Thinking and Enacting the Patient Medical Home Under Pandemic Conditions: A Qualitative Study From Primary Care in Alberta, Canada
Myles Leslie, Brian Hansen, Rida Abboud, Caroline Claussen, Fariba Aghajafari

TL;DR
This study explores how primary care teams in Alberta, Canada used the Patient Medical Home model to respond to the challenges of the COVID-19 pandemic.
Contribution
The paper provides new insights into how the Patient Medical Home model supported pandemic response through patient-centered and team-based care.
Findings
The PMH model helped ensure access to care and address social determinants of health during the pandemic.
Healthcare teams adapted and expanded their services to meet the evolving needs of their communities.
The PMH model enabled a patient-centered and team-based approach to delivering primary health care during the crisis.
Abstract
The COVID-19 (C19) pandemic shocked primary care systems around the world. Those systems responded by supporting patients in the community, and acute care facilities in crisis. In Canada, the Patient Medical Home (PMH) is a widely adopted care model that aims to operationalize the tenets and principles of Primary Health Care (PHC) as developed since the Alma-Ata Declaration. This paper describes how personnel working in and with Primary Care Networks (PCNs) in Alberta, Canada deployed the PMH model and its underlying PHC principles to frame and respond to the C19 shock. Using purposive and snowball sampling techniques, we interviewed 57 participants who worked in public health and primary care, including community-based family physicians. We used interpretive description to analyze the interviews. PCN staff and physicians described how the PMH model was foundational to normal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1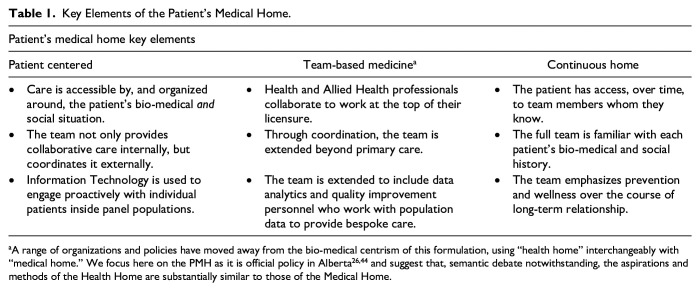 Figure 2
Figure 2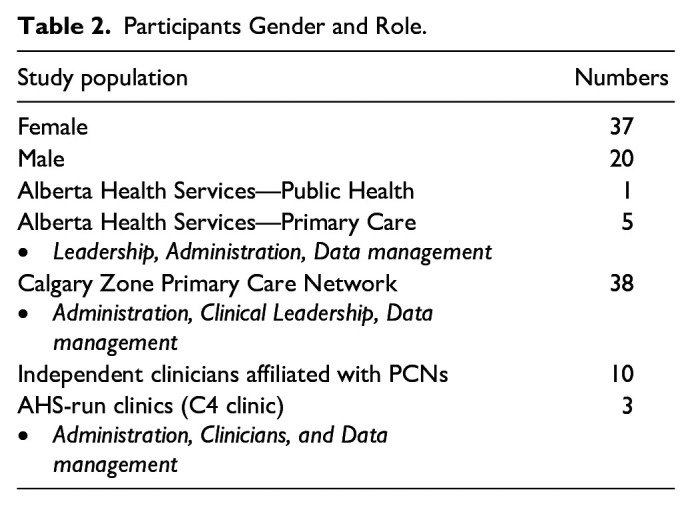 Figure 3
Figure 3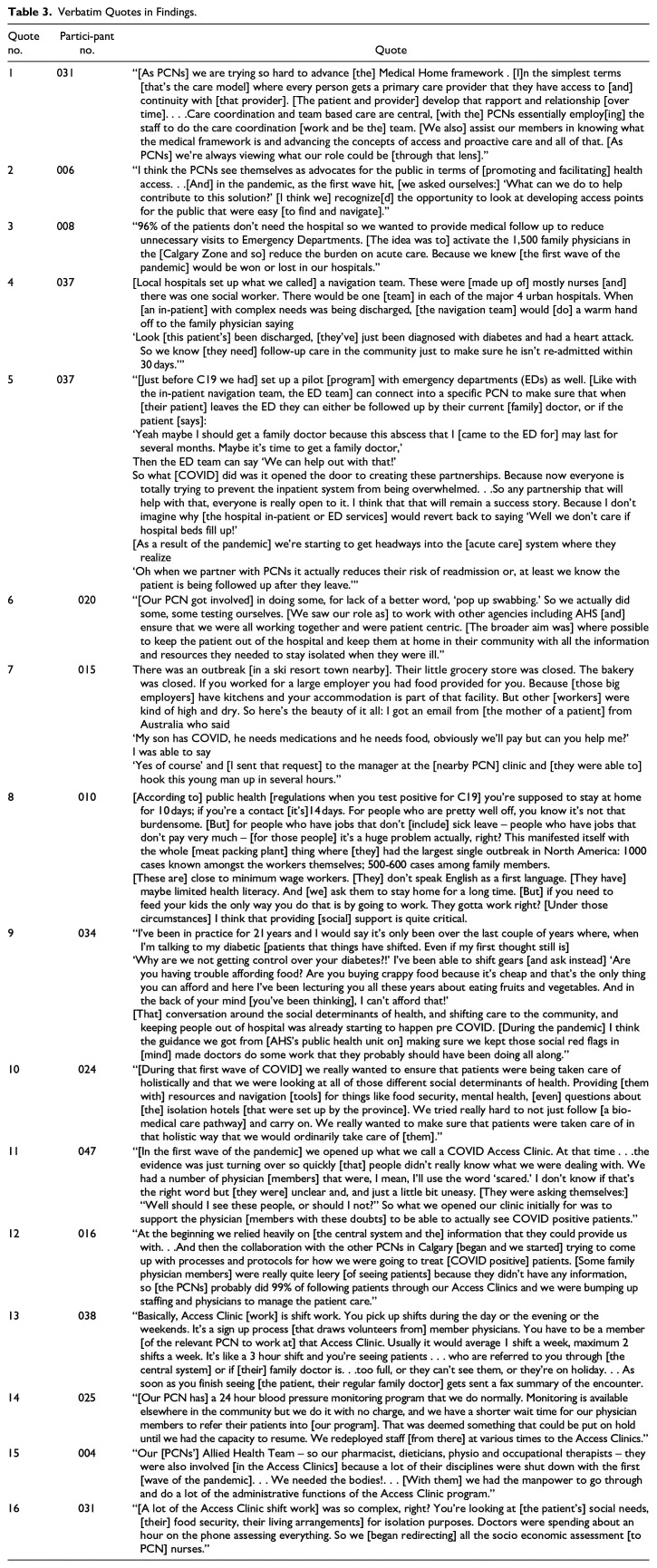 Figure 4
Figure 4- —College of Family Physicians of Canadahttps://doi.org/10.13039/501100000018
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPrimary Care and Health Outcomes · Healthcare Policy and Management · Chronic Disease Management Strategies
Background
Primary care teams have played significant roles in the response to COVID-19 (C19), ranging from the in-community management of patients^1,2^ to vaccine counseling and delivery.^3 ???-7^ Striving to deliver Primary Health Care (PHC) broadly and holistically conceived,^8,9^ those teams have protected the capacity of acute care facilities^ 10 ^ and integrated with other elements of the health system helping to achieve resilience.^11 ??-14^ The shock of the pandemic to PHC provision has been unique in its sustained severity,^15,16^ highlighting and exacerbating longstanding challenges to the provision of PHC including burnout amongst existing clinicians^17 ?-19^; threats to the financial viability of practices^20,21^; and a decreased flow of new physicians into the practice of family medicine.^22 ?-24^ In this context of new and old challenges, the pandemic’s effects on the delivery of PHC-focused care models are not well understood. This paper takes Canada’s Patient Medical Home (PMH)^ 25 ^ care model as a particular example of how the tenets and principles of PHC were shaped by, and put into action during, the C19 shock. It highlights how the PMH was not just a rhetorical trope for those providing PHC, but a way of imagining and organizing their response to the pandemic. We show how the PMH underpinned more effective integration of primary and acute care operations and draw out lessons for jurisdictions beyond where the study took place.
This paper analyzes qualitative data to describe how the PMH became a shared way of thinking about and responding to the pandemic amongst PHC stakeholders in Alberta, Canada. We begin by describing the primary care policy environment in Alberta, and then move to a brief history of the PMH, tracing out its focus on patient centrism, team-based medicine, and a continuous home or point of contact for patients. We next show how these concepts were enacted by stakeholders who took a shared rhetoric and turned it into action. Illustrating how PHC principles and PMH policies advanced under pandemic conditions, we pose questions for those designing reform and transformation policy for a post C19 environment. Following how the tenets of PHC were put into action through the PMH during the pandemic reveals important considerations for those working to transform primary care through policy.
Primary Health Care in Alberta
The delivery of PHC in Alberta is a provincial policy goal,^ 26 ^ supported by dedicated structures in the health system. Alberta is the only province in Canada to operate a single central health authority—Alberta Health Services (AHS). AHS’ dominant focus is on running acute care and long-term care facilities, as well as the provincial ambulance and public health services, but it does staff a dedicated PHC unit that aims to co-ordinate and integrate primary care into these broader operations. Recent moves toward reform appear set to diminish AHS’ role and empower a freestanding primary care organization^27 ?-29^ but these have not yet taken concrete shape. If this is the central system’s support for PHC, then there are also community-based structures—the Primary Care Networks (PCNs). The PCNs act as bridges between AHS and the independent-contractor physicians who provide the vast majority of primary care to Albertans, and who bill the provincial government on a fee-for-service (FFS) basis.^ 30 ^
The province’s more than 3800 independent primary care physicians have the option to join 1 of 40 PCNs. The majority opt-in, with their choice triggering a capitation payment based on the size of their patient panel, which is then made by the ministry of health to the selected PCN. While physicians are still reimbursed for their services through FFS, or in rare cases, other alternative methods of payment, the capitation funding is routed toward the PCNs In this way both FFS and capitation models run concurrently, with the PCNs being held accountable for the funds they receive on behalf of their member physicians through a range of requirements that include the delivery of the PMH. Their a particular focus as they operationalize the PMH, and their progress is measured, is on attaching patients and so improving Albertans’ access to PHC.^26,31 ?-33^ Initially focused on improving access and the patient-centeredness of care for patients with complex chronic conditions, the PCNs have added co-planning service delivery with local AHS authorities to meet the particular needs of the populations in their geographic catchments.
As much as the PCNs have evolved to be, if not the glue, then at least an interaction point between the acute care-focused AHS system and primary care, barriers to achieving integrated care coordination, and so delivering PHC, have persisted. Those barriers include an administrative focus on acute care and divergent funding and accountability models. As in the rest of Canada, Alberta focuses its time and money on the oversight and delivery of acute care. This specialization in, and emphasis on, building hospitals and managing in-patient services can be traced to the original negotiations and social contract that gave rise to the nation’s various publicly funded health systems.^ 34 ^ At the time that Canada’s modern health systems were established, primary care physicians (PCPs) preferred the status of an independent contractor working on a FFS basis, and this set them apart from the employee status and salaries of hospital-based physicians. Beyond paying more attention to paid employees working in acute care than to independent contractors working in longitudinal care, the 2 funding models have been deployed with quite different accountability expectations. Despite calls to draw primary and acute care into closer integration^ 35 ^ bridging those divergent expectations for performance has proved to be challenging.^36,37^
If the PCNs—striving to support their physician members in the delivery of the PMH—were the primary contact point between the isolated primary and acute care elements of Alberta’s system prior to C-19’s arrival, the pandemic perturbed operations significantly. Actions taken by AHS units that were aimed at rapidly deploying mass C-19 testing across the province initially did not include provision for test result notifications to be shared with PCPs.^ 14 ^ This emergent integration challenge^ 15 ^ was met with parties in the 2 siloes building a data bridge between C-19 clinics run by the PCNs and the AHS public health and testing units generating the results.^ 13 ^ The integration enabling data bridge solution ensured PCPs knew about C-19 positive patients, and that those patients received in-community follow-up. Staff from the PCNs- and AHS personnel also combined to develop an evidence-based clinical algorithm that supported PCPs in providing medical and social care to C-19 positive patients in the community. Emergency Departments in AHS hospital facilities were made aware of the follow up strategy, and knowing it was in place altered their threshold for admission allowed them to discharge “borderline” patients knowing they would be followed for deterioration.^ 14 ^ The pandemic, then, was a generative moment in the integration history of the primary and acute care elements of Alberta’s system. It provided the impetus for overcoming persistent barriers to integration, and, as we will show, the enactment of the province’s PHC goals through its specific commitment to the PMH.
The Patient’s Medical Home
The broad goals of PHC, set out in the 1978 Alma-Ata declaration,^ 38 ^ can be described as providing widely accessible first-line care focused on patient needs and experiences that goes beyond, and wraps around, those patient’s bio-medical conditions.^39,40^ This is to say, PHC works with the social, as well as the bio-medical, determinants of health.^41,42^ It offers patients convenient, comprehensive, future-focused care delivered over time and in the context of a continuous relationship.^9,39^ It involves not just care delivery, but co-ordination, with an emphasis on teams of clinicians working together and at the top of their members’ licensures.^43 ?-45^ A decade or more ago, these broad PHC concepts were distilled into the Patient Centered Medical Home care model in the United States.^46 ???-50^ That model has shown significant promise in reducing costs and improving outcomes since.^ 49 ^ Renamed the PMH as part of its adaptation to Canadian primary care conditions,^25,51,52^ the model has subsequently been adopted across the country^53,54^ having been assessed, revised, and evaluated in terms of general policy preparation and uptake^54 ?-56^ as well as for the factors shaping and shaped by the members of its teams.^57,58^ Table 1 highlights key elements of the PMH as deployed in Canada.
Table 1.: Key Elements of the Patient’s Medical Home.
In March 2020, when Alberta’s first C19 case was identified, as with other PHC organizations,^11 ??-14^ PCNs pivoted to managing patients in the community.^13,14^ They brought to this pandemic response work not just their resources, but their mandated commitment to the PMH.^ 26 ^ This is to say, they brought the PMH as an operational model to the work of making the principles of PHC real under pandemic conditions. In what follows, we highlight how C19 interacted with and informed PHC stakeholders’ approach to, and operationalization of, the PMH. We draw broader lessons for those seeking to continue the transformation of primary care toward PHC principles and the enactment of the PMH.
Methods
The qualitative data presented in this paper are from a broader mixed-methods research study that sought to understand: (1) if, and how, patients of a PCN-based C19 clinic were already connected to a PMH; and (2) if, and how, any new patients were matched with a PCP in the process of becoming attached a PMH for the first time^ 13 ^ In the course of the analysis and coding process aimed at answering these questions our team identified crosscutting themes that highlighted the PMH and its underlying PHC principles being put into action under pandemic conditions. In this way we shifted from a deductive project aimed at answering a priori questions to a deductive emergent analysis driven by the collected data.
To gather the qualitative data presented here, we completed semi-structured interviews from January 2021 through to March 2021 with a range of stakeholders whom we identified using purposive (https://methods.sagepub.com/foundations/snowball-sampling) and snowball sampling techniques.^59,60^ The project’s Scientific Advisory Committee identified prospective participants and selected them based on their involvement and influence in shaping the primary care response to C19, ensuring that AHS, PCNs, and physicians were represented amongst those interviewed. An e-mail invitation was sent to 79 individuals identified by the Scientific Advisory Committee and as people consented to take part, interviews took place and recruitment continued. Of the 79 identified, 57 individuals agreed to participate and completed an interview that lasted between 19 and 71 min (average length = 35.7 min, median length = 32.5 min). PCNs employed 39 participants (eg, executive directors, physician clinical directors, clinic managers, physician leads, and technical analysts who supported the data sharing process), AHS employed 10 (primary care medical directors and executive directors and managers of AHS clinics that coordinated with PCN clinics and leadership), and community physicians connected to PCNs represented the final 8 participants (Table 2).
Table 2.: Participants Gender and Role.
Interviews were conducted by 2 members of the research team with extensive experience in qualitative research. Almost all one-on-one interviews were conducted virtually (ie, using Zoom), with 2 of the 57 interviews including 2 or more participants. We emailed all participants an informed consent from prior to participation, along with a copy of the interview questionnaire so that they could consider the questions in advance. Interviews were audio-recorded and subsequently transcribed verbatim. In addition, we produced a summary cover sheet immediately following each interview to capture emerging observations and themes.
Interviews explored the integrated response between the central health authority (ie, AHS), the PCNs, and community physicians. Interviews aimed to understand how the people, organizations, and relationships facilitated or inhibited the C19 response initially, as well as how these changed throughout the course of the response during the first wave of C19 infections. Interviewers used open-ended, narrative interviewing, which is a method of qualitative data gathering that encourages participants to speak to their own experiences in whatever order they feel is most meaningful, allowing the participants to prioritize their perspective rather than adhering to a strict research agenda.^ 61 ^ Using a semi-structured interview guide, interviewers asked questions and identified probes; however, interviewers followed the participants’ lead and what the latter chose to prioritize and share during the interview based on their own experiences.
This study utilized the Interpretive Description approach. This analytical approach involves a continuous relationship between data collection and analysis, whereby interviews are conducted and field notes (interview summary cover sheets) are taken to capture observations made during the data-gathering process that can help contextualize the data during analysis.^ 62 ^ Upon completion of the interviews, the 2 researchers who conducted the interviews reviewed the transcripts and cover sheets to orient themselves to the data and develop a set of preliminary codes. They performed this first cycle of open coding until they assigned each segment of text a conceptual code that described its contents. Qualitative researchers employed the constant comparative approach, whereby they developed each code in consideration of all other codes in order to determine analytic distinctions.^ 63 ^ Once the data were coded, a third analyst completed a second focused phase of coding to identify patterns and develop themes that conceptualized larger segments of the data. Analysis was considered complete when the coding became saturated, and the established themes adequately described the patterns in the data. While we did not seek participant feedback on the analysis, we did review a high-level summary of emerging themes as a group (which included primary care physicians). This study was approved by the University’s Conjoint Health Research Ethics Board (REB20-0959).
Findings
Key themes found in the data included: the importance of the PMH to overall PCN operations and the impact of C19 on those operations; and approaches to maintaining patient centric, team-delivered, and continuous care.
Importance of PMH and Impact of C19
PCN staff and physicians emphasized the importance of the PMH to their organizations’ operations. They described how PMH tenets were foundational to normal operations, with a focus on ensuring access to well-coordinated care (Table 3, Quote 1). The pandemic, however, introduced a specific access issue that extended beyond the PCNs’ world: hospital capacity (T3, Q2). Protecting acute care’s capacity to deal with the sickest patients became a key organizing principle as the PCNs responded to the pandemic (T3, Q3). In these pandemic induced adaptations we see the PCN teams seeking to deliver on their specific PMH mandate, and so on the broader PHC principal of ensuring access, by expanding their definition to include the protection of central hospital capacity through the management of C19 patients in the community.
Table 3.: Verbatim Quotes in Findings.
Over the course of the pandemic, to ensure access to PHC, PCNs expanded their capacity to coordinate care with centrally managed acute care facilities. PCN staff integrated into navigation teams that were set up by local hospitals to facilitate the discharge of post-C19 in-patients who also had complex chronic conditions. These warm hand-offs from acute- to primary-care (T3, Q4) extended the care delivery team beyond PHC, increased coordination and mutual trust between the 2 parts of the health system, reduced hospital readmissions, and sought to attach patients to a PMH if they did not already have 1 (T3, Q5). Similarly, in the Emergency Department setting, a pre-pandemic and PHC-focused partnership between hospitals and PCNs aimed at coordinating care in the community and attaching patients to a PMH gained momentum as C19 struck (T3, Q5).
Approaches to Maintaining Patient Centric, Team-Delivered, and Continuous Care
PCNs serving rural areas sought to ensure access by opening their own C19 testing centers. In Alberta, testing was a central system mandate, but the drop-in and drive-through facilities were often distant from rural patients’ homes. In response, a rural PCN adhering to the PMH’s patient centric principals, opened its own “pop up swabbing” center (T3, Q6). With rural Alberta hosting large populations of both short-term international workers and permanent immigrant and refugee newcomer workers, local PCNs encountered particular access-to-care issues in these lower-income populations. Short-term international workers in locked-down ski resorts found themselves without access to food and medication. PHC teams of physicians and PCN staff following the PMH’s holistic and relationship-focused principles responded to this combination of food insecurity and medical need (T3, Q7). In an adjacent PCN’s catchment, lower wage immigrant workers at a rural meat packing plant were similarly prioritized for access to team-delivered holistic social and medical supports (T3, Q8). While the patient centric foci of ensuring access and addressing the social determinants of health were not new, the pandemic sharpened family physicians’ focus on providing care that went beyond bio-medical considerations (T3, Q9-10).
In urban areas, efforts to ensure patients had convenient access to PHC focused on the creation of C19 Access Clinics. These clinics emerged in the first wave of the pandemic as individual family physician members of the PCNs wrestled with fears and incomplete or varying information on the virus and the number of appointments available to patients dropped (T3, Q11). Relying heavily on information supplied by central AHS systems, staff from the various urban PCNs began collaborating to expand and adjust the way the C19 Access Clinics worked and to safeguard patient access to PHC (T3, Q12). Family physicians worked shifts at the clinics, providing access to care in the absence of in-PCN colleagues (T3, Q13). For their part, the PCNs themselves redeployed allied health staff from other PMH-focused programming that had been suspended due to the pandemic (T3, Q14-5), reconstituting and expanding the team that was delivering care. These redeployments backstopped family physicians who were working shifts at the Access Clinics and spending far longer to understand and respond to the social determinants of their patients’ health than was covered by the available FFS billing codes (T3, Q16).
Our data highlights, on the one hand, that primary care teams protected the acute care system’s capacity. On the other, we have shown that those same teams ensured access to PHC in the community. Protecting hospital capacity became a shared mission that transcended the Alberta health system’s silos of “independent FFS primary care” and “centrally funded acute care.” If this became a shared mission, the words of the shared narrative that supported it were taken directly from PHC principles and provincial PMH policies. The PMH care model became the words and ways to think about, engage with, and respond to the C19 shock.
Discussion
As shown, PCN staff and family physicians, as well as their counterparts in hospital in-patient and Emergency Departments, saw their pandemic mission as being one of ensuring access. Access has been defined broadly as “the degree of fit between clients and the system”^ 64 ^ with 5 specific dimensions of this “fit” identified as: availability, accessibility, accommodation, affordability, and acceptability,^ 58 ^ with a sixth dimension “awareness,” added more recently.^ 61 ^ Our participants’ efforts to protect the acute care system by diverting patients or managing them in-community to prevent re-admission were focused on “availability.” Which is to say, the mission and narrative shared by primary care and acute care personnel hinged on balancing the relationship between the volume of existing services and resources and the volume and type of patient needs.^ 65 ^
While this dimension of access was clearly important in the thinking and actions of independent primary care stakeholders as they built the C19 Access Clinics, our data suggest the pandemic encouraged gains in other aspects of access as well. Specifically, “accessibility,” “accommodation,” and “awareness” were particularly targeted by primary care teams as they used the principles of PHC and policies of the PMH to make sense of and respond to the pandemic. As evidenced by the efforts rural locations to open pop-up testing centers, accessibility in access was sought through efforts to optimize the relationship between the location of primary care supply and patients’ locations. As evidenced by the efforts to address food insecurity as well as biomedical issues, accommodation in access was sought through efforts to tailor care availability to the temporal, spatial, and social needs and capacities of patients As evidenced by efforts to integrate PCN staff into acute-care-based navigation teams, awareness in access was sought through efforts to optimize the flow of well-adapted communications and information.
Grounding these efforts to ensure access—arguably the defining feature of PHC^ 66 ^—was the emphases and practices of the PMH. Patient centrism was expressed as a focus on not just bio-medical conditions, but the social determinants of health. It saw primary care teams create C19 Access Clinics, pop-up swabbing stations, food security interventions, isolation management solutions, and it saw them altering their clinical encounters, all so that patients were met where they were spatially, bio-medically, and socio-economically. Team-based medicine was made a practical reality in partnership and care-coordination efforts that extended well beyond the primary care clinic, and in the redeployment of PCN staff to distribute the work required to deliver patient centrism under pandemic conditions. Establishing a continuous home connection with more patients—indeed “all Albertans” as called for in policy^ 26 ^—was pursued through partnerships with acute care stakeholders who, as C19 shocked their capacity, came to understand the value of working with primary care and so of attaching patients to a medical home.
In these examples of the pandemic pushing progress toward PHC, there are also unanswered questions. Our methods, as with all qualitative studies, offer a cross-sectional study of a moment in time and, notwithstanding our participants’ hopes that relationships and improvements to access would survive the waning of C19, it is unclear whether the gains we describe here can be maintained. Given that the pandemic rendered the redeployment of a small army of PCN staff possible, how might the accessible patient-centric care that was delivered under such heightened circumstances be supported in less fraught times? As jurisdictions around the world face strained primary care systems and demands for reform or transformation grow,^67 ?-69^ more research is required to understand how not just to embed the narrative and mission of PHC in stakeholders’ minds and practices, but to rebalance funding and incentives to support the PMH beyond the C19 shock.
Conclusion
More than 45 years after the Alma-Ata Declaration, the C19 pandemic delivered a shock to primary care systems around the world. In the intervening time, the Declaration’s PHC principles had become the basis of widely adopted care models like the PMH. In the case of Alberta’s PCNs, the PMH provided the words, and ways, to think about, engage with, and respond to the C19 shock. It focused primary care personnel on the various dimensions of care access, and through its emphasis on patient centrism, team-based delivery, and continuity of care, saw them flexibly adapting to changing conditions. Indeed, the pandemic provided an opportunity for operationalization of PHC principles, and created a foundation of new relationships and ways of working to further explore PHC tenets. The extent to which these gains are shared in other jurisdictions, and the PMH narrative can be embedded in normal non-pandemic operations as health system reforms are undertaken, remain open questions.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241236007 – Supplemental material for Thinking and Enacting the Patient Medical Home Under Pandemic Conditions: A Qualitative Study From Primary Care in Alberta, CanadaSupplemental material, sj-docx-1-jpc-10.1177_21501319241236007 for Thinking and Enacting the Patient Medical Home Under Pandemic Conditions: A Qualitative Study From Primary Care in Alberta, Canada by Myles Leslie, Brian Hansen, Rida Abboud, Caroline Claussen and Fariba Aghajafari in Journal of Primary Care & Community Health
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chakraborty S Vyse A Coakley A. Engaging primary care in the community management of COVID-19: Global lessons from a small town in Alberta, Canada. Health Affairs Blog. 2020. Accessed August 28, 2020. https://www.healthaffairs.org/content/forefront/engaging-primary-care-community-management-covid-19-global-lessons-small-town-alberta.
- 2British Columbia Ministry of Health, BC Centre for Disease Control. Guidance for primary care management for adults in the community with suspected or confirmed COVID-19. British Columbia Ministry of Health. Updated December 15, 2022. Accessed August 28, 2020. http://www.bccdc.ca/Health-Professionals-Site/Documents/BC_COVID_primarycare_outpatient_mgmt.pdf.
- 3Newton WP Baxley E Magill M. Learning from COVID-19: system blindness to primary care. Ann Fam Med. 2021;19(3):282-284. doi:10.1370/afm.270534180855 PMC 8118485 · doi ↗ · pubmed ↗
- 4Leslie M Pinto N Fadaak R. Improving conversations with COVID-19 vaccine hesitant patients: action research to support family physicians. Ann Fam Med. 2022;20(4):368-373. doi:10.1370/afm.281635443974 PMC 9328713 · doi ↗ · pubmed ↗
- 5Shakory S Eissa A Kiran T Pinto AD. Best practices for COVID-19 mass vaccination clinics. Ann Fam Med. 2022;20(2):149-156. doi:10.1370/afm.277335346931 PMC 8959732 · doi ↗ · pubmed ↗
- 6Ratzan S Schneider EC Hatch H Cacchione J. Missing the point—how primary care can overcome COVID-19 vaccine “hesitancy”. N Engl J Med. 2021;384(25):e 100. doi:10.1056/NEJ Mp 210613733951377 · doi ↗ · pubmed ↗
- 7Katzman JG Katzman JW. Primary care clinicians as COVID-19 vaccine ambassadors. J Prim Care Community Health. 2021;12:1-4. doi:10.1177/21501327211007026 PMC 877235033787395 · doi ↗ · pubmed ↗
- 8World Health Organization. Integrating Health Services. Technical Series on Primary Health Care. 2018. Accessed December 15, 2022. https://www.who.int/docs/default-source/primary-health-care-conference/linkages.pdf.