Chronic Visual Abnormality in an Elderly Patient With Temporal Lobe Epilepsy
Kiyohiro Atsuji, Shuichiro Neshige, Narumi Ohno, Hirofumi Maruyama

TL;DR
An elderly woman with chronic visual issues was diagnosed with temporal lobe epilepsy, which improved significantly with lacosamide treatment.
Contribution
Highlights the challenge of diagnosing epilepsy in the elderly through nonspecific symptoms like visual abnormalities.
Findings
Temporal lobe epilepsy was diagnosed based on MRI and EEG findings in an elderly patient with visual complaints.
Treatment with lacosamide led to significant improvement in symptoms and EEG results.
Mild focal seizures can mimic ophthalmologic issues, complicating diagnosis in older adults.
Abstract
A 79-year-old woman visited our department for chronic visual field abnormalities with a floating sensation for two months. Neurological and ophthalmologic examinations yielded normal results, except for brain MRI indicating left hippocampal atrophy. Cognitive function tests were normal. EEG revealed frequent spikes and slow waves in the left frontotemporal region, corroborated by reduced accumulation in 123I-iomazenil single photon emission computed tomography. A diagnosis of temporal lobe epilepsy was established, and treatment with lacosamide resulted in a remarkable improvement in symptoms and EEG findings. Mild focal seizures from the temporal region might cause mild impaired awareness, resulting in the patient’s report as a sensation of uncertainty between the self and the outside world, mimicking ophthalmologic abnormalities. The repeated nature of the seizures contributed to the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
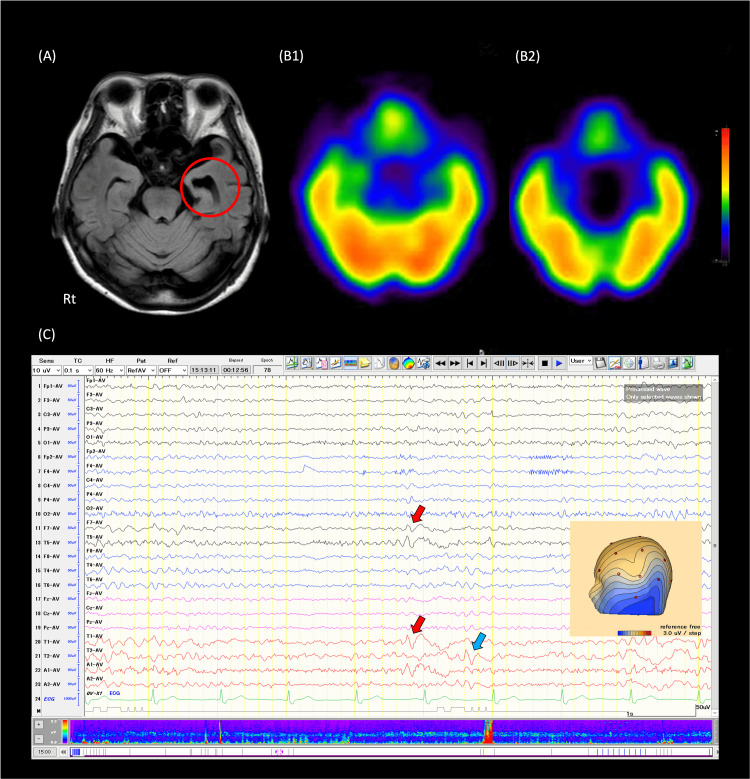 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEpilepsy research and treatment · Autoimmune Neurological Disorders and Treatments · Neuroscience and Neuropharmacology Research
Introduction
With the rapid aging of society, the prevalence of epilepsy in the elderly is increasing. Temporal lobe epilepsy (TLE) is the most common form in this population. The major seizure type is focal impaired awareness seizure (FIAS). The seizures are accompanied by typical ictal semiology such as motion arrest, dystonia, and oral or hand automatism [1]. Therefore, diagnosis in typical cases of TLE is not difficult. However, diagnosing elderly patients with TLE can be challenging, as the complaints might be unspecific, potentially leading to misdiagnoses such as dementia [2]. Herein, we present an elderly patient finally diagnosed with TLE, whose initial symptom was an ophthalmologic complaint.
Case presentation
A 79-year-old woman visited our department for visual chronic field abnormalities with a floating sensation for two months. She complained that her visual symptoms had been persisting. We asked the patient which or all of their visual fields were abnormal, and she responded that her entire visual field was blurred. No visual field abnormalities were elicited when looking in any particular direction. She had a history of well-controlled hypertension and paroxysmal atrial fibrillation managed through oral medication. She had no history of epilepsy and no risk factors for epilepsy such as a precipitating brain injury. The neurological examination yielded normal results. She had no double vision. Repeated ophthalmologic examinations also revealed no abnormalities. Additionally, blood tests revealed unremarkable findings. While brain MRI showed normal findings, including in the optic nerve, it indicated atrophy of the left hippocampus (Figure 1A).
Brain imaging and interictal EEGA. Brain MRI with FLAIR imaging demonstrates atrophy of the medial temporal lobe on the left; B. 123I-iomazenil SPECT (B1: early and B2: late phase) reveals findings compatible with left temporal lobe epilepsy; C. Interictal EEG displays bilateral independent focal sharp waves, predominantly on the left.FLAIR: fluid-attenuated inversion recovery
However, cognitive function tests showed normal results (the revised Hasegawa dementia scale was 27/30), and she maintained independence in daily activities. EEG revealed bilateral independent focal sharp waves, occurring every several pages, predominantly on the left, during both awake and drowsy states (Figure 1C). There was no ictal EEG activity. 123I-iomazenil single-photon emission computed tomography (SPECT) demonstrated reduced accumulation in the region (Figure 1B). A diagnosis of temporal lobe epilepsy (TLE) was established, and treatment with lacosamide at a dose of 100 mg/day resulted in a remarkable improvement in both symptoms and EEG findings. She has continued to make regular outpatient visits. Six months have passed without any recurrence of visual field symptoms, and she wishes to continue treatment.
Discussion
We report a case of an elderly patient with TLE. The diagnostic rationale is supported by the concordance among EEG findings, brain structural findings of MRI (hippocampal atrophy) [3], and findings of brain functional imaging (SPECT) [4]. Additionally, the rapid improvement of symptoms and epileptic findings of EEG following the introduction of anti-seizure medication also supported the diagnosis of the present patient. Therefore, we believe that this condition was consistent with temporal lobe epilepsy in the elderly, even though the patient did not present with seizure-typical symptoms specific to TLE.
It is possible that the patient had a relatively mild degree of FIAS, and thus the degree of impairment was small, and the patient was describing a sensation of uncertainty between the self and the outside world as ophthalmologic abnormalities. Additionally, our case presumably had focal seizures repeatedly. Thus, the patient did not report the symptoms as a "transient" phenomenon by herself, making it challenging for the clinician to include epileptic seizures in the differential at the initial visit.
The MRI of this case was notable in that it showed significant atrophy in the medial temporal lobe, with left-sided predominance. However, it is unlikely that such brain atrophy would occur within a two-month period following the onset of epileptic seizures. Moreover, there were no obvious symptoms of dementia in this case. Thus, it is possible that the long-term repetition of focal seizures, of which the patient was unaware, might have caused chronic brain atrophy.
The clinical course of this case appears to have been somewhat subacute. From this point of view, autoimmune epilepsy enters the differential as the etiology of temporal lobe epilepsy in this case. However, autoimmune epilepsy generally has a more complex seizure pattern and is often associated with impaired consciousness and higher brain dysfunction [5]. Considering the scoring as a diagnostic screening for autoimmune epilepsy [6], it was not necessary to actively consider autoimmune mechanisms in this case.
Epilepsy is most prevalent among the elderly [7]. In Japan, the prevalence of epilepsy in this demographic is on the rise due to the rapid expansion of the geriatric population. Reports indicate that the prevalence of epilepsy in individuals over the age of 65 surpasses 1% of the general population [8]. Approximately half of the initial seizures in the elderly are focal seizures with impaired consciousness, lacking convulsions; about 40% are generalized seizures (evolving from focal to bilateral tonic-clonic seizures); and less than 10% are characterized as generalized seizures such as myoclonic seizures. Older adults often encounter difficulties in accurately describing their symptoms [9]. The variation in seizure types demands close attention. Although epileptic seizures significantly impact the elderly both physically and psychologically, antiepileptic drugs are highly effective when the condition is accurately diagnosed and treated [10]. In Japan's hyper-aged society, comprehending the pathophysiology, diagnosis, and management of epilepsy in elderly patients holds critical importance, both from clinical and social perspectives.
Conclusions
The number of elderly patients with epilepsy is increasing, and temporal lobe epilepsy is becoming a common disorder in the treatment of the elderly. On the other hand, elderly patients may not present with the typical form of FIAS, or their complaints may be nonspecific, such as visual field abnormalities, as shown in our case. Therefore, clinicians should note that FIAS in elderly-onset TLE may not cause impairment of consciousness. Thus, imaging tests and EEG should be used to further the diagnosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Temporal lobe epilepsy semiology Epilepsy Res Treat Blair RD 751510201220122295724110.1155/2012/751510 PMC 3420439 · doi ↗ · pubmed ↗
- 2Temporal lobe epilepsy and Alzheimer’s disease: from preclinical to clinical evidence of a strong association J Alzheimers Dis Rep Tombini M Assenza G Ricci L 243261520213411378210.3233/ADR-200286 PMC 8150253 · doi ↗ · pubmed ↗
- 3Detection of hippocampal atrophy in patients with temporal lobe epilepsy: a 3-Tesla MRI shape Epilepsy Behav Mumoli L Labate A Vasta R 4894932820132389257910.1016/j.yebeh.2013.05.035 · doi ↗ · pubmed ↗
- 4SPECT imaging of epilepsy: an overview and comparison with F-18 FDG PET Int J Mol Imaging Kim S Mountz JM 813028201120112178572210.1155/2011/813028 PMC 3139140 · doi ↗ · pubmed ↗
- 5Autoimmune epilepsy - novel multidisciplinary analysis, discoveries and insights Front Immunol Levite M Goldberg H 7627431220213509584110.3389/fimmu.2021.762743 PMC 8790247 · doi ↗ · pubmed ↗
- 6Neurological autoantibody prevalence in epilepsy of unknown etiology JAMA Neurol Dubey D Alqallaf A Hays R 3974027420172816632710.1001/jamaneurol.2016.5429 · doi ↗ · pubmed ↗
- 7Seizure disorders: the changes with age Epilepsia Hauser WA 01433 Suppl 4199210.1111/j.1528-1157.1992.tb 06222.x 1425495 · doi ↗ · pubmed ↗
- 8Prevalence of adult epilepsy in a general Japanese population: the Hisayama study Epilepsia Open Tanaka A Hata J Akamatsu N 182186420193086812910.1002/epi 4.12295 PMC 6398097 · doi ↗ · pubmed ↗