Platypnea-Orthodeoxia Syndrome and COVID-19 Successfully Treated With Percutaneous Patent Foramen Ovale Closure: A Report of Two Cases and Literature Review
Fernando Jiménez-Segovia, Sara Luis-García, Candela González-San Narciso, Pablo Demelo-Rodríguez, Rita García-Martínez, Francisco Galeano-Valle

TL;DR
Two patients with severe COVID-19 and a rare breathing condition were successfully treated by closing a heart defect called patent foramen ovale.
Contribution
This is the first report of successful PFO closure during acute COVID-19 in patients with platypnea-orthodeoxia syndrome.
Findings
PFO closure resolved platypnea-orthodeoxia syndrome in two patients with severe COVID-19.
Bubble echocardiography confirmed PFO with significant shunting in both cases.
PFO closure during acute COVID-19 was safe and effective in these patients.
Abstract
Platypnea-orthodeoxia syndrome (POS) is a rare clinical condition characterized by positional dyspnea and/or hypoxia. We report two cases of patients with COVID-19 bronchopneumonia with a torpid evolution. Due to clinical suspicion of POS, a diagnostic workup was performed, including a bubble echocardiography, which revealed a patent foramen ovale (PFO) with early and massive passage of bubbles to the left cavities. Both patients underwent percutaneous PFO closure with a resolution of POS. Here, we present the second and third cases of POS associated with PFO successfully closed during the acute phase of COVID-19. This suggests that PFO closure could be a potential treatment option for this condition.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
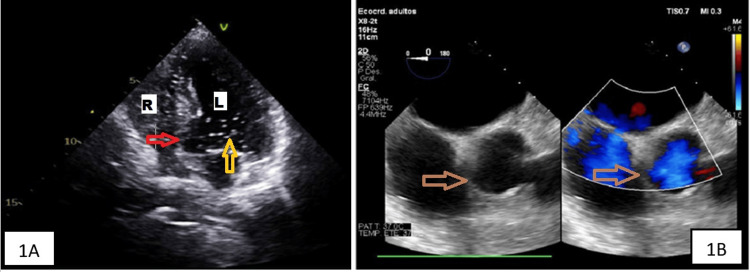 Figure 1
Figure 1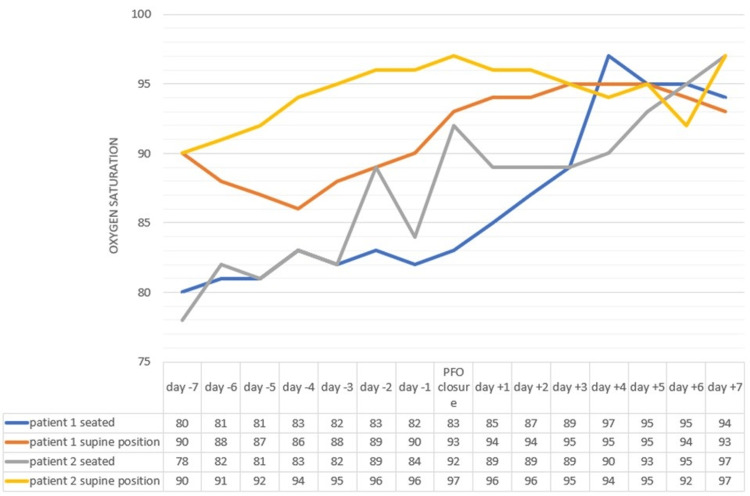 Figure 2
Figure 2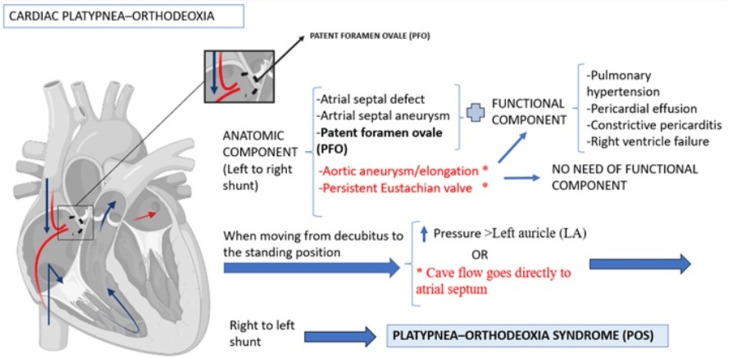 Figure 3
Figure 3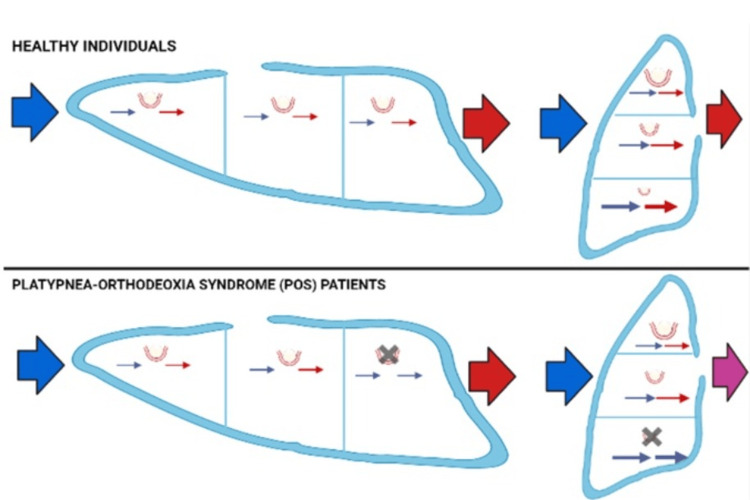 Figure 4
Figure 4| Author (year) (ref) | N | Gender | Mean age | Admission to the ICU | Oxygen support needed | Chest image | Echocardiography | Presence of PFO | PFO closure | Pulmonary embolism | Hepatopulmonary syndrome | Moment of diagnosis of POS | Treatment of POS |
| Tan et al. (2020) [ | 5 | 5/5 (100%) males | 65 (54-71) | 5/5 (100%) | IMV 5/5 (100%) | Ground glass opacities and consolidation in the posterior lung segments and lower lobes 5/5 (100%) | NA | NA | NA | 1/5 (20%) | - | During physiotherapy | Respiratory rehabilitation + supplemental oxygen. POS resolved over a median of 17 days |
| Tham et al. (2020) [ | 2 | 2/2 (100%) males | 69 and 63 | 2/2 (100%) | IMV 1/1 (50%). High-flow nasal cannula 1/1 (50%) | Patchy air space opacities and ground-glass attenuation of both lungs | 2/2 (100%) normal | 0 | 0 | 0 | 1/2 (50%) possible liver cirrhosis | During the commencement of rehabilitation, 18 and 9 days, respectively, after admission to the ICU | Respiratory rehabilitation + supplemental oxygen. POS resolved after 65 and 22 days respectively from the day of detection |
| Singh et al. (2020) [ | 1 | Male | 66 | 1 | IMV | Bilateral peripheral ground-glass opacities in both upper and lower zones | Normal | 0 | 0 | NA | - | During the commencement of rehabilitation | Physiotherapy and intermittent oxygen therapy via cannula nasal at 2 L O2. POS improved after 7 days of physiotherapy and the patient was discharged on room air after 15 days of hospitalization |
| Siddique et al. (2021) [ | 1 | Male | 45 | 0 | High-flow nasal cannula | Bronchopneumonia + pneumomediastinum | Yes. R-L shunt | 0 | 0 | 0 | - | NA | Oxygen therapy. POS remained |
| Oldani et al. (2021) [ | 1 | Male | 80 | 0 | CPAP High-flow nasal cannula | Bilateral peripheral ground-glass opacities in lower zones | NA | NA | NA | NA | NA | 18 days after the onset of COVID-19 | NA |
| Vanhomwegen et al. (2021) [ | 1 | Male | 55 | 0 | Oxygen therapy and Boussignac continuous positive airway pressure | Bilateral peripheral ground glass opacities with crazy paving patterns | Yes. PFO | 1 | 0 | NA | - | Three weeks after hospital admission | Oxygen therapy. Two weeks after discharge, POS disappeared |
| Kramer et al. (2021) [ | 1 | Male | 73 | 1 | IMV | Bilateral opacities. | Yes. PFO | 1 | 1 | 0 | - | During rehabilitation | PFO closure. No need for oxygen therapy when discharged |
| Hoshi et al. (2021) [ | 1 | Woman | 73 | 0 | OxyMaskTM (Southmedic Inc., Barrie, ON, Canada) at 7 L/min | Bilateral and peripheral predominant consolidation and an air bronchogram | Normal | 0 | 0 | NA | - | During the commencement of rehabilitation | Respiratory rehabilitation. The patient was discharged under home oxygen therapy with 0.5 L/min via a nasal cannula 28 days after admission |
| Dodson et al. (2021) [ | 1 | Male | 85 | 0 | High-flow nasal cannula | Consolidation and ground-glass opacities involving most of the left lung | Yes. PFO and atrial septum aneurysm | 1 | 0 | NA | - | 28 days after the diagnosis of COVID-19. | Graded progression to standing and supplemental oxygen increases when upright. The patient was discharged and his oxygen requirement was resolved on approximately day 78 |
| Zanoni et al. (2022) [ | 1 | Woman | 76 | 0 | Oxygen therapy, CPAP | Bilateral ground-glass opacities. + pneumomediastinum and fibrosis | Normal | 0 | 0 | 1 | - | Approximately 1 month after the diagnosis of COVID-19 | Oxygen therapy, diuretics, anticoagulant therapy, azithromycin. POS remained |
| Aprea et al. (2022) [ | 1 | Woman | 82 | 0 | CPAP high-flow nasal cannula PSV | Moderate to severe interstitial lung involvement is greater at the lung bases | Normal | 0 | 0 | 0 | - | On the third day of hospital admission | Respiratory rehabilitation + supplemental oxygen. Discharge on day 18 |
| Asami-Noyama et al. (2022) [ | 1 | Male | 83 | 0 | High-flow nasal cannula | Bilateral ground-glass opacities | Normal | 0 | 0 | NA | - | 1 month after the diagnosis of COVID-19 | Gradual improvement in oxygenation. POS remained |
| Yowesgaran et al. (2022) [ | 1 | Woman | 63 | 0 | NA | NA | Yes. PFA | 1 | 1 | 0 | - | 1 year after the diagnosis of COVID-19 | PFA closure. No need for oxygen therapy when discharged |
| Jiménez-Segovia et al. (2024) (current case report) | 2 | 2/2 (100%) Women | 74 and 61 | 1/2 (50%) | 1/2 (50%) IMV. 1/2 (50%) low-flow oxygen therapy | Bilateral peripheral interstitial opacities compatible with bronchopneumonia | Yes. 2/2 (100%) PFA | 2 | 2 | 1/2 (50%) | - | During the rehabilitation sessions | PFA closure. No need for oxygen therapy when discharged |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and Diving-Related Complications · Respiratory Support and Mechanisms · Restraint-Related Deaths
Introduction
Platypnea-orthodeoxia syndrome (POS) is a rare clinical condition characterized by the appearance or worsening of hypoxemia (orthodeoxia) and dyspnea (platypnea) when moving from the supine position to the upright position of the trunk [1]. Hypoxemia is considered significant when there is a decrease in PaO2 of at least 4 mmHg or an oxygen desaturation of at least 5% upon transitioning from a supine position to sitting or standing [2].
The pathophysiology of POS is based on the mixing of venous blood with arterial blood through a connecting pathway or shunt, which can be intracardiac (e.g., patent foramen ovale (PFO)) or extracardiac (e.g., pulmonary arteriovenous fistula). For this to occur, therefore, a right-to-left shunt is necessary. In addition, a functional component that favors the R-L shunt is necessary when the patient passes from the decubitus position to the orthostatic position [2].
Since the beginning of the SARS-CoV-2 pandemic, a few cases of POS have been reported, and some authors have suggested that bronchopneumonia can cause an imbalance in ventilation/perfusion (V/P) that favors shunting in patients with PFO [3].
Here, we present two new cases of patients diagnosed with SARS-CoV-2 infection who subsequently developed POS due to a PFO. Additionally, we perform a narrative review of the literature on this topic.
Case presentation
Case 1
A 74-year-old woman had a history of liver cirrhosis due to hepatitis B virus infection (without portal hypertension), intrinsic asthma, and mild pulmonary hypertension. She attended the emergency department in October 2020 due to fever, muscle pain, and dyspnea. Upon arrival, blood pressure was 122/78 mmHg, heart rate was 104 bpm, oxygen saturation was 88%, and temperature was 98.96ºF. The reverse transcriptase polymerase chain reaction (RT-PCR) for SARS-CoV-2 was positive. The chest X-ray showed bilateral bronchopneumonia. Blood analysis disclosed lymphocytes 0.5 103/μL (1.3-3.5 103/μL), fibrinogen 799 mg/dL (200-600 mg/dl), D-dimer 408 ng/mL (0-250 ng/ml), Nt-pro BNP 1017 ng/L (0-300 ng/L), C-reactive protein 18.5 mg/dL (<0.4 mg/dl), and ferritin 1094 μg/L (22-274 μg/L).
The patient received treatment with dexamethasone and low-flow oxygen therapy. During the first two weeks of admission, the clinical condition improved slowly, but the chest X-ray only showed radiologically mild improvement. During the rehabilitation sessions, she presented episodes of oxygen desaturation (a decrease from 96% to 85%) and dyspnea when she was sitting, improving when she was in the supine position. A bubble contrast echocardiogram demonstrated the early and massive passage of bubbles to the left cavities, confirming the diagnosis of PFO (Figure 1A). In addition, it showed an atrial septum aneurysm with 1 cm of separation. A right heart catheterization showed a pulmonary capillary wedge pressure of 7 mmHg (4-12 mmHg) and a mean pulmonary artery pressure of 28 mmHg (<20 mmHg). Percutaneous closure was performed by means of an interatrial device with resolution of platypnea and orthodeoxia (Figure 2), allowing the patient to be discharged without oxygen therapy.
1A: Bubble echocardiogram demonstrating early and massive passage of bubbles from right to left cavities, suggesting intracavitary shunt compatible with the diagnosis of PFO in patient 1. 1B: PFO visible through transesophageal echocardiographyR: right cavities, L: left cavities, PFO: patent foramen ovale, red arrow: PFO, yellow arrow: bubbles in left cavities, brown arrow: PFO visible through transesophageal echocardiography
Oxygen saturation levels during hospitalization of patients 1 and 2PFO: patent foramen ovale
Case 2
A 61-year-old woman with no relevant personal history presented to the ED in March 2020 due to fever and dyspnea. Upon arrival, blood pressure was 103/69 mmHg, heart rate 112 bpm, oxygen saturation 84%, and temperature 102.2ºF. A nasopharyngeal swab RT-PCR for SARS-CoV-2 was positive. A chest X-ray showed bilateral bronchopneumonia, and blood analysis revealed: leukocytes 18.70 103/µL (4-10 103/µL), neutrophils 17.5 103/µL (1.8-7.5 103/µL), lymphocytes 0.9 103/µL (1.3-3.5 103/µL), INR 1.4 (0.8-1.2), fibrinogen >1000 mg/dL (200-600 mg/dl), D-dimer 654 ng/mL (0-250 ng/ml), procalcitonin 3.12 µg/L (0-0.5 µg/L), and C-reactive protein 59.3 mg/dL (<0.4 mg/dl).
The patient's respiratory condition worsened despite treatment with dexamethasone and high-flow oxygen therapy. A chest CT showed a bilateral subsegmental pulmonary embolism, and the patient was admitted to the critical care unit for invasive mechanical ventilation. After clinical stabilization (one month later), she was transferred back to the conventional hospital ward, where she developed typical symptoms of POS. During rehabilitation sessions, she presented episodes of oxygen desaturation and dyspnea that improved when she was in the supine position. A repeated chest CT showed signs of organized pneumonia, and a transesophageal echocardiogram revealed a PFO (Figure 1B). The PFO was successfully closed percutaneously, leading to clinical improvement in the patient (Figure 2).
Discussion
We present two cases of POS in patients with a previously asymptomatic PFO in the setting of SARS-CoV-2 pneumonia, successfully treated with percutaneous PFO closure.
The true incidence of POS is uncertain. POS requires two elements: on the one hand, an interatrial shunt (e.g.., PFO, an atrial septal defect, an atrial septal aneurysm, an aortic aneurysm/elongation, a persistent Eustachian valve) or an intrapulmonary shunt (e.g., hepatopulmonary syndrome in the context of cirrhosis, arteriovenous malformations in Rendu-Osler-Weber syndrome, or parenchimal lung diseases such as intersticial pneumonia, Pneumocystis jirovecii pneumonia, thoracic trauma, acute respiratory distress syndrome, pulmonary fibrosis, chronic obstructive pulmonary disease, and obstructive pneumonia such as bronchogenic or laryngeal carcinoma). On the other hand, a functional component is necessary that favors the R-L shunt when the patient changes position from supine to orthostatic. The functional component includes cardiac and pulmonary conditions. These conditions are proposed to cause transient elevations in right atrial pressures in the upright position. This reverses the pressure gradient across the intracardiac defect, which leads to an R-L shunt. Such a clinical scenario occurs in hypoxic lung diseases (e.g., pulmonary embolism), decreased right-sided compliance (e.g., right ventricular ischemia), or those associated with high right-sided filling pressures (e.g., myxoma of the right atrium or pericardial effusion) (Figure 3-4) [2,4].
Mechanisms of cardiac platypnea-orthodeoxiaImage Credit: Author
Mechanisms of pulmonary platypnea-orthodeoxia. V/Q and shunt in healthy individuals and in patients with POSParenchymal lung diseases such as emphysema, interstitial lung disease, or consolidation with preferential involvement of lung bases can occasionally present as POS through severe V/Q mismatch, as discussed below. Pulmonary blood flow distribution is heterogeneous due to gravity. Gravity increases the blood flow in the lung bases more than in the apical regions, a phenomenon that is accentuated in upright positions. In addition, when standing upright, the right ventricular preload reduces, causing decreased output to the pulmonary arteries. This results in alveolar pressure exceeding pulmonary arterial and venous pressures at the lung apex. The lung apices tend to act as dead space in an upright position and contribute to an increase in V/Q mismatch and increased dyspnea, the so-called zone I phenomenon [5]. Lung diseases such as COVID-19 involve mostly the bases and posterior areas of the lung, causing intrapulmonary shunting and accentuating the V/Q mismatch.Blue arrow: deoxygenated blood, red arrow: oxygenated blood, purple arrow: mix of deoxygenated and oxygenated blood, black cross: interstitial disease, V/Q: ventilation/perfusion, POS: platypnea-orthodeoxia syndromeImage Credit: Author
The first patient had pulmonary conditions (cirrhosis, intrinsic asthma, mild pulmonary hypertension, and acute respiratory distress syndrome in the context of COVID-19 pneumonia), and the interatrial shunt was confirmed: a PFO associated with ascending aortic aneurysm (it is the most frequent coadjuvant anatomical alteration). Intracardiac POS can be seen in patients with aortic aneurysm, aortic root dilatation, and aortic elongation in patients with an atrial septal aneurysm [2,6]. The second patient had a pulmonary condition (acute respiratory distress syndrome in the context of COVID-19 pneumonia and the development of pulmonary embolism), and the interatrial shunt was a PFO as well.
The overall incidence of PFO was 27.3%, but it progressively declined with increasing age, from 34.3% during the first three decades of life to 25.4% during the fourth through eighth decades and to 20.2% during the ninth and 10th decades, with the vast majority being asymptomatic [7]. However, it can manifest as POS, or paradoxical embolism, in some cases. Its diagnosis requires an echocardiogram with agitated saline contrast showing an early passage of bubbles. The appearance of bubbles in the left atrium within three cardiac cycles suggests an intracardiac shunt [8]. In suspected POS cases, it should ideally be performed dynamically, first with the patient in a decubitus position and then repeated with the patient in a seated position. In cases of high suspicion with an indeterminate echocardiographic study, cardiac magnetic resonance imaging may be used to look for distortion of the cardiac anatomy leading to R-L shunting [9].
In patients with SARS-CoV-2 pneumonia, involvement of the lower and posterior zones of the pulmonary parenchyma and gravitational shunts of blood in the lower zones are frequent, hindering proper ventilation. This situation is aggravated by the presence of microthrombosis and microangiopathy observed in cases of severe infection [3], as was confirmed in the second patient. Patients with SARS-CoV-2 pneumonia present variable degrees of pulmonary fibrosis and respiratory dysfunction. Lung lesions caused by SARS-CoV-2 are often located in the subpleural area of the lower lobes of both lungs, as was the case in our first patient. Since gravity causes blood flow to be directed to the lung bases, the apical lung areas show increased ventilatory dead space. Thus, basal parenchymal involvement may worsen this physiological imbalance of ventilation and perfusion, precipitating POS [3]. Furthermore, although SARS-CoV-2 pneumonia predominantly affects the basal lung segments of both lungs, it is not clear why POS is only present in rare cases of SARS-CoV-2 pneumonia [3]. Although both of our patients had an anatomic component (PFO), the syndrome only manifested after SARS-CoV-2 pneumonia, suggesting that the infection may have played a role in the development of POS (Figures 3-4).
We conducted a literature search in January 2023 using PubMed and Scopus. We searched for articles using the terms "platypnea-orthodeoxia syndrome," "COVID-19," "SARS-COV-2," "patent foramen ovale," "persistent foramen ovale," and "intracardiac shunt" in English. Thirteen results were screened for eligibility, and among them, 11 articles were single case reports, while two articles were case series of two and five patients, respectively. These cases are summarized in Table 1.
The majority of POS cases associated with COVID-19 were described in men (14/18 patients) older than 60 years old [10-12,14,16,17,20]. This may be explained because the development of POS seems to be associated with severe COVID-19, which is more frequent in men and the elderly. Besides, most cases required admission to the ICU and invasive mechanical ventilation [10-12,16].
Most cases of POS were diagnosed during rehabilitation sessions when the patient was moved from the supine position to the upright position, as was the case with our patients. PFO was confirmed in four out of 12 patients who underwent echocardiography [15-17,21]. Almost all these cases were diagnosed during the acute phase of the SARS-CoV-2 infection, as was the case with our patients. However, in one case [21], the diagnosis of POS was made one year after the diagnosis of COVID-19 due to the persistence of dyspnea. It is also noteworthy that in one case [17], the patient presented an atrial septal aneurysm, as was seen in our first case.
On the other hand, when we analyzed the rate of pulmonary embolism, we found only two cases [10,18]. This number may be underestimated if we consider that microthrombosis is one of the mechanisms that could also play a role in the development of POS in COVID-19, as it occurred in our second patient. One of the previous cases [11] had cirrhosis, and a possible hepatopulmonary syndrome was also postulated as one of the mechanisms contributing to POS in COVID-19.
In the aforementioned articles, the main mechanism suggested for POS is a ventilation-perfusion mismatch within the lesions of COVID-19 pneumonia. This mismatch is exacerbated by other conditions mentioned above, such as pulmonary embolism or hepatopulmonary syndrome.
The treatment applied in previous cases of POS secondary to SARS-CoV-2 pneumonia was respiratory rehabilitation and oxygen therapy, showing a variable degree of efficacy but with good results in most cases [10-12,15-17,21]. However, in three of the aforementioned articles, POS remained [13,18,20]. In two of the four previous cases of PFO and COVID-19 [15,17] respiratory rehabilitation and supplemental oxygen were enough, but the closure of the PFO was not pursued. The ACC/AHA guidelines recommend ASD closure in patients with RA and right ventricular enlargement (Class I). Smaller ASDs (diameter <5 mm) with no evidence of right ventricular enlargement or pulmonary hypertension do not require closure unless they are associated with POS or paradoxical embolism (Class IIa) [22]. However, in the other two cases [16,21], the PFO closure was necessary since respiratory rehabilitation was not effective with good results. A 10-20% increase in upright oxygen saturation has been reported after the corrective surgery [23]. Nevertheless, only in one case [16] was the closure of the PFO successfully performed during the acute phase of COVID-19. Therefore, we present the second and third cases of POS linked to PFO, whose closure was also made successfully during the acute phase of COVID-19; this could be a possible treatment in those patients with PFO and COVID-19 who do not respond to conservative management.
Conclusions
We present two rare cases of POS and COVID-19, successfully treated with percutaneous PFO closure. In COVID-19 patients who do not evolve favorably, the diagnosis of POS should be considered and PFO should be ruled out. In confirmed cases, PFO closure may be an effective treatment to improve the respiratory situation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Platypnea (diffuse zone I phenomenon?)N Engl J Med Altman M Robin ED 134713482811969535543910.1056/NEJM 196912112812408 · doi ↗ · pubmed ↗
- 2Platypnea-orthodeoxia syndrome and Budd-Chiari syndrome: an unreported association (Article in Spanish)Med Clin (Barc) Demelo-Rodríguez P Del Toro-Cervera J 949514420152476820210.1016/j.medcli.2014.03.008 · doi ↗ · pubmed ↗
- 3Platypnea-orthodeoxia syndrome associated with COVID-19 pneumonia: a case report JA Clin Rep Hoshi T Tadokoro Y Nemoto M Honda J Matsukura S 67720213446747310.1186/s 40981-021-00471-7PMC 8407127 · doi ↗ · pubmed ↗
- 4Cardiac platypnea-orthodeoxia syndrome: an often unrecognized malady Clin Cardiol Knapper JT Schultz J Das G Sperling LS 6456493720142491200410.1002/clc.22301 PMC 6649356 · doi ↗ · pubmed ↗
- 5Distribution of pulmonary perfusion in erect man J Appl Physiol Anthonisen NR Milic-Emili J 760766211966591274510.1152/jappl.1966.21.3.760 · doi ↗ · pubmed ↗
- 6Hypoxaemia associated with an enlarged aortic root: a new syndrome?Heart Eicher JC Bonniaud P Baudouin N 103010359120051576104610.1136/hrt.2003.027839 PMC 1769048 · doi ↗ · pubmed ↗
- 7Incidence and size of patent foramen ovale during the first 10 decades of life: an autopsy study of 965 normal hearts Mayo Clin Proc Hagen PT Scholz DG Edwards WD 1720591984669442710.1016/s 0025-6196(12)60336-x · doi ↗ · pubmed ↗
- 8The use of contrast echocardiography for the detection of cardiac shunts Eur J Echocardiogr Soliman OI Geleijnse ML Meijboom FJ 2128200710.1016/j.euje.2007.03.00617462958 · doi ↗ · pubmed ↗