Pyrexia of Unknown Origin Caused by Non-Hodgkin’s Lymphoma: A Diagnostic Challenge for Clinicians
Hassan Hussain, Chaminda Janaka, Anne Sonali Rodrigo, Manojkumar Krishnan, Azra Hassan

TL;DR
A 69-year-old man with a persistent fever and neck lump was eventually diagnosed with non-Hodgkin’s lymphoma after multiple inconclusive tests.
Contribution
This case highlights the diagnostic challenges of non-Hodgkin’s lymphoma presenting as fever of unknown origin.
Findings
Initial imaging and biopsies failed to diagnose the patient's condition.
A third lymph node biopsy confirmed non-Hodgkin’s lymphoma.
The patient showed mild improvement after chemotherapy.
Abstract
Non-Hodgkin’s lymphomas (NHLs) are a group of lymphoproliferative diseases that originate from different cell types, namely B cells, T cells, or natural killer cells. Herein, we report the case of a 69-year-old male patient who presented with a gradual-onset, intermittent, low-grade fever for four months and a right-sided neck lump for two months. On examination, a right-sided enlarged lymph node sized 1 × 1 cm2 was noted, which was mobile, hard in consistency, and non-tender. No other lymphadenopathy was noted in other parts of the body. Imaging and biochemical studies done at the initial stages did not reveal features in favor of any lymphoproliferative disorders, and the two lymph node biopsies done two weeks apart were inconclusive as well. An extended panel of investigations was done in view of excluding other infective and inflammatory pathologies, which was negative, making the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
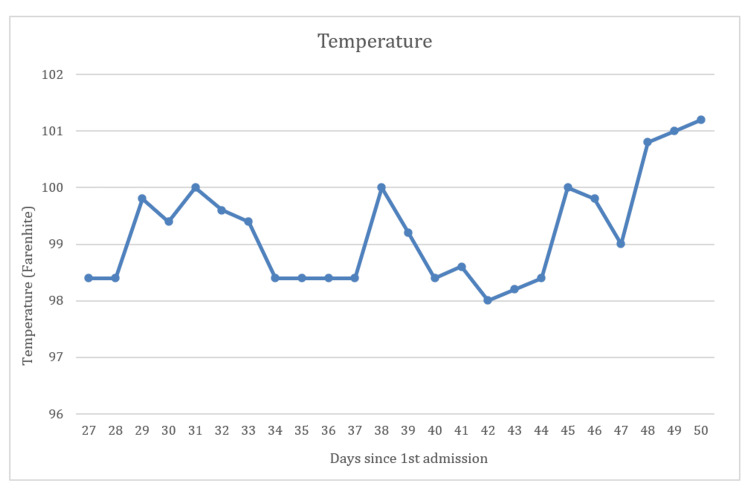 Figure 1
Figure 1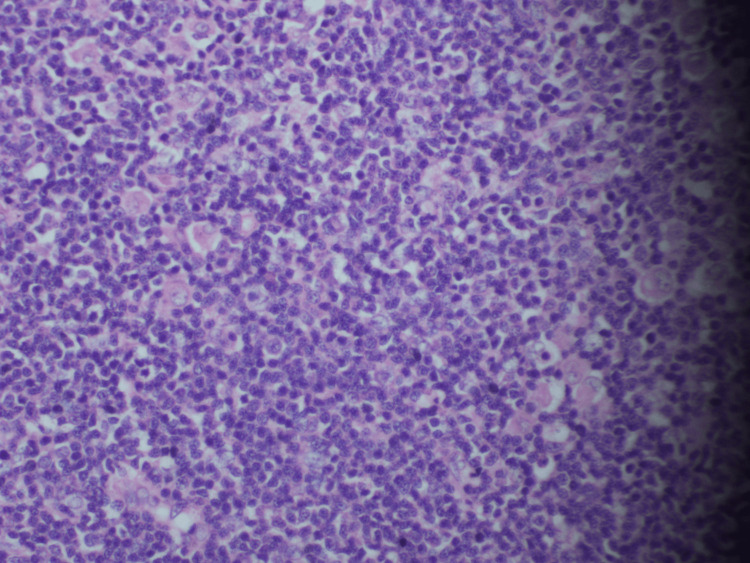 Figure 2
Figure 2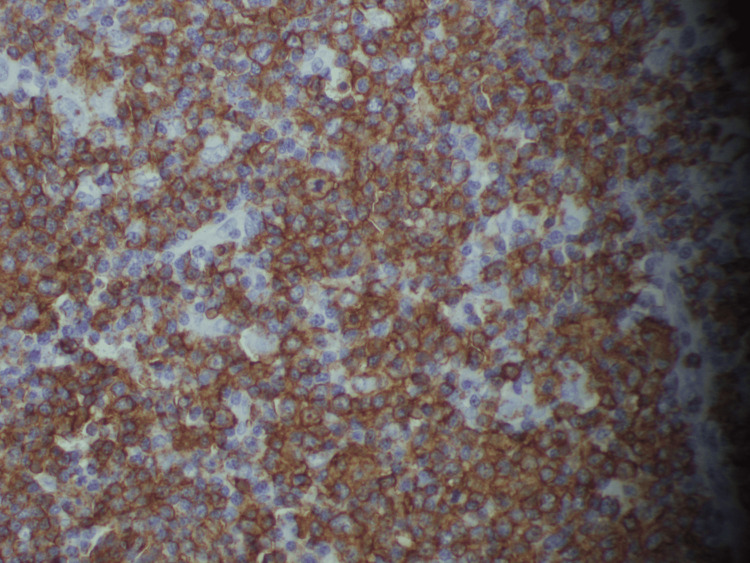 Figure 3
Figure 3| Investigations | Values | Reference range | ||||||
| 1st admission | 2nd admission | |||||||
| D1 | D27 | D33 | D35 | D38 | D41 | |||
| Full blood count | White cell count (*103) | 6.74 | 6.60 | 6.63 | 6.07 | 8.54 | 7.59 | 4–11 |
| Neutrophils (%) | 62 | 3.8 | 33 | 48 | 61 | 62 | 50–70 | |
| Lymphocytes (%) | 22 | 1.78 | 33 | 34 | 26 | 25 | 20–40 | |
| Hemoglobin (g/dL) | 11.8 | 9.8 | 11.9 | 10 | 10.8 | 10.5 | 12–14 | |
| Platelets (*103/µL) | 411 | 290 | 329 | 296 | 307 | 370 | 150–400 | |
| Liver biochemistry | Alanine transaminases (U/L) | 144 | - | - | - | - | 24 | <40 |
| Aspartate transaminases (U/L) | 22 | - | - | - | - | 33 | 0–37 | |
| Alkaline phosphatase (U/L) | 144 | - | - | - | - | 164 | 30–120 | |
| Total bilirubin (mg/dL) | 0.4 | - | - | - | - | 0.5 | 0.2–1.1 | |
| Serum albumin (g/dL) | - | - | - | - | - | 3.1 | 3.4–5.4 | |
| Serum globulin | - | - | - | - | - | 3.9 | 2–4 | |
| Inflammatory markers | C-reactive protein (mg/L) | 65 | 49 | 91 | 25 | 32 | 76 | <5 |
| Erythrocyte sedimentation rate (mm in 1st hour) | 76 | 88 | 90 | - | - | 67 | <20 | |
| Procalcitonin (ng/mL) | 0.1 | - | - | - | - | - | <0.1 | |
| Serum electrolytes | Serum sodium (mmol/L) | 141 | - | - | - | - | - | 135–145 |
| Serum potassium (mmol/L) | 3.7 | - | - | - | - | - | 3.5–5.5 | |
| Serum total calcium (mg/dL) | - | - | - | 8.40 | - | - | 8.5–10.5 | |
| Adjusted calcium (mg/dL) | - | - | - | 8.88 | - | - | 8.6–10 | |
| Renal function tests | Serum creatinine (µmol/L) | - | 69 | - | - | - | - | 65–104 |
| Other investigations | D-dimers (ng/ml) | - | - | - | - | 1982 | - | <550 |
| Serum lactate dehydrogenase (U/L) | 187 | - | - | - | - | 205 | <330 | |
| Tumor markers | CEA (ng/ml) | - | - | - | - | - | 2.4 | 0–5 |
| Alpha fetoprotein (ng/ml) | - | - | - | - | - | 1.49 | 0–8.5 | |
| CA 19-9 (U/ml) | - | - | - | - | - | 4 | <35 | |
| Iron studies | Serum iron (µmol/L) | 2.9 | 10–30 | |||||
| Total iron binding capacity (mcg/dL) | 27 | 240–450 | ||||||
| Transferrin saturation (%) | 10.3 | 15–50 | ||||||
| Serum ferritin (ng/mL) | 250 | 20–250 | ||||||
| ANA test | Negative | |||||||
| Rheumatoid factor | Negative | |||||||
| Thyroid profile | Serum TSH (µIU/mL) | 0.588 | 0.35–5.5 | |||||
| Free T4 (ng/dL) | 1.06 | 0.7–1.48 | ||||||
| PSA (ng/mL) | 2.4 | <4 | ||||||
| Blood picture | Mild anemia with left shift of neutrophils with toxic changes suggestive of infective or inflammatory process. | |||||||
| Right-cervical lymph node biopsy-1 (1st admission) | Appearances are compatible with chronic sialadenitis of submandibular gland. No evidence of a lymph node. | |||||||
| Right-cervical lymph node biopsy-2 (2nd admission) | Inconclusive viral infection is most likely | |||||||
| Right-cervical lymph node biopsy-3 (2nd admission) | Left cervical lymph node level 2 showing features of high-grade non-Hodgkin lymphoma of B lineage. | |||||||
| Bone marrow biopsy | Reactive marrow with granulocytic hyperplasia with mildly increased monocytes/macrophage activity evidence of mild iron deficiency noted no evidence of leukemia/lymphoma/myeloma or non-hemopoietic cell infiltration trephine biopsy-consistent with bone marrow aspiration findings. | |||||||
| Schirmer's test | Negative | |||||||
| Serum protein electrophoresis | Reduced albumin. But no abnormal bands. | |||||||
| Infective screening | Results |
| Urine full report | Normal (repeated 3 times) |
| Urine culture | No growth (repeated 3 times) |
| Blood culture | No growth (repeated 3 times) |
| Sputum culture | No growth |
| Sputum GeneXpert | Negative |
| Stool for microscopy | No parasites, amoeba, cyst, or ova seen |
| CSF analysis | Appearance - colorless/clear glucose – 45 mg/dL (50-85) protein – 57 mg/dl (15-45) white cell count – nil red cells - 168 |
| CSF culture | No growth |
| TB culture of bone marrow aspirate | Not isolated after 2 weeks of growth |
| Sputum acid fast bacilli | 3 samples negative |
| Malarial parasite (microscopy and RDT) | Negative |
| HIV 1 and 2 antibodies | Negative |
| Mantoux test | Negative |
| Venereal diseases laboratory test | Non-reactive |
| Urine for acid fast bacilli | Not seen |
| Filaria antibody test | Negative |
| Brucella antibody | Negative |
| Hepatitis B surface antigen | Negative |
| Hepatitis C antibody | Negative |
| Salmonella typhi O,H and Para typhi antigens | Negative |
| Melioidosis antibodies | Negative |
| Epstein Barr virus antibodies | Negative |
| Typhoid antibodies | Negative |
| Imaging studies | Results |
| Upper gastrointestinal endoscopy | Normal |
| Lower gastrointestinal endoscopy | Normal |
| Trans esophageal echocardiography | No evidence of infectious endocarditis |
| 2D echocardiography | Normal. Did not have vegetation or shunts |
| USS KUBP | Prostatomegaly with no significant post-voidal volume. |
| CECT chest, abdomen, and pelvis | Heterogenous-enhancing area in anterior mediastinum most likely residual thymic tissues. Few prominent bilateral cervical lymph nodes noted bilateral non-obstructing renal calculi simple liver cyst in segment v11 of liver. |
| Venous doppler study of bilateral lower limbs | No features of deep vein thrombosis |
| Ultrasound scan of neck | Features suggestive of chronic submandibular sialadenitis. Bilateral cervical lymphadenopathy with possible necrotic lymph nodes at level 2. |
| Stage | Features |
| Stage 1 | Involvement of a single lymph node region or lymphoid structure |
| Stage 2 | Involvement of 2 or more lymph node regions on the same side of the diaphragm |
| Stage 3 | Involvement of lymph regions or structures on both sides of the diaphragm |
| Stage 4 | Involvement of extranodal site beyond that is designated in E |
| For all stages | |
| A | No symptoms |
| B | Fever (38 °C), drenching sweats, weight loss (10% body weight over 6 months) |
| For stages 1 to 3 | |
| E | Involvement of a single, extra nodal site contiguous or proximal to known nodal site |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphoma Diagnosis and Treatment · Hematological disorders and diagnostics · Viral-associated cancers and disorders
Introduction
Tumors of the lymphoid system can be broadly classified as Hodgkin’s lymphoma (HL) and non-Hodgkin’s lymphoma (NHL) [1]. NHL is a malignancy that has a wide range of presentations. It most commonly involves the lymph nodes and presents with generalized lymphadenopathy, yet there can be extranodal involvement as well. The extranodal sites include the stomach, lungs, and skin. The incidence of NHL has increased over the years, and among all malignant neoplasms, NHL usually presents in the 6th decade of life, with a preponderance among men [1].
NHL is characterized by abnormal cell clone proliferation, either involving T cells, B cells, or both cell types. Most of the NHLs originate from B cells, and the majority of patients express the CD20 antigen [2,3]. Considering the tumor activity, some of the NHLs are indolent malignancies with a lower tumor grade, while some NHLs are very aggressive [1]. NHLs are usually present at the age of 42, and the prevalence of the disease increases with age [4]. The most common histological type is diffuse large B-cell lymphoma. Various imaging modalities, including computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET), are valuable in finding nodal and extranodal sites of involvement, which can be further analyzed by tissue biopsies as well. Immunohistochemistry studies help in evaluating the positivity of CD20 and Ki67 [1].
Case presentation
A 69-year-old retired teacher from Western Province, Sri Lanka, presented with a gradual-onset, intermittent, low-grade fever for four months. The fever was associated with chills, but not rigors, and was markedly noted in the evening and early hours of the morning every day. The fever slightly responded to simple analgesics but recurred from time to time. The patient reported a history of intermittent episodes of dry cough with whitish sputum for the same duration but no history of shortness of breath, pleuritic chest pain, or hemoptysis. He had no contact history of tuberculosis either. He denied having any history of headache, trauma to the head, or altered level of consciousness, as well as visual disturbances or photophobia.
There was no history of recurrent vomiting or abdominal pain. The patient reported no changes in his bowel motions. He complained of a few lower urinary tract symptoms, such as urgency, increased frequency, and nocturia, for about six months and was on oral tamsulosin at 0.4 µm daily at the time of presentation. He denied a history of girdle pain or weakness in any part of the body. There was no history of joint pains, alopecia, or skin rashes, and the patient did not have a history of significant weight loss, loss of appetite, or night sweats.
The patient traveled to India in 2019 on a religious pilgrimage and had been there for 20 days. However, no history of illnesses or hospital admissions around the time was noted. He had no history of exposure to animals or poultry and no history of consuming unpasteurized milk.
The patient reported noting a lump on the right side of his neck about two months ago. Initially, it was about 0.5 × 0.5 cm^2^ in size, and no skin changes like erythema or discharges were noted from the lump. Since the patient did not see any significant increase in the size of the lump over the past two months, he did not seek medical advice. His past medical history was insignificant, with no history of valvular heart diseases. He underwent a left-sided laser lithotripsy procedure nine months ago due to a left-sided renal calculus. He denied a family history of any chronic medical conditions or malignancies. He was a non-smoker and a teetotaler with no history of illicit drug abuse. He denied having risky sexual behaviors and was not allergic to any substance, drug, or food item.
The patient, who lived with his wife and daughter, reported having good family support and financial stability. The patient was an averagely built male whose appearance was consistent with his chronological age. He had a body weight of 43 kg, a height of 171 cm, and a body mass index (BMI) of 14.7. He was afebrile at the time of admission. There was no conjunctival pallor, plethora, or icterus. On the right side, there was an enlarged lymph node, which was around 1 × 1 cm^2^ in size. It was mobile, hard on consistency, and non-tender. No other part of the body showed any signs of lymphadenopathy. No enlarged thyroid gland was noted. There were no skin rashes, and no peripheral stigmata of infective endocarditis was present. Ankle edema was not noted.
The patient had a pulse rate of 80 beats per minute, which was regular and normal in volume and character. Peripheral pulses were present, and there were no delays. His blood pressure was 120/80 mmHg. The cardiovascular system examination was unremarkable, with no murmurs. He had a respiratory rate of 12 per minute with bilateral equal air entry in all zones and vesicular breathing. No added sounds like crepitations or rhonchi were noted. Abdominal examination was unremarkable, with no organomegaly, palpable masses, or free fluid. He did not show any signs of meningism, and the fundoscopic examination was unremarkable, with absent Roth spots, toxoplasma chorioretinitis, choroid tubercles, or cystoid bodies. Cranial nerve examination was normal, and no features of peripheral neuropathy were present.
To arrive at a diagnosis, serial investigations were performed, which have been summarized in Table 1. Despite extensive evaluation, no diagnosis for the patient’s presentation could be elicited, and he was discharged after 10 days of admission to be reviewed with the right-sided lymph node biopsy report. He was not initiated on any antibiotics during this admission.
The patient was readmitted 27 days after the initial admission for further investigation of a fever. At the time, he had the biopsy report from the previous admission, which showed evidence of chronic sialadenitis of the submandibular gland with no evidence of lymphadenopathy [1]. Hence, the diagnosis was inconclusive, and serial imaging studies were performed. Furthermore, infective screening (Table 2) as well as imaging studies (Table 3) were performed as well.
The patient was initiated on antibiotics during this admission, which included an intravenous combination of cefuroxime, ceftriaxone, piperacillin, and tazobactam, along with meropenem and doxycycline. Despite antibiotic administration, his fever continued with a slight variation in severity. The pattern of fever is shown in Figure 1.
Body temperature chart plotted against the days since admission
Hematoxylin and eosin (H&E) staining of the left-sided level 2 cervical lymph node showed atypical lymphoid cells with enlarged nuclei, clumped chromatin, and moderate-to-scant eosinophilic cytoplasm. We observed mitoses without any signs of tumor necrosis. These features are compatible with diffuse large B-cell lymphoma (Figure 2).
Microscopic view of the left-side level 2 cervical lymph node
Although almost all the investigations were normal at the initial stages, the third lymph node biopsy performed during the second admission showed evidence of diffuse large B-cell lymphoma with germinal center B cell type (Figure 3) [1]. Hence, an NHL diagnosis was confirmed, and the patient was initiated on chemotherapeutic management with rituximab, cyclophosphamide, doxorubicin, and vincristine, after which a symptomatic improvement in his clinical state was noted.
Immunohistochemistry of the left-sided level 2 cervical lymph node showing diffuse cytoplasmic positivity for CD20 and few background cells showing cytoplasmic positivity for CD3
Discussion
Malignancies of the lymphoreticular system are sometimes collectively called lymphomas. These malignancies stem from lymphatic tissue and may extend to an extra-nodal site (NHL) or transform into non-tender masses in the lymph node region (HL). At the latter stages, they may spread to various other lymph node groups and may involve the bone marrow [1]. Based on the World Health Organization’s (WHO) modified version of the Revised European-American Lymphoma classification, lymphoid malignancies can be classified into three sub-categories, namely B-cell lymphoma, T-cell or natural killer cell lymphoma, and HL [1].
Among head and neck malignancies, the NHL has a special place, and Waldeyer’s ring is the most common site of origin for these NHLs [1,5]. Most head and neck NHLs have cervical nodal involvement as well. This was seen in this case as well. Paranasal sinuses, orbits, salivary glands, and the nose are among the other sites in the head and neck region that are commonly involved in NHLs [5]. Considering the clinical course of the disease, NHLs have varying clinical presentations and heterogeneous morphological appearances. A wide variation in response to treatment is also seen in NHLs. The cellular variation of NHLs depends on at which stage of development the cells are arrested, their grade of anti-apoptotic abnormality, etc. [1].
Based on cell maturation, NHLs are further classified as immature and mature variants. Based on the cell of origin, they are classified as B cells, T cells, or natural killer cell types [1]. Immunohistochemistry markers vary for each type; while CD20 and CD79a are used as markers for B-cell tumors, CD3 and CD5 are used as markers for T-cell tumors [6]. Immunohistochemistry markers are important in determining the specific lineages and the stage of development of the lymphoma. In this case, immunohistochemistry studies revealed positivity for CD20 and BCL2, and stains were negative for CD3 and CD10. Hence, it was identified as a diffuse B-cell lymphoma. The tumor grade was identified as a high-grade tumor, as the Ki67 index was 71%.
Primary lymphomas are common in males in their fifth and sixth decades of life. Considering the presentation of our case, the age group and gender of the patient matched the classical presentation of a patient with NHL (a male patient aged 69 years). In terms of geographical location, NHLs are more common in developed countries than in developing nations. Since this patient was from Sri Lanka, it did not align with the above finding.
The diagnosis of NHL is based on imaging studies, histological evaluation, and immunohistochemistry. In diffuse large B-cell lymphoma, the most sensitive investigation is a PET scan [7]. It has been shown to have more sensitivity than a bone marrow biopsy [8]. This was evident in this case because the bone marrow biopsy done in this patient did not reveal evidence of any lymphoproliferative disorders, and it led to the diagnosis being missed at the initial stage. A PET scan could not be performed on this patient due to financial constraints. However, a PET scan is not foolproof, as there would still be a chance of missed diagnosis in the case of low-volume diffused lesions [7]. But this outweighs the benefits of a PET scan, which enables the diagnosis of the majority of lesions at the first instance itself. Apart from diagnosis, a PET scan is useful in monitoring response to treatment and for restaging the disease following treatment in both HL and NHL.
The Ann Arbor staging system is used for the management of NHLs affecting the head and neck region (Table 4) [1]. Low-grade tumors are usually managed with radiotherapy alone, while patients with high-grade lymphoma with a disseminated clinical picture are treated with a combination of chemotherapy and radiation therapy. This patient was initiated on a chemotherapeutic regime alone, and he showed a good response despite the NHL being a high-grade tumor. Although there is a place for surgical resection for isolated lesions [1], in most cases, surgical enucleation is combined with radiotherapy and chemotherapy for better outcomes.
Diffuse large B-cell lymphoma usually has an aggressive disease progression, with 30-60% of tumors being curable with intensive chemotherapy coupled with rituximab, which is why it was initiated in this patient [9]. R-CHOP (rituximab, cyclophosphamide, hydroxydaunorubicin, oncovin, and prednisone) is the classic protocol initiated in patients with aggressive NHL. It comprises six to seven cycles of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone [9].
Conclusions
NHLs can have varying presentations, and the initial investigations can be negative despite the patient harboring the disease. Hence, this case emphasizes the importance of proper examination, the value of performing serial investigations, and, if clinically indicated, the necessity of performing repeated histological biopsies to arrive at a proper tissue diagnosis. Histological diagnosis is vital and paramount for successful patient treatment and for predicting the disease outcome following treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Non-Hodgkins lymphoma: a case report and review of literature J Oral Maxillofac Pathol Singaraju S Patel S Sharma A Singaraju M 3223262420203345624210.4103/jomfp.JOMFP_271_19PMC 7802842 · doi ↗ · pubmed ↗
- 2Expression of human B cell-associated antigens on leukemias and lymphomas: a model of human B cell differentiation Blood Anderson KC Bates MP Slaughenhoupt BL Pinkus GS Schlossman SF Nadler LM 14241433631984 https://pubmed.ncbi.nlm.nih.gov/6609729/6609729 · pubmed ↗
- 3A revised European-American classification of lymphoid neoplasms: a proposal from the International Lymphoma Study Group Blood Harris NL Jaffe ES Stein H 13611392841994 https://pubmed.ncbi.nlm.nih.gov/8068936/8068936 · pubmed ↗
- 4Treatment of patients with low-grade B-cell lymphoma with the combination of chimeric anti-CD 20 monoclonal antibody and CHOP chemotherapy J Clin Oncol Czuczman MS Grillo-López AJ White CA 2682761719991045824210.1200/JCO.1999.17.1.268 · doi ↗ · pubmed ↗
- 5Atypical clinical presentations of lymphomas: two case reports J Mahatma Gandhi Instit Sci Sekhon S Kolte S Gupta K Yadav A 505212016
- 6Role of immunohistochemistry in lymphoma Indian J Med Paediatr Oncol Rao IS 1451473120102158422110.4103/0971-5851.76201 PMC 3089924 · doi ↗ · pubmed ↗
- 7Cervical lymphadenopathy: unwinding the hidden truth Dent Res J (Isfahan) Ramadas AA Jose R Varma B Chandy ML 73781420172834862210.4103/1735-3327.201136 PMC 5356393 · doi ↗ · pubmed ↗
- 8Detection of lymphoma in bone marrow by whole-body positron emission tomography Blood Carr R Barrington SF Madan B O'Doherty MJ Saunders CA van der Walt J Timothy AR 33403346911998 https://pubmed.ncbi.nlm.nih.gov/9558391/9558391 · pubmed ↗