaldehyde, butadiene and butenes among these VOCs [8]. However, they did not evaluate the effect of the central ventilation system on the results of their study.
SES is effective if it is close to the source of the smoke. The power of the smoke evacuation system increases when it is placed closer to the smoke source and the power setting of the device is increased [42]. Many researchers have presented many inexpensive and alternative innovative methods for evacuation of smoke from near the source (since mobile smoke filter devices are expensive) [16], [60], [61], [62], [63], [64]. In addition, irrigation with water is recommended as an innovative technique, especially during laparoscopic laser application. Some authors reported a significant reduction in the amount of smoke by irrigating with water [65]. A different study recommended precipitating the smoke in the abdomen by an electrostatic method during laparoscopic surgery. Using the electrostatic method, there was no need to interrupt the surgical procedure, clean the camera lens, or additionally evacuate the abdominal air [66]. If the smoke precipitation in the abdomen is not performed, exposure to smoke increases indirectly.
Smoke removal from the operating theater through a ventilation system
Central ventilation systems blow the smoke and diffuse it into the operating theater, then discharge it through the channels in the walls of the room. This could be suggested as a passive method for smoke removal. Conventional operating-room central ventilation systems are classified as laminar or turbulent mixed airflow systems and negative pressure systems [67]. The conventional system does not blow filtered air; however, it provides ambient air exchange by drawing air through the channels in the ceiling. The laminar flow ventilation system (LVS) blows the filtered air from the ceiling or walls and exchanges the ambient air by drawing it through channels in the walls. The negative pressure system provides suction with reinforced laminar flow from the ceiling and negative pressure from the walls in the closed operating theatre. This system was first used during the SARS epidemic in 2003 [67].
The characteristics of the operating-room central ventilation system produce different effects (independent of the smoke) [67], [68], [69], [70]. Conventional ventilation systems increase the amount of all particles near the surgeon and the risk of bacterial contamination in the operating area [69], [70]. This risk is also mentioned for LVS in two other studies, which allows anticipating a similar effect for the smoke [69], [70]. LVS, on the other hand, has been found to significantly reduce the quantity and concentration of particles near the surgeon [38], [49], [71]. It is thought that LVS achieves its reducing effect by first dispersing the dense smoke from the source through the operating room and then removing it through the air vents in the walls. Contrary to this, Hofer et al. [68] reported that LVS caused more smoke to concentrate near the surgeon. The authors suggested that surgical lamps caused smoke to concentrate near the surgeon by blocking the tabletop airflow and increasing the temperature below the lamps [68]. Other studies stated that LVS distributed the dense smoke from the source through the operating room, exposing the personnel far from the operating table to the same extent as the surgeon at the table [8], [53]. Van Gestel [53] asserted that the resident and nurse were more exposed to the smoke than was the surgeon. They performed this study in an operating room with LVS with horizontally placed blower and evacuation channels on the opposite walls [53]. This might have allowed the smoke to be directed towards the other members of the team.
The number and mobility of personnel in the operating theater generally disrupt the air flow that increases the number of macro- and microparticles in the air and indirectly causes surgical site infections [72], [73]. Thus, it can be predicted that the increase in the number and mobility of personnel will delay smoke evacuation by disrupting the airflow created by the central ventilation system. However, no research on this issue was found.
Symptoms caused by surgical smoke in healthcare personnel
Acute side effects and risks
In general, large particles are of biological concern due to the transport risk of cell and tissue particles as well as droplets, while small particles pose more of a chemical concern as they can reach as far as the alveoli (Figure 1 (Fig. 1)) [5], [20], [22], [28].
Particles smaller than 5.0 µm, which cross the surgical mask barrier and reach the alveoli, cause noticeable, acute effects. A number of them are dizziness-drowsiness (74.2%), headache (72.8%), cough (70.3%), dizziness (68.6%), tearing (65.7%), nausea (63.4%), throat irritation (56.6%), smell of smoke in the hair (43.7%), and fatigue (28.2%) (Table 5 (Tab. 5)) [74], [75], [76]. Probabilities of viral and bacterial transmissions are mentioned above.
Chronic risks
In public life, prolonged exposure to small particles suspended in the air has been associated with increased risk of lung, breast, uterine, ovarian, colon, and prostate cancers [77]. Surgical smoke has been reported to cause cardiovascular diseases, lung injuries, such as pneumonia, chronic bronchiolitis, emphysema, and pulmonary fibrosis, in addition to blood disorders (e.g. anemia, leukemia), in the long-term [3], [4], [5], [20], [78]. Besides to the carcinogenic, mutagenic and potential teratogenic risks of it, smoke is also known as a tumor-cell carrier, and tumor cells can be cultivated from smoke samples [27], [79]. The mutagenic effect of surgical smoke is estimated to be greater than that of cigarette smoke, and may increase depending on the type of tissue processed. It was found that the mutagenic potential of the smoke resulting from the ablation of 1 g of tissue with electrocautery was equivalent to the smoke of 6 unfiltered cigarettes. Accordingly, it is predicted that in the operating theater, a surgeon exposed to surgical smoke is subject to the same mutagenic power created by the smoke of 27–30 unfiltered cigarettes per day (depending on the brand) [4]. Some authors have stated that the concentration of small particles in the operating theater does not exceed that of office air but is much lower than in cigarette smoke, and that the mutagenic potential of the surgical smoke is negligible [43]. They speculated that this was probably due to the intermittent use of electrocautery and high-velocity ventilation during surgery.
Awareness
It is a rare surgeon who does not use a power device. However, the rate of the evacuation of the smoke from the operation table ranges from 14% to 70% [78], [80]. If evacuation is needed, the majority (90%) of the surgeons use the standard central aspiration system for this purpose [78]. According to a 2012 study, only 66% of the operating theaters had an SES [4]. However, the current rate of SES equipment in the operating theaters may have increased by now. Elsewhere, the SES usage rate is reported to be as low as 16.8% to 0% [74], [78], [81]. The low usage rate of SES varied according to the surgeon and the surgical procedure performed. The reasons why the surgeons used SES were to obtain clear vision (76.9%), safety (61.5%) and deodorization (15.3%) [4].
Awareness of smoke toxicity has increased over the years, but has not yet been fully realized by all [78], [80], [81], [82]. In 2007, although 51% of surgeons considered the smoke to be harmful, residents and operating-theater nurses were more aware of its harmful effects, i.e., 78% and 91%, respectively [81]. A publication in 2020 found that although awareness had increased (95%), only 50.4% of the surgeons considered smoke very harmful and tried to avoid it (51%) [81]. Nurses also had varying degrees of awareness (44.4%–80%) [74], [81]. These rates show that there is still much room for improvement in terms of awareness of and protection against surgical smoke. In one survey [83], surgeons and anesthetists perceived less risk from the smoke and claimed lower exposure to the smoke than nurses. Males had a low perception of risk. Moreover, surgeons support a diathermy smoke-free policy less (78%) than do nurses and anesthetists. Nurses (86%) and – with a low frequency (49%) – surgeons suggest that making smoke-evacuator use mandatory is the best way to manage smoke exposure. These results show a great need for surgeons’ awareness to improve.
A review by Dixon et al. [84] contains contradictory statements about awareness. Conclusions in their abstract and in discussion sections differ. In the conclusion of the abstract, the authors stated that smoke was hazardous and advised protection. However, they claimed that high-level evidence for infectivity potential of the smoke does not exist. They seemed to accept ‘a possible link’ between the surgical smoke and HPV infection and concluded that surgical smoke does not cause permanent health problems in long-term follow-ups. Moreover, they concluded that carcinogenic chemicals had a low carcinogenic potential overall. They reviewed 28 studies, of which 92% were experimental and had a limited number of subjects. These implications drawn by those authors are beyond their study’s results. This demonstrates that even the authors’ awareness of surgical smoke is conflicted.
Stewart [85] pointed out some limitations and contradictions in a number of studies in her editorial article and concluded that the hazards of surgical smoke are generally overstated. Moreover, she claimed other authors had clear conflicts of interest in the medical device industry. The author Stewart concluded that the hazards from direct inhalation of surgical smoke is hypothetical and does not occur in the operating theater [85]. According to the author of the present article, who suffered from acute illnesses for many years due to surgical smoke, this suggestion seems more harmful than ignorance.
In the literature, the rate of education and training on surgical smoke was reported at about 56% [3], [74], [80]. However, it may be as low as 16%–20.4% for surgeons and operating theater nurses [74], [81]. An average of 60% of healthcare professionals think that warnings and standards about the deleterious effects of surgical smoke are insufficient [78], [80]. Moreover, as the author of this article experienced, some surgeons offer no institutional support when this problem is pointed out [78]. Fortunately, despite the lack of institutional interest and support, the literature reflects that something is changing. A search in PubMed with the keyword “surgical smoke” presented 117 articles from the year 1900 up to April 2018 (in 118 years) and 215 articles up to April 2023 for the last 5 years [86], [87].
Guidelines and regulations
The National Institute for Occupational Safety and Health (NIOSH) states five levels of actions to reduce or remove hazards in the workplace, which is named as ‘the hierarchy of controls’ [88]. NIOSH first published a guideline on controlling surgical smoke in 1996 [89]. Recommendations in the guideline are still up to date and are clearly organized in ‘the surgical smoke hierarchy of controls’ [89], [90].
In detail, the surgical smoke hierarchy of controls are
- Elimination: preventing surgical smoke production and removing all the smoke emitted;
- Substitution: evaluating alternative surgical power devices that generate less surgical smoke;
- Engineering controls: isolating the smoke from the operating theater staff by every feasible method and device, and modifying equipment or the workspace, using protective barriers, ventilation, and more;
- Administrative controls: establishing policies and procedures with periodical review and revision, providing education, training in work processes, ensuring adequate rest breaks, job rotation, limiting access to hazardous areas. Perioperative personnel should participate in improvement programs by relevant health-care organizations of countries;
- Personal protective equipment: using appropriate masks, eye and face protectors, suitable surgical cap, gowns according to the power devices used, and insisting on using high quality equipment [89], [90], [91], [92].
Finally, the health care organizations of the countries are obligated to provide a surgical-smoke-free work environment, and the operating-room staff has responsibilities and obligations to protect themselves from exposure to smoke.
Conclusion
Power devices (e.g., electrocautery, ultrasonic and laser devices) produce surgical smoke with a particle size as small as 0.007µm during the surgical procedures. Currently, more than 1,000 different chemicals have been identified in the smoke. There are high amounts of toxic, carcinogenic and mutagenic substances among these chemicals. Surgical masks cannot filter particles smaller than 5 µm. In this case, 95% of the smoke particles which crossed the mask reaches deep into the respiratory tract.
Surgical smoke often causes headache, dizziness, nausea, eye and respiratory tract irritation, weakness, abdominal pain, dysrhythmia, hypertensive attack, etc. in the acute period. Long-term effects of surgical smoke on various diseases have consistently been ignored.
Bacteria and viruses, mostly <2.5 µm in size, can be transported by the smoke and there is a potential risk of contamination. Among these viruses, SARS-CoV-2, HIV, HPV, HBV must be considered.
Mutagenic and carcinogenic compounds as well as malignant cells may also be found in the smoke. Therefore, surgical smoke inhalation is a significant chemical and biological occupational hazard in the operating theater. Surgical smoke is as mutagenic as cigarette smoke. No hospital would think of allowing smoking in the operating theater to protect non-smokers. In contrast, protection from exposure to surgical smoke does not receive the analogous attention.
The quantity of the smoke changes with the technique of the surgeon, the characteristics of the power device used, the energy level set, the characteristics of the tissue processed and the ventilation or smoke evacuation system. The most effective method is to collect the smoke from the origin with an aspiration system and to evacuate it to the outside.
Awareness and legal regulations in terms of hygiene, toxicology, occupational health, and safety should be increased.
Notes
Competing interests
The author declares that he has no competing interest.
Funding
None.
Author’s ORCID
Nurettin Kahramansoy: 0000-0001-8990-5073
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Barrett WL Garber SM Surgical smoke: a review of the literature. Is this just a lot of hot air?Surg Endosc Jun 200317697998710.1007/s 00464-002-8584-512640543 · doi ↗ · pubmed ↗
- 2Mowbray N Ansell J Warren N Wall P Torkington J Is surgical smoke harmful to theater staff? A systematic review Surg Endosc 20132793100310710.1007/s 00464-013-2940-523605191 · doi ↗ · pubmed ↗
- 3Bree K Barnhill S Rundell W The dangers of electrosurgical smoke to operating room personnel: a review Workplace Health Saf 2017651151752610.1177/216507991769106328414627 · doi ↗ · pubmed ↗
- 4Hill DSO'Neill JK Powell RJ Oliver DW Surgical smoke – a health hazard in the operating theatre: a study to quantify exposure and a survey of the use of smoke extractor systems in UK plastic surgery units J Plast Reconstr Aesthet Surg 201265791191610.1016/j.bjps.2012.02.01222445358 · doi ↗ · pubmed ↗
- 5Fan JK Chan FS Chu KM Surgical smoke Asian J Surg 200932425325710.1016/S 1015-9584(09)60403-619892630 · doi ↗ · pubmed ↗
- 6Choi SH Choi DH Kang DH Ha YS Lee JN Kim BS Kim HT Yoo ES Kwon TG Chung SK Kim TH Activated carbon fiber filters could reduce the risk of surgical smoke exposure during laparoscopic surgery: application of volatile organic compounds Surg Endosc 201832104290429810.1007/s 00464-018-6222-029770884 · doi ↗ · pubmed ↗
- 7Pierce JS Lacey SE Lippert JF Lopez R Franke JE Laser-generated air contaminants from medical laser applications: a state-of-the-science review of exposure characterization, health effects, and control J Occup Environ Hyg 201187447466 Available from: 10.1080/15459624.2011.58588821726157 · doi ↗ · pubmed ↗
- 8Kocher GJ Koss AR Groessl M Schefold JC Luedi MM Quapp C Dorn P Lutz J Cappellin L Hutterli M Lopez-Hilfiker FD Al-Hurani M Sesia SB Electrocautery smoke exposure and efficacy of smoke evacuation systems in minimally invasive and open surgery: a prospective randomized study Sci Rep 2022121494110.1038/s 41598-022-08970-y 35322134 PMC 8943181 · doi ↗ · pubmed ↗