Adenocarcinoma originating in the anterior mediastinum diagnosed by endobronchial ultrasound-guided transbronchial cryobiopsy: a case report
Hiroyuki Tsuchida, Yuji Matsumoto, Hideaki Furuse, Takaaki Tsuchida

TL;DR
A rare adenocarcinoma in the anterior mediastinum was successfully diagnosed using endobronchial ultrasound-guided transbronchial cryobiopsy.
Contribution
This case report highlights the effectiveness of EBUS-cryobiopsy in diagnosing mediastinal tumors with minimal tissue damage.
Findings
EBUS-cryobiopsy provided sufficient specimen quality for a definitive histopathological diagnosis.
The tumor was distinct from the patient's prior breast cancer, indicating a separate origin.
EBUS-cryobiopsy is a safe and effective alternative to CT-guided biopsies in complex anatomical regions.
Abstract
Endobronchial ultrasound-guided transbronchial cryobiopsy (EBUS-cryobiopsy) is advantageous for collecting larger specimens with minimal crushing; however, it has not been widely used for mediastinal tumors. A 73-year-old woman with a history of left breast cancer underwent surgery followed by radiotherapy. Computed tomography showed a mass in the anterior mediastinum that was in extensive contact with the sternum on the ventral side and partly with the trachea on the dorsal side. Two computed tomography-guided needle biopsies (CTNBs) were performed on the mass; however, a definitive diagnosis was not made because of severe crush artifacts. Subsequently, we performed EBUS-cryobiopsy and safely obtained sufficient specimen volume with minimal crushing. The histopathological diagnosis was adenocarcinoma, with immunobiological features distinct from those of previous breast cancers. Her…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
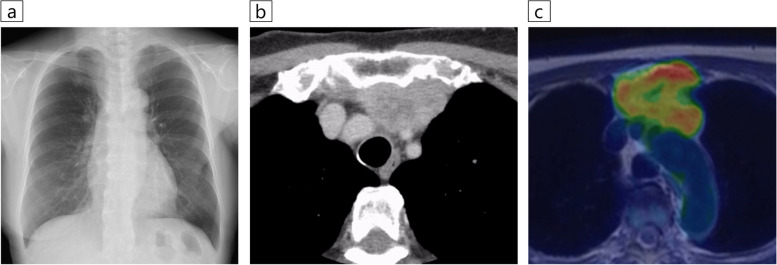 Figure 1
Figure 1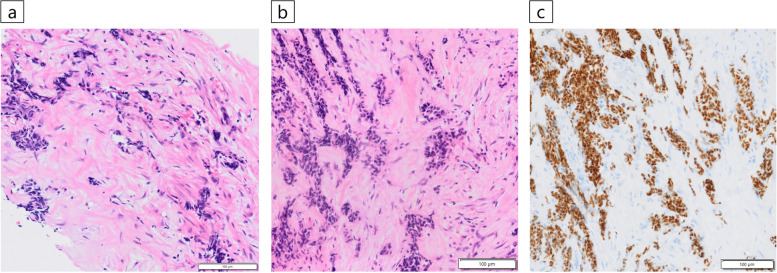 Figure 2
Figure 2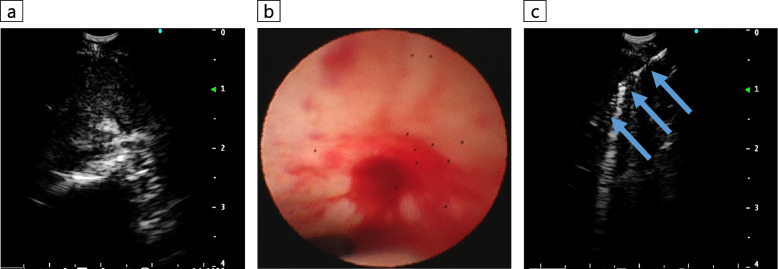 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Tumors Diagnosis and Treatment · Lung Cancer Diagnosis and Treatment · Infectious Diseases and Mycology
Background
Computed tomography-guided needle biopsy (CTNB) is the first-choice diagnostic method for mediastinal lesions that can be approached from the chest wall [1]. Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is a standard sampling technique for mediastinal and hilar lesions. However, because only cytological specimens are obtained with an aspiration needle, the diagnostic yield is limited. Recently, EBUS-guided transbronchial cryobiopsy (EBUS-cryobiopsy) has been reported to overcome these limitations.
We report a case of a patient with adenocarcinoma that originated in the anterior mediastinum adjacent to the trifurcation of the aortic arch and was diagnosed by cryobiopsy.
Case presentation
Patient information
The patient was a 73-year-old woman, who had never smoked, and who had a history of left breast cancer that was treated with surgery followed by radiotherapy. Chest radiography revealed an abnormal shadow in the mediastinum (Fig. 1a). There were no notable physical findings or abnormal values of various tumor markers.Fig. 1. Radiographic imaging findings. a Chest X-ray showed an abnormal opacity in the mediastinum at the patient’s first visit to our hospital. b Chest contrast-enhanced computed tomography showed a mass with a maximum diameter of 5.2 cm in the anterior mediastinum. The lesion was extensively in contact with the sternum on the ventral side and partly in contact with the trachea on the dorsal side, between the brachiocephalic and the left common carotid arteries. **c **^18^F-fluorodeoxyglucose-positron emission tomography (FDG-PET) showed high FDG uptake (maximum standardized uptake value was 6.71) in the anterior mediastinal mass and sternal infiltrate
Clinical findings
Chest contrast-enhanced computed tomography (CT) performed prior to ablation therapy for atrial fibrillation showed a mass with a maximum diameter of 5.2 cm in the anterior mediastinum. The mass was in extensive contact with the sternum on the ventral side and partly with the trachea on the dorsal side between the brachiocephalic and left common carotid arteries (Fig. 1b). ^18^F-fluorodeoxyglucose-positron emission tomography (FDG-PET) showed high FDG uptake in the mass and sternal infiltration but no significant uptake elsewhere (Fig. 1c). Two CTNBs were performed on the mass, but a definitive diagnosis was not made because of severe crush artifacts (Fig. 2a). We then performed EBUS-cryobiopsy to diagnose the lesion.Fig. 2. Histopathological findings. a An analysis of computed tomography-guided needle biopsy specimens did not lead to a definitive diagnosis due to severe tissue crushing (Hematoxylin and eosin staining). b The endobronchial ultrasound-guided transbronchial cryobiopsy specimens presented minimal crushing, and proliferating tumor cells with chromatin-enriched micronuclei were identified that formed scattered small foci against a background of extensive fibrous connective tissue with hyaline changes (Hematoxylin and eosin staining). c Immunohistochemical staining was positive for HNF4α, which is a finding suggestive of adenocarcinoma of gastrointestinal origin
Diagnostic assessment
Using a linear EBUS bronchoscope (BF-UC290F, Olympus, Japan), the lesion was delineated from the trachea while observing the brachiocephalic and left common carotid arteries as merkmals, and a 22-gauge needle (NA-U401SX, Olympus, Japan) was used to create a small tract in the tracheal wall while collecting specimens with EBUS-TBNA [2]. Subsequently, EBUS-cryobiopsy was performed four times with freezing for around five seconds each time by inserting a 1.7-mm cryoprobe (20402–410, Erbe Elektromedizin GmbH, Germany) into the lesion through the tract, which was completed without complications (Fig. 3). EBUS-cryobiopsy yielded sufficient specimen volume with minimal crushing. Histopathological findings revealed proliferating tumor cells with chromatin-enriched micronuclei that formed scattered small foci against a background of extensive fibrous connective tissue with hyaline changes, indicating adenocarcinoma (Fig. 2b). The immunohistochemical staining features were distinct from those of the past breast cancer and thymic epithelial tumors, although HNF4α, CDX2, and CK20 were positive, which suggested a gastrointestinal tumor (Fig. 2c). However, it was difficult to morphologically determine whether the metastasis originated from a gastrointestinal tumor, and the systemic examination was negative for the presence of a gastrointestinal tumor. The tumor was diagnosed as a rare adenocarcinoma originating in the anterior mediastinum.Fig. 3. Endobronchial ultrasound-guided transbronchial cryobiopsy (EBUS-cryobiopsy) procedure images. a The anterior mediastinal mass was visualized by EBUS with reference to the locations of the brachiocephalic and left common carotid arteries. b A small tract was made in the tracheal wall while sampling with EBUS-guided transbronchial needle aspiration using a 22-gauge needle. c EBUS-cryobiopsy was performed by inserting a cryoprobe with a diameter of 1.7 mm (arrow) into the lesion through the created tract
Therapeutic intervention
The patient underwent chemotherapy without any late complications of EBUS-cryobiopsy.
Discussion
We report a case of a patient with adenocarcinoma that originated in the anterior mediastinum and was diagnosed using EBUS-cryobiopsy. Epithelial tumors that occur in the anterior mediastinum include thymic carcinomas, metastases from other carcinomas, and primary anterior mediastinal carcinomas. In this patient, immunochemical staining was negative for PAX8, p40, ER, and PgR, ruling out thymic carcinoma and breast cancer metastasis. The immunohistochemistry suggested the adenocarcinoma was of gastrointestinal origin, which was ruled negative after thorough systemic examination. The tumor was diagnosed as an adenocarcinoma that originated in the anterior mediastinum. Mucinous adenocarcinomas associated with thymic cysts have been sporadically reported among primary anterior mediastinal adenocarcinomas; however, no prior reports have documented the correlation with HNF4α. To the best of our knowledge, this is the first case of a patient with adenocarcinoma that lacked thymic cysts and presented with HNF4α positivity.
CTNB has been reported to have a diagnostic yield of 94% for mediastinal tumors and should be considered as the highest priority when the tumor is in contact with or near the chest wall [1]. Previous reports have stated that using thinner needles (i.e., 20-gauge) and obtaining less than three samples were significant risk factors for CTNB diagnostic failure [3]. For this patient, four and six samples were collected using 18-gauge needles on the first and second attempts, respectively. Furthermore, diagnostic yields have been observed to be low in patients with malignant lymphoma [3]. We hypothesize that the diagnostic failure was due to extensive fibrous connective tissue within the lesion, which made the tumor highly susceptible to crushing. Also, it has been reported that mediastinoscopy biopsy has higher diagnostic accuracy than needle biopsy [4]. However, it is a fairly invasive procedure due to rib resection, incision location and length, longer follow-up time, and possible pleural opening [5]. Therefore, a less invasive transtracheal approach should be prioritized.
While EBUS has a high diagnostic yield due to real-time guidance, the yield by conventional TBNA is limited for some diseases. Recently, the efficacy of cryobiopsy, which allows for large-quantity and high-quality sampling, has been reported in two randomized controlled trials [6, 7]. Notably, we were able to diagnose the rare tumor mentioned above by performing EBUS-cryobiopsy. EBUS-cryobiopsy provides real-time results and can be performed safely, even for lesions that border major vessels, whereas conventional cryobiopsy for lung lesions carries the risk of bleeding.
Conclusion
Our findings suggest that EBUS-cryobiopsy can be safely performed in narrow areas surrounded by major blood vessels, and that the obtained specimens may be superior to those from CTNB for histopathological diagnosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Morrissey B Adams H Gibbs AR Crane MD Percutaneous needle biopsy of the mediastinum: review of 94 procedures Thorax 19934863263710.1136/thx.48.6.6328346494 PMC 464591 · doi ↗ · pubmed ↗
- 2Konno-Yamamoto A Matsumoto Y Imabayashi T Feasibility of modified endobronchial ultrasound-guided intranodal forceps biopsy: a retrospective analysis Respiration 202310214315310.1159/00052864436543151 · doi ↗ · pubmed ↗
- 3Lee HN Yun SJ Kim JI Ryu CW Diagnostic outcome and safety of CT-guided core needle biopsy for mediastinal masses: a systematic review and meta-analysis Eur Radiol 20203058859910.1007/s 00330-019-06377-431418086 · doi ↗ · pubmed ↗
- 4Watanabe M Takagi K Aoki TA comparison of biopsy through a parasternal anterior mediastinotomy under local anesthesia and percutaneous needle biopsy for malignant anterior mediastinal tumors Surg Today 199828101022102610.1007/BF 024839559786573 · doi ↗ · pubmed ↗
- 5Metin M Sayar A Turna A Extended cervical mediastinoscopy in the diagnosis of anterior mediastinal masses Ann Thorac Surg 200273125025210.1016/s 0003-4975(01)03182-411834018 · doi ↗ · pubmed ↗
- 6Fan Y Zhang AM Wu XL Transbronchial needle aspiration combined with cryobiopsy in the diagnosis of mediastinal diseases: a multicentre, open-label, randomised trial Lancet Respir Med 20231125626410.1016/S 2213-2600(22)00392-736279880 · doi ↗ · pubmed ↗
- 7Zhang J Guo JR Huang ZS Transbronchial mediastinal cryobiopsy in the diagnosis of mediastinal lesions: a randomised trial Eur Respir J 202158210005510.1183/13993003.00055-202133958432 · doi ↗ · pubmed ↗