Damage Control Surgery for Duodenal Ulcer Bleeding With Massive Hematoma and Perforation Due to Over-the-Scope Clip (OTSC)
Kei Harada, Daibo Kojima, Ippei Yamana, Hirotaka Seike, Takahisa Fujikawa

TL;DR
This paper presents a successful case of a complex duodenal ulcer treated with a less invasive surgical approach inspired by damage control surgery.
Contribution
The paper introduces the application of damage control surgery principles to a rare and severe case of duodenal ulcer bleeding.
Findings
A less invasive surgical approach successfully treated a duodenal ulcer with massive hematoma and perforation.
Damage control surgery principles were effectively applied in this complex gastrointestinal case.
The use of an over-the-scope clip contributed to the complication requiring surgical intervention.
Abstract
Due to the advances in endoscopic technology, surgery for duodenal ulcer (DU) bleeding has decreased, although surgery is still necessary for more complicated cases. The concept of damage control surgery (DCS) has been established in the field of trauma, and a simple surgical approach may be preferable in serious cases such as uncontrolled DU bleeding. We present a successful case of bleeding with massive hematoma and perforation of the duodenum due to an over-the-scope clip that was treated by a less invasive surgical approach with consideration of the DCS.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
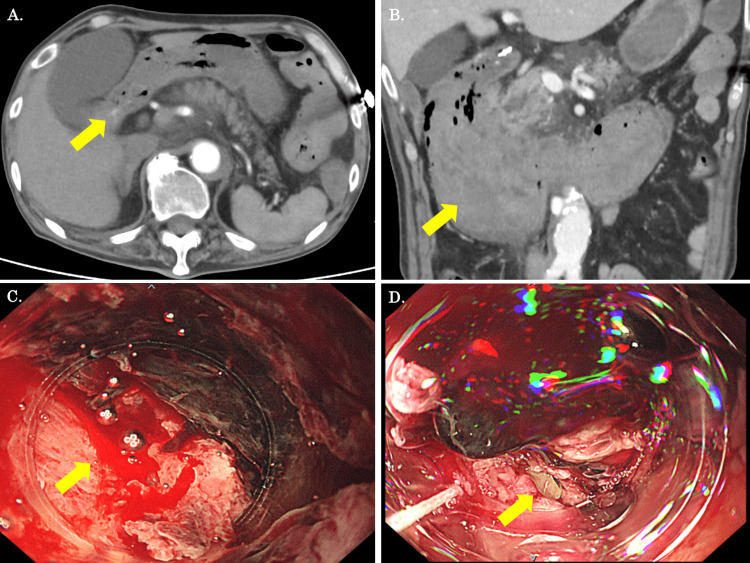 Figure 1
Figure 1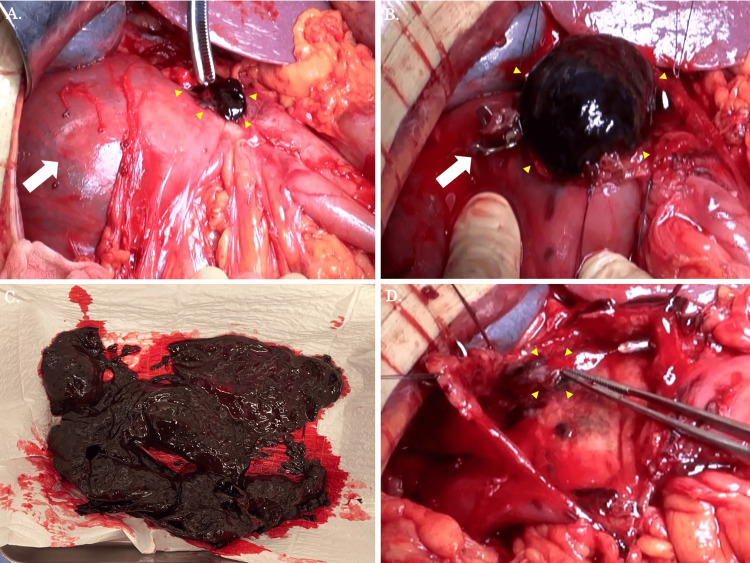 Figure 2
Figure 2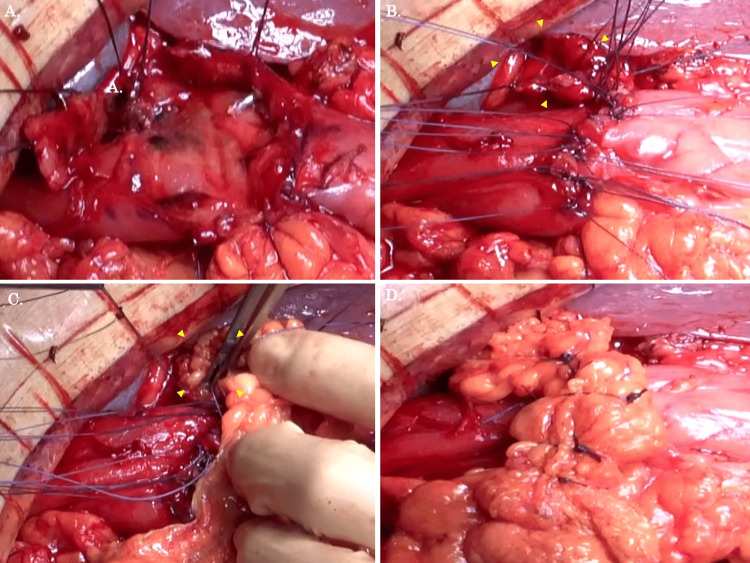 Figure 3
Figure 3 Figure 4
Figure 4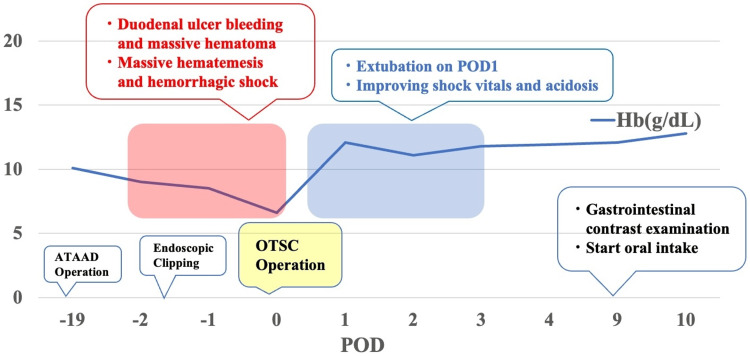 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Gastrointestinal Bleeding Diagnosis and Treatment · Foreign Body Medical Cases
Introduction
The frequency of surgery for peptic ulcer disease (PUD) has significantly decreased in the modern period due to the eradication of *Helicobacter pylori *and the development of anti-gastric acid medications like proton pump inhibitors [1,2]. However, surgery is still required in some cases, such as when it is difficult to stop bleeding with an endoscope, when the patient’s overall state is poor, or when complications arise as a result of endoscopic treatment [3,4].
Specifically, as we experienced, hemorrhagic shock-associated duodenal ulcer (DU) bleeding is a serious circumstance that requires immediate surgery, considering damage control surgery (DCS) [5,6]. DCS is a well-established surgical strategy for trauma treatment with hemodynamic stability as the primary goal and is now becoming popular in general emergency surgery [7].
Herein, we report a successful case of uncontrolled DU bleeding and perforation due to an over-the-scope clip (OTSC) that was treated with a less invasive surgical approach based on the concept of DCS. Furthermore, we hope that our case report will be useful in future treatment strategies for complicated cases of DU bleeding.
Case presentation
An 80-year-old man was referred to the gastroenterology department for an esophagogastroduodenoscopy (EGD) after hematemesis on postoperative day (POD) 18 following an operation for acute type A aortic dissection (ATAAD). The patient had chronic atrial fibrillation and was on warfarin. In addition, he had not taken any peptic ulcer agents since the ATAAD operation, but he had been using non-steroidal anti-inflammatory drugs every day for pain management. The EGD showed a small ulcer and open blood vessels in the duodenal bulb, which was then clipped. Since there were no other lesions with active bleeding and the patient’s vital signs were stable, it was decided to perform conservative treatment and conduct a second look two days later. The next morning, the patient had hematemesis once more. An enhanced CT scan was conducted. The CT scan showed extravasation near the clip of the inferior wall of the duodenal bulb (Figure 1A). Furthermore, a massive hematoma was observed mainly in the duodenum (Figure 1B). At this time, the patient was referred to our surgical department. The vital signs recorded were as follows: blood pressure: 103/62 mmHg; pulse rate: 136 beats/min; and body temperature: 37.2°C. Blood gas analyses revealed the following values: pH: 7.26; partial pressure of arterial carbon dioxide: 89.1 mmHg; partial pressure of arterial oxygen: 152.7 mmHg; HCO3: 29.3 mmol/L; and lactate: 2.67 mmol/L. We opted to do an EGD in the ICU with the surgeons on standby. An EGD showed an ulcer on the lower wall of the upper intestinal angle. The ulcer was still oozing in one place (Figure 1C). A 9-mm OTSC was performed at the same location, and a mucosal defect that seemed to be a perforation was discovered at the base (Figure 1D).
CT and EGD findings prior to the emergency operation(A, B) An enhanced CT scan showed that extravasation was present around the duodenal clipping point, and the duodenum was significantly dilated due to massive hematoma (yellow arrow). (C) An EGD showed that active bleeding was observed at the posterior lateral aspect of the duodenum (yellow arrow). (D) An EGD showed a mucosal defect that appeared to be perforation after OTSC (yellow arrow).EGD, esophagogastroduodenoscopy; OTSC, over-the-scope clip
Despite blood transfusion therapy, shock vitals continued, acidosis worsened, and OTSC perforation was discovered. Therefore, we decided to perform emergency surgery, considering DCS. The surgical findings and methods are presented here. An incision was made in the midline of the upper abdomen under general anesthesia. After mobilization of the duodenum, a significantly dilated duodenum and a perforation site suspected to be caused by OTSC were detected (Figure 2A). We performed a longitudinal duodenotomy extending across the pylorus to the distal stomach, and then massive duodenal hematomas were successfully removed (Figure 2B). It was about 350 grams of hematoma that was removed (Figure 2C). The mucosal surface of the duodenum could be clearly observed, and the bleeding was quickly halted with a Z suture (Figure 2D).
Intra-abdominal findings during operation(A) After a mobilization of the dilated duodenum (white arrow), the perforation site was observed (yellow arrows). (B) When the perforation site was opened to the gastric and duodenal sides, an OTSC (white arrow) and massive hematoma (yellow arrows) were found. (C) The hematoma removed was approximately 350 grams. (D) The bleeding from the wall of the duodenal ulcer, probably from a very small blood vessel distal to the gastroduodenal artery, from the duodenal wall (yellow arrows), was quickly halted with a suture.DU, duodenal ulcer; OTSC, over-the-scope clip
Based on an adaptation of the DCS idea, we decided that perforation closure and filling of the greater omentum were preferable to duodenal resection and gastrointestinal reconstruction. On the side where normal duodenal mucosa was still present, interrupted suture closure was carried out (Figure 3A, 3B). Greater omental filling was performed on a weak duodenal location with severe ulceration (Figure 3C). Additionally, the greater omental covering of the perforation was added with the thread left over after the interrupted suture closure (Figure 3D).
The surgical procedure is shown(A) After suturing the ulcer hemorrhage, the duodenal mucosal surface and tissue fragility were confirmed. (B) Interrupted suture closure was performed on the side where macroscopically normal duodenal mucosa remained. Suture closure was not performed in areas where the tissue was very fragile (yellow arrows). (C, D) Greater omentum filling and covering were performed in areas that were not closed with sutures (yellow arrows).
After that, a jejunostomy was made, and the operation was over. The time of the operation was two hours and 42 minutes, and 620 ml of blood was lost, including the hematoma that was removed. After the operation, the patient’s vitals returned, and acidosis improved. The patient was successfully extubated on POD 1, and enteral nutrition was started through the jejunostomy on POD 2. An oral intake was initiated on POD 9, following an oral gastrointestinal contrast test that verified no issues (Figure 4). Other than a little local intra-abdominal abscess and a urinary tract infection, the patient was able to eat normally after that and was sent to a rehabilitation facility without any major issues.
The oral gastrointestinal contrast examination findings on POD 9The contrast medium flowed well, and no evident leaks or severe stenosis were found.POD, postoperative day
Figure 5 summarizes the clinical course of the patient. In reporting the case, we respected ethical considerations, including the protection of personal privacy, and provided sufficient informed consent to the patient.
Clinical course of the patientATAAD, acute type A aortic dissection; Hb, hemoglobin; OTSC, over-the-scope clip; POD, postoperative dayThe figure is the authors’ own creation.
Discussion
Upper gastrointestinal bleeding is still a medical condition requiring hospitalization, and peptic ulcer bleeding is reported to be the most common cause of bleeding, with a rate of 40-46% [8]. According to the treatment protocol for PUD, endoscopic hemostasis is the first line of treatment for bleeding ulcers. If this fails, surgery or interventional radiology is advised [1].
Especially for bleeding DUs, local methods (suture of ulcers with or without extraluminal gastroduodenal artery ligation) and gastroduodenal resections (distal gastrectomy with partial duodenectomy) are available. However, there is still a high rate of morbidity and mortality linked to surgery [9]. Endoscopic treatment for bleeding DU on the posterior wall of the duodenal bulb, as in our case, is difficult due to anatomical factors. Additionally, erosion of the gastroduodenal artery or its branches beyond the posterior duodenal wall can cause significant bleeding and increase the risk of rebleeding [10].
According to Kobara et al., an OTSC is a relatively safe device for an endoscopic procedure. However, all OTSC-related problems occurred in approximately 1.7% (26/1,517) of patients [11]. Additionally, there have also been reports of microperforation of bleeding DUs caused by OTSC [12]. In our case, we chose an OTSC as an endoscopic treatment before surgery to prevent rebleeding the following day after primary hemostasis. As a result, endoscopic hemostasis was incomplete, resulting in a poor blood transfusion response, leading to hemorrhagic shock, acidosis, and perforation associated with OTSC, which led to emergency surgery.
We adopted the concept of DCS to perform an emergency surgery. The aim of DCS is to lower the risk of death in seriously injured patients with physiological derangement, and its application has recently broadened to include bleeding from complex gastroduodenal ulcer illness, generalized peritonitis, acute mesenteric ischemia, and other diseases [13,14]. In our case, we performed an incision from the anterior wall of the duodenum to the gastric pylorus and sutures on the bleeding site with the aim of removing the extensive hematoma and stopping the ulcer bleeding. Commonly known surgical treatments for DU include PD, gastrointestinal reconstruction with ulcer resection, and Dubois surgery [15,16]. However, because the ulcer in our case was shallow and had not spread to major blood vessels or the pancreas, we were able to use the less invasive surgical approach outlined above and had no serious postoperative problems.
Conclusions
We successfully treated bleeding with massive hematoma and perforation of the duodenum due to an OTSC with a less invasive surgical approach with consideration of the DCS. The concept of DCS and a simple surgical approach could be one of the preferred options to manage critical situations, as in our case. We hope that our case report may help develop strategies for complicated cases of fatal DU bleeding and complications with endoscopic treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Evidence-based clinical practice guidelines for peptic ulcer disease 2020 J Gastroenterol Kamada T Satoh K Itoh T 3033225620213362058610.1007/s 00535-021-01769-0PMC 8005399 · doi ↗ · pubmed ↗
- 2Optimal management of peptic ulcer disease in the elderly Drugs Aging Pilotto A Franceschi M Maggi S Addante F Sancarlo D 5455582720102058384910.2165/11537380-000000000-00000 · doi ↗ · pubmed ↗
- 3Surgical therapy of peptic ulcers in the 21st century: more common than you think Am J Surg Sarosi GA Jr Jaiswal KR Nwariaku FE Asolati M Fleming JB Anthony T 77577919020051622695710.1016/j.amjsurg.2005.07.019 · doi ↗ · pubmed ↗
- 4Bleeding gastric and duodenal ulcers: case-control study comparing angioembolization and surgery Scand J Gastroenterol Nykänen T Peltola E KylänpääL Udd M 5235305220172827004110.1080/00365521.2017.1288756 · doi ↗ · pubmed ↗
- 5Emergency ulcer surgery Surg Clin North Am Lee CW Sarosi GA Jr 100110139120112188902610.1016/j.suc.2011.06.008PMC 3811928 · doi ↗ · pubmed ↗
- 6Emerging trends in peptic ulcer disease and damage control surgery in the H. pylori era Am Surg Smith BR Stabile BE 797801712005 https://pubmed.ncbi.nlm.nih.gov/16468522/16468522 · pubmed ↗
- 7Damage control: concept and implementation J Visc Surg Malgras B Prunet B Lesaffre X 029154 Suppl 1201710.1016/j.jviscsurg.2017.08.01229055663 · doi ↗ · pubmed ↗
- 8Acute upper GI bleeding: did anything change? Time trend analysis of incidence and outcome of acute upper GI bleeding between 1993/1994 and 2000 Am J Gastroenterol van Leerdam ME Vreeburg EM Rauws EA Geraedts AA Tijssen JG Reitsma JB Tytgat GN 149414999820031287356810.1111/j.1572-0241.2003.07517.x · doi ↗ · pubmed ↗