An Isolated Second Carpometacarpal Joint Dislocation Treated With Open Reduction and Transfixation With K-wire: A Rare Case Report
Saravanan Alagesan, Silambarasi Nagasamy, Pradeep Elangovan, Haemanath Pandian, Ganesh Anantharaman

TL;DR
A rare case of a second carpometacarpal joint dislocation was successfully treated with open surgery and K-wire fixation.
Contribution
This case report presents a rare and isolated second CMC joint dislocation requiring open reduction and K-wire transfixation.
Findings
An extensor tendon was interposed in the dislocated second CMC joint.
Open reduction and K-wire transfixation successfully treated the injury.
Rehabilitation began after K-wire removal three weeks post-surgery.
Abstract
Carpometacarpal (CMC) joint dislocation is a rare injury that can be easily missed due to non-specific clinical signs and radiologic findings. We report a patient with an isolated and irreducible dorsal dislocation of the second CMC joint, which required an open reduction and K-wire transfixation. An extensor tendon was found to be interposed between the base and the trapezoid. K-wire removal was done after three weeks and following the removal of the wire, rehabilitation was started.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
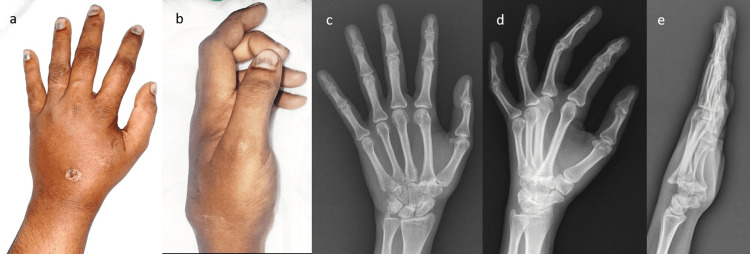 Figure 1
Figure 1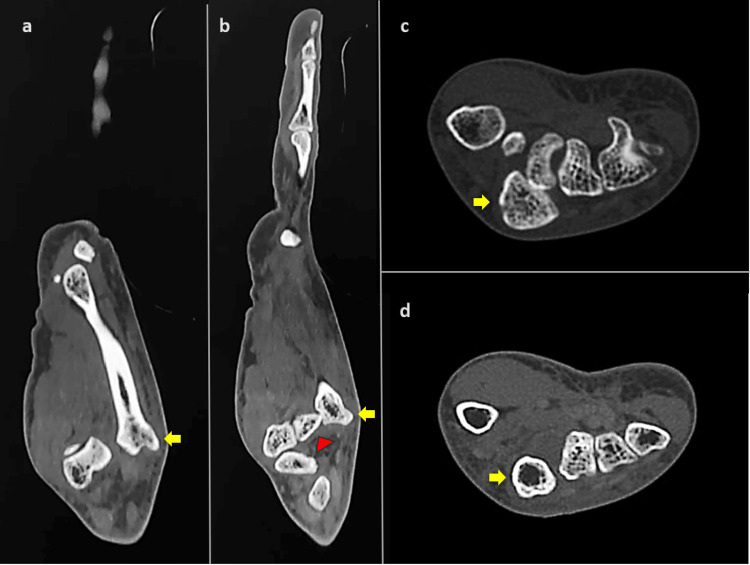 Figure 2
Figure 2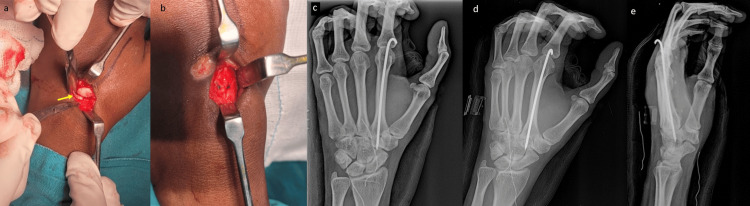 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Surgery and Rehabilitation · Elbow and Forearm Trauma Treatment · Musculoskeletal synovial abnormalities and treatments
Introduction
Carpometacarpal (CMC) joint dislocation is an uncommon injury that can be easily missed. It represents less than 1% of global hand trauma [1]. Fracture-dislocations of the CMC joints are more frequent than isolated dislocations, of which, dorsal dislocations are more common. These types of complex carpometacarpal injuries are a rare occurrence, with the last case of isolated second CMC joint dislocation reported in 1987 [2]. It is often missed due to non-specific clinical signs and radiologic findings. Also, the second CMC joint is extremely stable, which can be attributed to its strong ligamentous and bony stabilizers [2]. The articular facets, dorsal, volar and intermetacarpal ligaments provide a stable construct for this joint [3]. In an early presentation, a closed reduction may be possible. But in delayed presentations or unstable dislocations, open reduction may be required. We report a case of an isolated and irreducible dorsal dislocation of the second CMC joint, which required an open reduction and K-wire transfixation.
Case presentation
A 35-year-old female came to the Orthopaedics outpatient department with complaints of pain and swelling over the left hand for last one week. She gave an alleged history of skid and fall from her two-wheeler, thereby landing on an outstretched hand. On clinical examination, there was an abrasion of about 1 X 1 cm over the dorsum of the hand with a bony prominence (Figure 1) and tenderness present over the dorsal aspect of the base of the second metacarpal. She had limitation of active, as well as passive movements of the second metacarpophalangeal joint. Plain radiograph in anteroposterior and oblique view did not show any obvious bony abnormality but the lateral view of left hand showed isolated dorsal dislocation of the second CMC joint (Figure 1). Computed tomography scan was taken for better visualization of the CMC joint which revealed dorsal displacement of second CMC joint without any evidence of fracture (Figure 2).
Clinical pictures and X-rays at presentation(a) and (b) clinical pictures showing swelling over the dorsum of the hand, (c) anteroposterior and (d) oblique view of hand showing minimal bony overlap at second carpometacarpal joint, (e) lateral view showing dorsal dislocation at second carpometacarpal joint
Computed tomography of the hand (a) and (b) sagittal computed tomography sections demonstrating dorsal dislocation of the second metacarpal. Yellow arrow indicates dorsal dislocation of the base of the second metacarpal, while the red arrowhead indicates the trapezoid bone. (c) and (d) axial computed tomography sections showing disruption of the transverse metacarpal arch. Yellow arrow indicates the second metacarpal, which is no longer within the arch.
The patient was taken up for closed reduction under supraclavicular block. Closed reduction was found to be unsuccessful. Hence, open reduction was decided upon. Under fluoroscopy guidance, a 5cm long transverse incision was made over the base of the second metacarpal. The dorsal capsule was found to be disrupted. An extensor tendon was found to be interposed between the base of the second metacarpal and the trapezoid (Figure 3). The tendon was retracted and reduction was attempted, which was found to be satisfactory under fluoroscopy. The reduction was unstable and hence, a single 1.5mm K-wire was passed through the second metacarpal and into the trapezoid, stabilizing the second CMC joint by transfixation (Figure 3). Regular wound inspection and dressing was done.
Intra-operative pictures and postoperative X-rays(a) Intra-operative picture showing the base of the second metacarpal with the interposed extensor tendon (arrow) between the base of second metacarpal and the trapezoid, (b) sutured dorsal capsule. Postoperative X-rays showing the reduced second carpometacarpal joint transfixed with a K-wire; (c) anteroposterior, (d) oblique and (e) lateral views
Suture removal was done on the 12th postoperative day. K-wire removal was done after three weeks (Figure 4) and following the removal of the wire, rehabilitation was started. Patient returned to her routine activities by the end of fourth week.
Clinical pictures and X-rays after K-wire removalClinical pictures post-K-wire removal showing (a) dorsum and (b) lateral aspect of hand, (c) anteroposterior (d) oblique and (e) lateral views after K-wire removal
Discussion
This case report presents a patient with isolated second CMC joint dislocation, treated successfully with closed reduction and K-wire transfixation. CMC joint dislocations, a subset of complex carpometacarpal injuries, make up less than one of global hand trauma. These occur often due to high-energy trauma, where the direct impact causes dislocation of metacarpal base posteriorly following a flexion force subjected to the metacarpal head. Diagnosing an isolated CMC joint dislocation on the initial examination is difficult as it may be obscured by diffuse swelling of the hand [4]. According to a study by Henderson and Arafa in 1987, it was found that out of 21 patients with carpometacarpal dislocations, the diagnosis was missed in 15 cases in the accident and emergency department [5]. The anteroposterior and oblique views of the hand may also prove treacherous to the untrained eye, as the overlapping bones can obscure the pathology [6].
Iqbal et al. describe the Indian salutation test which may prove useful for acute dorsal dislocations of the ulnar four fingers [7]. On X-ray, one can look for the loss of the parallel appearance of opposing margins of the CMC joint and for overlapping at the CMC joint. Horneff et al. describe drawing metacarpal cascade lines to look for bony alignment and as mentioned in this case, a lateral view can be taken as well [8].
The longitudinal and transverse arches of the hand are disrupted following a CMC dislocation [9]. This can lead to decreased range of movement and poor grip. In order to restore the functional ability, reduction of the CMC joint is necessary.
Harwin et al. describe a case of isolated dislocation of the second and third CMC joints which required K-wire fixation to maintain the reduction [10]. Ho et al. reported a case of isolated dorsal dislocation of the second CMC joint, which was not amenable to closed reduction and hence, open reduction was performed where the extensor carpi radialis brevis was found to be interposing between the base of the second metacarpal and the trapezoid [2].
With closed reduction fails, open reduction is done keeping in mind the possibility of extensor tendon interposition. This is followed by a transfixation by K-wire to maintain the reduction.
Conclusions
Isolated CMC joint dislocations can be easily missed, both clinically and radiologically. In such cases, a lateral X-ray view or CT can be useful. Closed reduction must be attempted as soon as possible or, as in our instance, open reduction along with K-wire transfixation may be done. A regular follow-up is crucial to the patient’s rehabilitation after both closed, as well as open reduction. Vigilance in identifying and managing such rare hand injuries is essential for optimal patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Unusual case of carpometacarpal dislocation of all the four fingers of ulnar side of hand Med J Armed Forces India Sharma AK John JT 1881896120052740774810.1016/S 0377-1237(05)80024-3PMC 4922986 · doi ↗ · pubmed ↗
- 2Complex dorsal dislocation of the second carpometacarpal joint J Hand Surg Am Ho PK Choban SJ Eshman SJ Dupuy TE 10741076121987369384010.1016/s 0363-5023(87)80115-6 · doi ↗ · pubmed ↗
- 3The ligament and skeletal anatomy of the second through fifth carpometacarpal joints and adjacent structures J Hand Surg Am Nakamura K Patterson RM Viegas SF 101610292620011172124510.1053/jhsu.2001.26329 · doi ↗ · pubmed ↗
- 4Carpometacarpal joint dislocations: management and long-term outcomes at a specialized hand surgery center in Latin America Plast Surg (Oakv) Telich-Tarriba JE Guevara-Valmaña OI Navarro-Barquín DF Victor-Baldin A 2102142820203321503510.1177/2292550320933690 PMC 7644835 · doi ↗ · pubmed ↗
- 5Carpometacarpal dislocation: an unusual complex injury of the hand Arch Emerg Med Gibson MF Clancy MJ 565771990213518210.1136/emj.7.1.56PMC 1285663 · doi ↗ · pubmed ↗
- 6Man with left hand pain J Am Coll Emerg Physicians Open Barskaya A Lowy R Acosta N 04202310.1002/emp 2.13031 PMC 1044533237621467 · doi ↗ · pubmed ↗
- 7Indian salutation test in acute dorsal carpometacarpal joint dislocation of the ulnar four fingers Am J Emerg Med Iqbal MJ Saleemi A 74762120031256358710.1053/ajem.2003.50023 · doi ↗ · pubmed ↗
- 8Acute closed dislocation of the second through fourth carpometacarpal joints: satisfactory treatment with closed reduction and immobilization Hand (N Y) Horneff JG 3rd Park MJ Steinberg DR 227231820132442692410.1007/s 11552-012-9484-3PMC 3653003 · doi ↗ · pubmed ↗