A Rare and Intriguing Case Report of Metaplastic Breast Carcinoma
Vallal Kani, Vimal Chander, Sulochana Sonti, Sridevi Manian, Sudha Vasudevan, Muthuvel Esakki, Sarah Grace Priyadarshini, Karthika Rajendran

TL;DR
This paper presents a rare case of metaplastic breast carcinoma, a fast-growing and aggressive form of breast cancer that is difficult to diagnose and has a poor prognosis.
Contribution
The novelty lies in reporting a rare and complex case of metaplastic breast carcinoma to raise awareness among clinicians.
Findings
Metaplastic breast carcinoma has both epithelial and mesenchymal components and grows rapidly.
It is harder to diagnose than invasive ductal carcinoma and has worse survival outcomes.
Rapidly growing breast masses should be evaluated for metaplastic or sarcomatoid malignancies.
Abstract
Metaplastic breast carcinoma (MBC) is a rare and aggressive subtype of breast cancer characterized by the presence of both epithelial and mesenchymal components within the tumor. Its clinical and radiological appearance is comparable to other types of breast cancer, but it grows rapidly. The diagnosis of metaplastic carcinoma is largely based on the epithelial origin of the cells confirmed by immunohistochemistry (IHC). Compared to invasive ductal carcinoma, metaplastic carcinoma has a worse overall survival rate. Any patient with a rapidly growing breast mass should be assessed with suspicion of sarcomatoid or metaplastic malignant neoplasm. We report this case due to its rarity and the complex nature of the disease.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
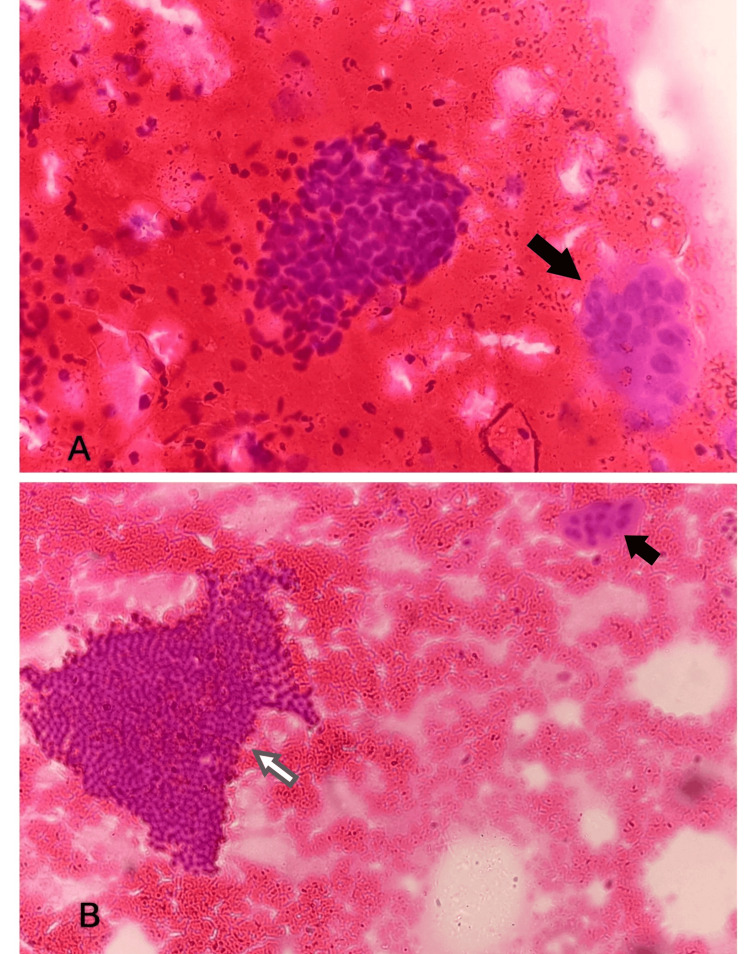 Figure 1
Figure 1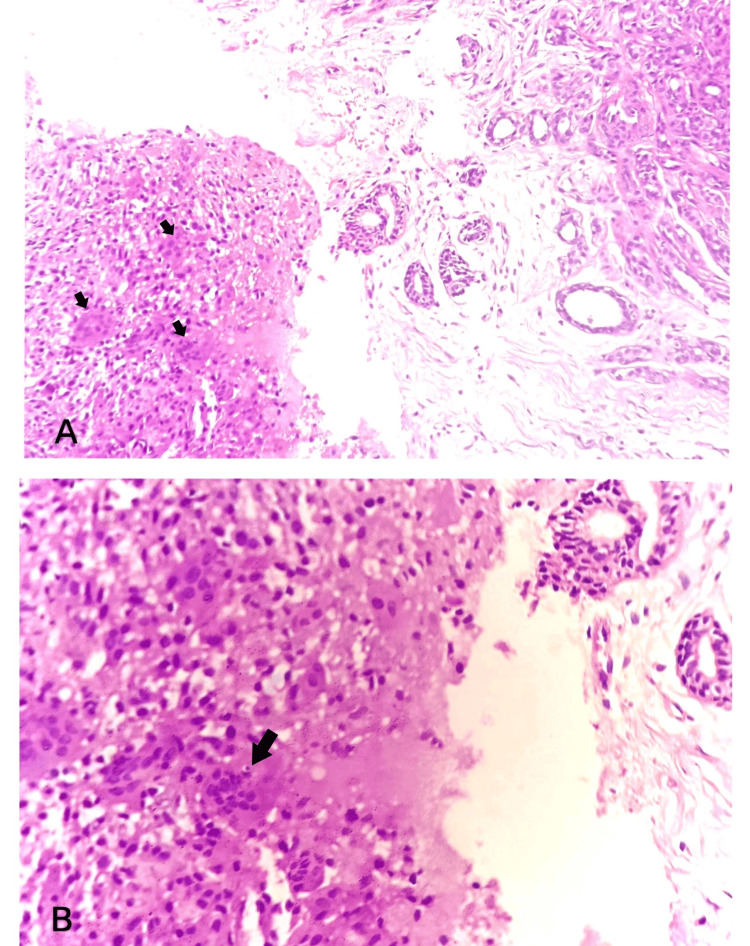 Figure 2
Figure 2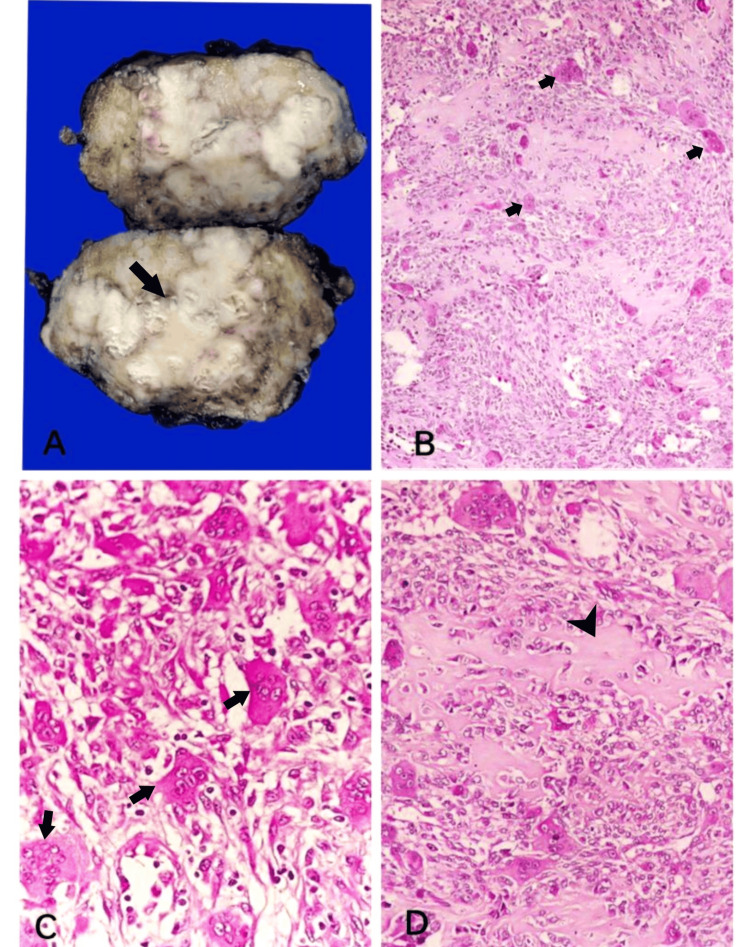 Figure 3
Figure 3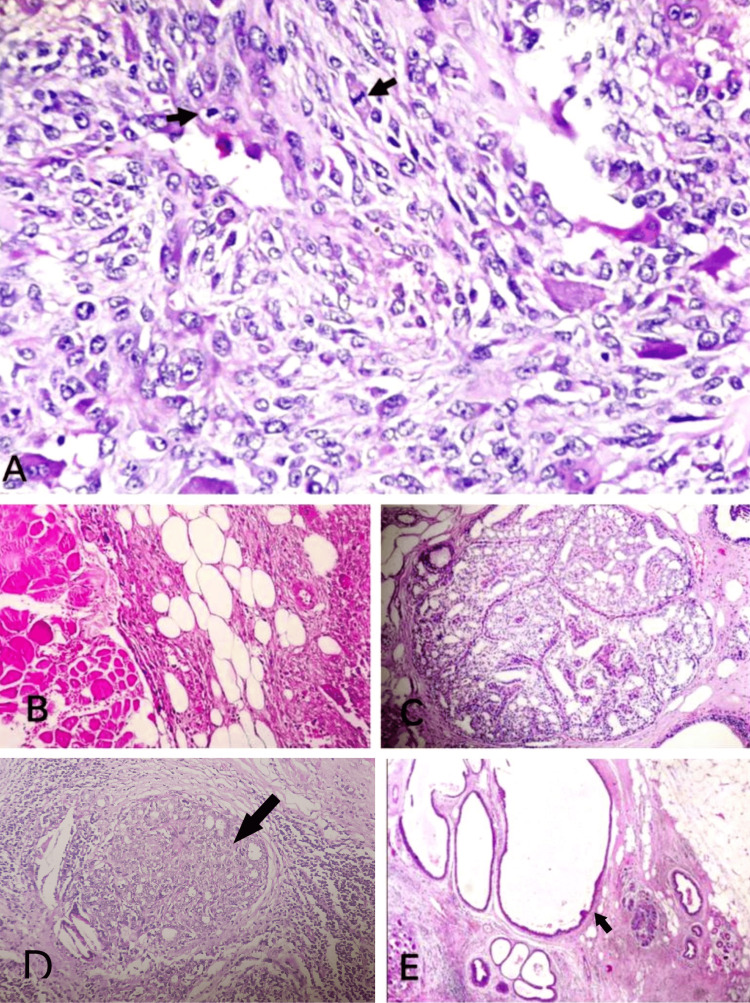 Figure 4
Figure 4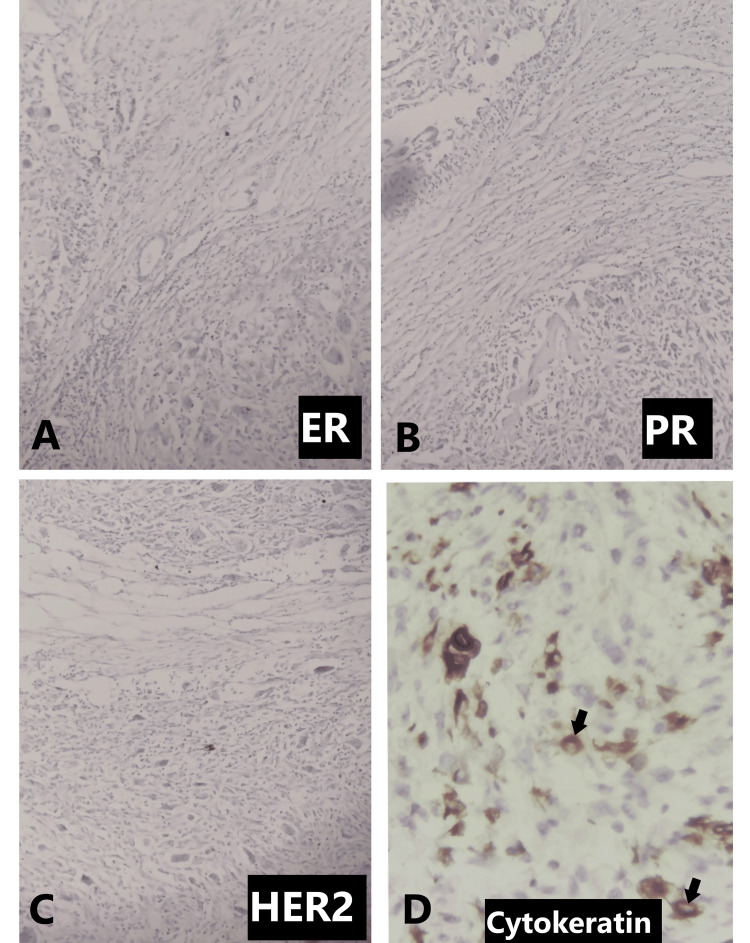 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Lesions and Carcinomas · Breast Cancer Treatment Studies · Cancer and Skin Lesions
Introduction
Metaplastic breast carcinoma (MBC) stands as a rare and distinct aggressive subtype of breast cancer, characterized by its unique histological features and challenging clinical management. Its incidence is 0.2-5% of all cancers of the breast and has the worst prognosis when compared to other forms of the disease, leading to the major cause of mortality due to breast carcinoma globally [1]. In 1973, Huvos and associates published the first publication introducing the term metaplastic carcinoma [1,2]. In this article, we report a case of metaplastic breast carcinoma in a 44-year-old female.
Case presentation
A 44-year-old female has been complaining of a lump in the right breast for the past four months, associated with pain. On examination, a 7x6 cm swelling was noted in the right breast, and with a clinical diagnosis of fibroadenoma, fine needle aspiration and trucut biopsy followed by an excision biopsy were performed. In fine needle aspiration cytology (FNAC), the smears were moderately cellular and showed branching papillary fronds, monolayered sheets, clusters of ductal epithelial cells with interspersed myoepithelial cells, a few bare nuclei, occasional clusters of apocrine cells, multinucleated giant cells, and a few anucleate squames in a background of hemorrhage. The smears studied showed no evidence of malignancy (Figures 1A, 1B). Hence, a diagnosis suggestive of fibroadenoma with focal foreign body giant cell reaction was given.
Fine needle aspiration cytologyA: Smear showing ductal epithelial cells and multinucleated giant cells (arrow); B: Monolayered sheets of ductal epithelial cells (white arrow) with multinucleated giant cells (black arrow)
In a subsequent trucut biopsy, we received multiple grey-white soft tissue fragments on aggregate measuring 0.8x0.5x0.2 cm, which microscopically showed breast parenchyma with glands lined by bilayered epithelium with focal areas of foreign body giant cell reaction. A few ducts showed epithelial hyperplasia without atypia. The sections studied showed no atypical cells or granulomas (Figures 2A, 2B). The report was given as features suggestive of benign breast disease with foreign body giant cell reactions.
Trucut biopsyA: Sections from trucut biopsy showing glands with multinucleated giant cells (arrows); B: Sections from trucut biopsy showing multinucleated giant cells (arrow)
Then an excision biopsy was done, and macroscopically, we received a cut-open single globular mass measuring 8x5x4 cm, and the cut surface showed grey-white to grey-brown areas (Figure 3A). On microscopy, multiple sections studied showed breast parenchyma with an infiltrating malignant neoplasm composed of sheets of cells with scant to moderate eosinophilic cytoplasm and elongated to spindle-shaped hyperchromatic, pleomorphic nuclei with brisk mitosis, along with numerous scattered osteoclastic types of multinucleated giant cells (Figures 3B, 3C). Focal areas showed eosinophilic osteoid separating the tumor cells along with necrosis and chondroid areas (Figure 3D). Numerous mitotic figures were noted (Figure 4A). The tumor cells were seen to invade the adipose tissue and adjacent breast parenchyma and skeletal muscle bundles in one focus (Figure 4B). Adjacent parenchyma showed dense hyalinization and fibrocystic change with focal usual ductal hyperplasia and low-grade ductal carcinoma in situ (Figures 4C-4E). Immunohistochemistry showed estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor 2 (HER2) negativity with 40% positivity of cytokeratin (Figures 5A-5D). Based on the above findings, a final diagnosis of metaplastic carcinoma (with predominant mesenchymal/osteosarcomatous patterns) was given. No lymph nodes were submitted.
Gross and microscopy of excision biopsyA: Gross specimen showing a globular mass with a grey-white cut surface (arrow); B: Breast parenchyma with an infiltrating malignant neoplasm and numerous multinucleated giant cells (arrows); C: Elongated to spindle-shaped tumor cells with numerous scattered osteoclastic types of multinucleated giant cells (arrows); D: Areas of eosinophilic osteoid (arrowhead) separating the tumor cells
MicroscopyA: Mitotic figures (arrows); B: Tumor cells invading the adipose tissue and adjacent breast parenchyma; C: Areas of usual ductal hyperplasia; D: Ductal carcinoma in situ component (arrow); E: Areas of fibrocystic change (arrow)
ImmunohistochemistryA: Immunohistochemistry showing ER negativity; B: Immunohistochemistry showing PR negativity; C: Immunohistochemistry showing HER2 negativity; D: Immunohistochemistry showing 40% cytokeratin positivity (arrows)
Then, an oncology opinion was obtained, which advised chemotherapy for eight cycles and planned revision surgery with a modified radical mastectomy. The patient was followed up, and she has completed two cycles of chemotherapy with Adriamycin and Cyclophosphamide and improved symptomatically.
Discussion
Metaplastic carcinomas are defined as including one or more populations of cells that have undergone metaplastic differentiation, or the transformation of glandular morphology into non-glandular morphological forms [3]. The metaplastic alterations consist of either carcinomatous (squamous) or sarcomatous (spindle, chondroid, and osseous) components [1]. Metaplastic breast carcinoma is classified as low-grade tumors, which include low-grade adenosquamous carcinoma and fibromatosis-like spindle cell carcinoma, followed by high-grade tumors, which include high-grade adenosquamous carcinoma and aggressive high-grade spindle cell carcinoma. Rarely intermediate-grade tumors, which include spindle cell metaplastic carcinoma, are also seen, as they behave with intermediate risk between low-grade and high-grade tumors. Two primary types of metaplastic breast carcinoma are observed in practice: tumors having both metaplastic and adenocarcinomatous elements that can overlap morphologically and tumors having specific metaplastic components (such as squamous, spindle cell, or matrix-producing tumors) [4]. The major reasons for false negative results in fine needle aspiration cytology and trucut biopsy are inappropriate sampling procedures, the incorrect site of the tumor, or the existence of a well-defined neoplasm with low atypia [5]. Most metaplastic breast carcinomas do not express the human epidermal growth factor 2 receptor (HER2), progesterone receptor (PR), or estrogen receptor (ER). Hence, they fall under triple-negative breast cancer (TNBC). Regretfully, the prognosis for metaplastic breast carcinoma is poorer than that of non-metaplastic triple-negative breast cancer; it has a twofold chance of recurrence and a lower overall and disease-free life [1]. The epithelial origin of metaplastic carcinoma is mostly dependent on demonstrating a positive expression of cytokeratin, at least focally on immunohistochemistry. It also stains for vimentin and smooth muscle actin [6,7]. Because metaplastic carcinoma is uncommon and heterogeneous, the best course of treatment has not been determined. Usually, treatment for it is comparable to that for a standard case of breast adenocarcinoma. In most studies, treatment consists of modified radical mastectomy and dissection of axillary nodes, together with chemotherapy and radiotherapy. The role of targeted therapy and conventional chemotherapy is limited by the lack of hormone receptor expression and the human epidermal growth factor 2 receptor (HER2). While post-mastectomy radiotherapy was linked to advantages in overall survival in the advanced stage but not in the early stage, post-lumpectomy radiotherapy was associated with greater overall survival in both the early and advanced stages of the carcinoma [6,8]. The significant predictors of survival include the duration of symptoms, stage of the tumor, size of the tumor, and status of axillary nodes [6].
Conclusions
This rare case report of metaplastic breast carcinoma underscores the importance of comprehensive diagnostic evaluation and individualized treatment approaches in managing uncommon breast malignancies. Despite its rarity, clinicians must maintain a high index of suspicion for metaplastic breast carcinoma when encountering atypical, rapidly growing breast lesions, especially in older patients with unique clinical presentations. Additionally, this case highlights the significance of multidisciplinary collaboration involving oncologists, pathologists, radiologists, and surgeons to ensure accurate diagnosis, optimal treatment planning, and favorable patient outcomes. Continued research efforts are warranted to further elucidate the pathogenesis, prognostic factors, and therapeutic strategies for this challenging subtype of breast cancer. Through diligent clinical observation, meticulous pathological assessment, and tailored therapeutic interventions, we can strive to improve our understanding and management of metaplastic breast carcinoma, ultimately enhancing the quality of care and outcomes for affected individuals.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A comprehensive overview of metaplastic breast cancer: clinical features and molecular aberrations Breast Cancer Res Reddy TP Rosato RR Li X Moulder S Piwnica-Worms H Chang JC 121222020 https://breast-cancer-research.biomedcentral.com/articles/10.1186/s 13058-020-01353-z?fbclid=Iw AR 1LP Sxl Kl W 3l Efjrt Vv Up 0Pt SZTQQ Jic Am 11E 20Sy 7Z 0-m 6tp EMY 9TOV-03314828810.1186/s 13058-020-01353-z PMC 7640663 · doi ↗ · pubmed ↗
- 2Metaplastic carcinoma of the breast: analysis of 38 cases from a single institute Turk Patoloji Derg Hasbay B Aka Bolat F AytaçHÖ Aslan H Purbager A 2330362020 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 10512683/#ref-33176949910.5146/tjpath.2019.01472 PMC 10512683 · doi ↗ · pubmed ↗
- 3Metaplastic carcinoma of the breast: report of three cases Cancer: Interdisciplinary International Journal of the American Cancer Society Brenner RJ Turner RR Schiller V Arndt RD Giuliano A 10821087821998 https://acsjournals.onlinelibrary.wiley.com/doi/full/10.1002/%28SICI%291097-0142%2819980315%2982%3A 6%3C 1082%3A%3AAID-CNCR 11%3E 3.0.CO%3B 2-29506353 · pubmed ↗
- 4An update on the pathological classification of breast cancer Histopathology Rakha EA Tse GM Quinn CM 516822023 https://onlinelibrary.wiley.com/doi/full/10.1111/his.147863648227210.1111/his.14786 PMC 10108289 · doi ↗ · pubmed ↗
- 5Fine needle aspiration cytology of the breast: the nonmalignant categories Patholog Res Int Mendoza P Lacambra M Tan PH Tse GM 54758020112011 https://downloads.hindawi.com/archive/2011/547580.pdf 2166027510.4061/2011/547580 PMC 3108472 · doi ↗ · pubmed ↗
- 6Metaplastic carcinoma of the breast- case report and review of literature Int Journal Surg Open Kumar M Nigam JS Khanna P Arora A 4346242020 https://www.sciencedirect.com/science/article/pii/S 2405857220300176
- 7Spindle cell (sarcomatoid) carcinoma of the breast: a clinicopathologic and immunohistochemical analysis of 29 cases Am J Surg Pathol Carter MR Hornick JL Lester S Fletcher CD 300309302006 https://journals.lww.com/ajsp/abstract/2006/03000/spindle_cell__sarcomatoid__carcinoma_of_the.2.aspx 1653804910.1097/01.pas.0000184809.27735.a 1 · doi ↗ · pubmed ↗
- 8Metaplastic breast cancer: practice patterns, outcomes, and the role of radiotherapy Ann Surg Oncol Haque W Verma V Naik N Butler EB Teh BS 928936252018 https://link.springer.com/article/10.1245/s 10434-017-6316-210.1245/s 10434-017-6316-229322287 · doi ↗ · pubmed ↗