TERT RNAscope analysis of sub-centimetric papillary thyroid carcinomas and synchronous lymph node metastases
Marie-Lisa Eich, Wiebke Jeske, Uschi Zenz, Costanza Chiapponi, Christina Alidousty, Sabine Merkelbach-Bruse, Reinhard Büttner, Anne M. Schultheis

TL;DR
This study examines the role of TERT RNA in small thyroid cancers and their lymph node metastases, finding no TERT expression in metastases.
Contribution
The study provides new evidence that TERT expression is not involved in early lymph node metastasis in small papillary thyroid carcinomas.
Findings
TERT RNA expression was not detected in lymph node metastases using RNAScope®.
Primary tumors and metastases showed low Ki-67 proliferation indices and wild-type p53 status.
Morphological patterns were heterogeneous in both primary tumors and metastases.
Abstract
Sub-centrimetric papillary thyroid carcinomas usually have a good prognosis with a cancer specific survival of > 99%, however in up to 65% of patients, lymph node metastases can be observed. Molecular alterations in BRAF, TERT and TP53 are associated with worse clinicopathological outcome in patients with papillary thyroid carcinoma. Twenty-two cases of papillary thyroid carcinomas measuring ≤ 1 cm with synchronous lymph node metastases were examined regarding morphological patterns and immunohistochemical status of p53, Ki-67, and BRAF V600E status. TERT RNA expression in lymph node metastases were evaluated by RNAScope®. Morphological patterns were heterogeneous in both primary tumors and lymph node metastases. Proliferation indices measured by Ki-67 were low. Both primary and lymph node metastases were wild type for p53 by immunohistochemical analysis. No lymph node metastasis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
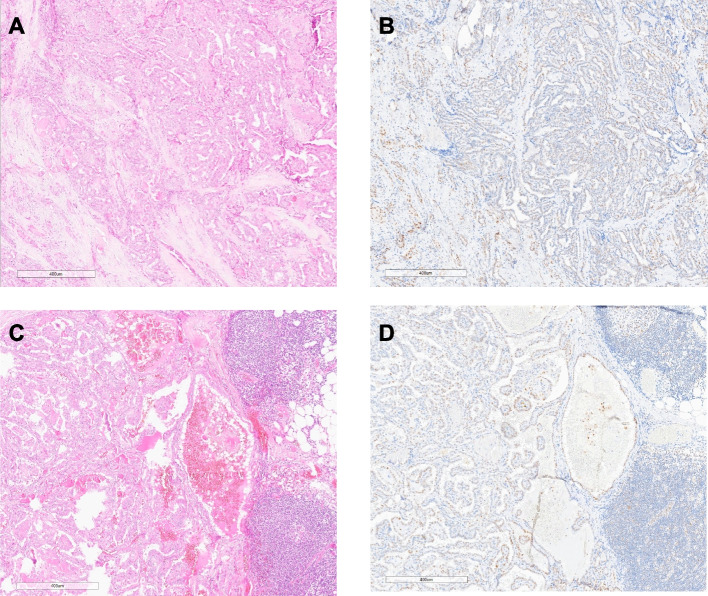 Figure 1
Figure 1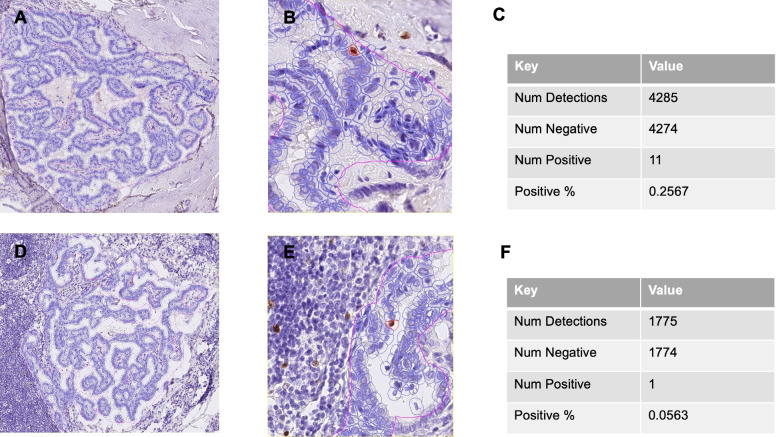 Figure 2
Figure 2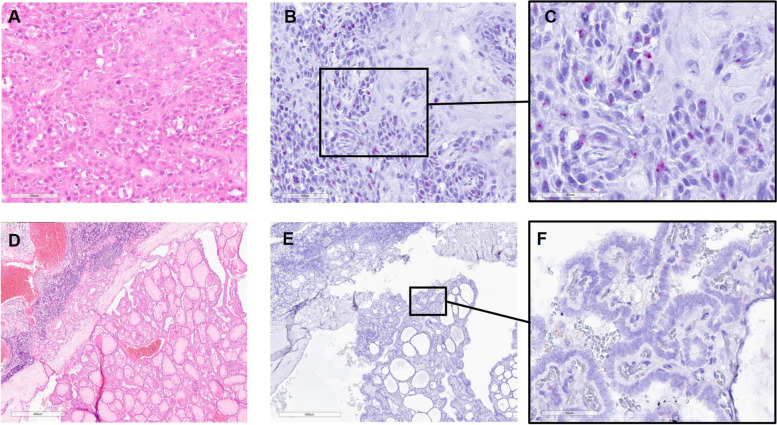 Figure 3
Figure 3- —Köln Fortune
- —Universitätsklinikum Köln (8977)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment · S100 Proteins and Annexins · Ferroptosis and cancer prognosis
Introduction
Papillary thyroid cancer is the most common endocrine malignancy in both adults and children [1]. Several clinicopathological factors have been described to be associated with a more aggressive behavior, such as patient’s age, tumor size, extrathyroidal extension, lymph node metastasis, margin status, and subtype [2, 3]. However, the outcome in patients presenting with papillary thyroid carcinoma is highly heterogeneous.
With the advent of next-generation sequencing studies, the genomic background of the disease was unraveled. In papillary thyroid carcinomas, a high rate of activating somatic alterations in genes that encode effectors of the mitogen-activated protein kinase (MAPK) signaling pathway have been identified, including point mutations in the BRAF and RAS genes, the TERT promotor region, as well as fusions involving the RET, ROS1, NTRK1 and NTRK3 tyrosine kinases. BRAF mutations occur in approximately 55% of all papillary thyroid carcinomas, and specifically the BRAF V600E mutation is the most common genomic alteration. Meta-analyses have shown that patients with a BRAF V600E mutation, especially in combination with a TERT promoter mutation, have a higher risk of unfavorable clinicopathological parameters such as extrathyroidal tumor spread, lymph node metastasis, and a higher TNM stage [4–7]. Also, alterations in TERT and TP53 can trigger progression from well-differentiated papillary thyroid carcinoma to more aggressive poorly differentiated thyroid carcinoma and anaplastic thyroid carcinoma [8, 9]. Genomic mechanisms of TERT upregulation and reactivation include TERT promotor mutations as the most common one. However, there are also other mechanisms that lead to overexpression of TERT mRNA. Recently, an assay for RNA in situ hybridization RNAScope® has been developed with the advantage of capturing all RNA aberrations leading to increase RNA expression.
Sub-centrimetric papillary thyroid carcinomas show in general a better clinical behavior with a cancer specific survival of > 99% [10]. They were classified as a distinct subtype of papillary thyroid carcinomas, namely papillary thyroid microcarcinoma, in the previous WHO classification. However, depending on the study, lymph node metastases have been described in up to 65% of patients [11, 12].
Therefore, our aim was to examine the role of TERT expression level alterations using RNAscope®, and histological patterns in a cohort of papillary thyroid carcinoma patients with a tumor size ≤ 1 cm harboring synchronous lymph node metastasis.
Methods
Patient cohort
The study was conducted in accordance to local ethical guidelines. Patient consent has been obtained from each patient after full explanation of the purpose and nature of the all procedures used, and approval by the ethical board was granted (number 21-1025_1, institutional review board of the University Hospital of Cologne).
Twenty-two specimens of papillary thyroid carcinoma with a tumor size ≤ 1 cm (traditionally classified as papillary thyroid microcarcinoma) and corresponding lymph node metastases diagnosed between 2012 and 2022 were retrieved from the surgical pathological archives. No prophylactic lymphadenectomy is performed in case of tumors ≤ 1 cm at our institution, according to the current German Guidelines. Accordingly, all patients had either preoperative sonographic or biopsy diagnosis of suspicious lymph nodes. In four patients papillary carcinoma lymph node metastases were detected on lymph node dissection for head and neck squamous cell carcinoma, followed by subsequent thyroidectomy. Lymph node metastasis removed later than 6 months after diagnosis were considered metachronous and were not included in the present study, as well as all with concomitant carcinoma > 1 cm.
Histopathological evaluation
Whole slide images of thyroid resection specimens and lymph node dissection samples were evaluated by two experienced pathologists (AMS, MLE). For establishment of diagnosis of lymph node metastasis of papillary thyroid carcinoma TTF1 and PAX8 immunohistochemistry was performed in routine diagnostic workflow. Positivity of TTF1 and PAX8, indicating thyroid origin along with morphologic features, lead to the diagnosis of lymph node metastasis from papillary thyroid carcinoma. The concomitant lymph node metastasis from head and neck squamous cell carcinoma were negative for these two markers.
Both primary tumors and lymph node metastases were examined with regard to presence of stromal desmoplasia, histologic variant of papillary thyroid carcinoma (infiltrative follicular, classic, and others), presence of inflammation, psammoma bodies, and extracapsular extension. Lymphovascular invasion in primary tumors was also examined, as well as the presence of underlying Hashimoto’s thyroiditis.
Immunohistochemical assessment
Whole slide sections of primary tumor and the largest lymph node metastasis were used to perform immunohistochemistry for p53 (clone: DO-7. 1:1800, Dako / CE), Ki-67 (clone: SP6. 1:100. Cellmarque / CE) and BRAF V600E (clone: VE1, ready to use, Roche / CE) following the manufacturer’s protocol. Detection of immunolabeling was performed using anti-mouse or anti-rabbit horseradish peroxidase–conjugated secondary antibodies and developed using 3,3′-diaminobenzidine.
For BRAF V600E diffuse cytoplasmic staining of tumor cells was considered positive and used as a surrogate marker for an underlying mutation. P53 was considered abnormal, if a strong nuclear expression in a majority of nuclei was present, a strong cytoplasmic staining or the absence of staining. A varying staining pattern across tumor nuclei was considered wild type staining pattern.
For evaluation of proliferation index via Ki-67, whole slide images were digitized with a Hamamatsu S360 scanner. Representative tumor areas were annotated in QuPath 0.3.2. Positive cells were detected running the built-in positive cell detection command using following parameters: detection image optical density sum, requested pixel size 1 µm; nucleus parameters: background radius 8 µm, median filter radius 0 µm, sigma 2 µm, minimum area 12 µm2, maximum area 400 µm2; intensity parameters: threshold 0.1, max background intensity 2; and cell parameters: cell expansion 5 µm, cell nucleus included.
TERT RNAscope®
The largest lymph node metastasis of each case was selected for analysis. RNAscope® detection for TERT was performed manually using the Hs-TERT-01 probe. Staining was done a per manufacturer’s protocol (ACDBio). Appropriate accompanying positive and negative controls (universal negative control dapB probe) were used to evaluate the staining procedure. After pre-treatment, probe hybridization and detection, the slides were counterstained with 50% hematoxylin, dehydrated, and mounted.
Expression quantification was carried out as described by Momeni-Boroujeni et al. [13] TERT signals in 100 cells were counted in hotspot regions.
Results
Clinicopathological parameters
Table 1 summarizes the clinicopathological parameters of the 22 patients with sub-centimetric papillary thyroid carcinomas with simultaneous lymph node metastasis identified at our institution from 2012 to 2022. Age and gender for each case can be found in Supplementary Table 1, as well as location (central and lateral compartment) of lymph node metastases.Table 1. Clinicopathological parameters in 22 patients with sub-centimetric papillary thyroid carcinoma and synchronous lymph node metastasesVariablesValuesn22Age, years Mean (± SD)48 (14.5 ± SD) Min, max19, 80Sex (%) Male13 (59%) Female9 (41%)pT stage (%) pT1a22 (100%)pN stage pN1a3 (14%) pN1b19(86%)Tumor size in cm Mean (± SD)0.52 (± 0.27) Lymph node metastasis size in cm1.64 Mean (± SD) ± 1.15 Multifocality (%)13 (59%)
Four patients (patient 4, patient 9, patient 13, and patient 17) showed simultaneous head and neck squamous cell carcinomas (patient 4: squamous cell carcinoma of tonsil; patient 9 squamous cell carcinoma of floor of the mouth, patient 13: squamous cell carcinoma of tonsil and patient 17: squamous cell carcinoma of larynx). Regarding outcome, data was available for 15 patients. One patient experienced disease recurrence in a cervical lymph node (see Supplementary Table 1).
Comparison of morphological features between primary tumors and lymph node metastasis
The morphological features of primary tumors and their lymph node metastases are summarized in Supplementary Table 1. Sixteen primary tumors were of classic and 6 of infiltrative follicular subtype, other subtypes were not observed. In patients 1, 2, and 14, the subtype differed between primary tumors and lymph node metastases. In patient 1, the primary tumor was of classic subtype, whereas the lymph node metastases showed follicular morphology. In patients 2 and 14, the primary tumor was composed of papillae and showed classic morphology, whereas the lymph node metastases were follicular. Lymphovascular invasion could not be detected morphologically in any of the tumors. Stromal dysplasia was present in 16 of primary tumors and 8 lymph node metastases. The size of primary tumors ranged from 0.3 to 10 mm and from 1.5 to 45 mm for the accompanying lymph node metastases. Extranodal growth was seen in four specimens. Fourteen primary tumors were BRAF V600E mutated by immunohistochemical evaluation. Of these, thirteen displayed classic morphology, and only one showed absence of stromal dysplasia. In thirteen of the corresponding lymph nodes, a mutational pattern was observed. In one case, no tissue was left for further evaluation (see Supplementary Table 1).
Immunohistochemical expression patterns of p53 and Ki-67 in primary tumors and lymph node metastasis
Tissue for immunohistochemical analysis of p53 and Ki-67 was available in 18 of primary tumors and all lymph node metastases. The P53 staining pattern was considered wild type in all specimens. Proliferation rates measured by Ki-67 ranged from 0.05 to 2.69% in primary and from 0.22 to 2.56% in lymph node metastases (see Table 2). Representative tumors are shown in Figs. 1 and 2.Table 2p53 and Ki-67 expression patterns in primary tumors and lymph node metastases in patients with sub-centimetric papillary thyroid carcinomasCaseThyroidLymph node metastases**P53-IHC****Ki-67 (%)P53-IHCKi-67 (%)**PTMC1NANAWT2.16PTMC2NANAWT1.73PTMC3NANAWT2.15PTMC4WT0.6WT0.54PTMC5WT0.86WT0.42PTMC6WT0.23WT0.78PTMC7WT0.68WT0.24PTMC8WT0.73WT2.17PTMC9WT0.75WT2.46PTMC10WT2.69WT0.3PTMC11WT0.55WT1.37PTMC12WT1.63WT1.76PTMC13WT0.06WT0.66PTMC14WT0.4WT0.33PTMC15WT0.37WT0.37PTMC16WT1.4WT6.76PTMC17WT0.26WT0.06PTMC18WT0.04WT2.43PTMC19WT0.57WT0.54PTMC20WT0.05WT1.32PTMC21NANAWT0.22PTMC22WT0.55WT0.93Fig. 1p53 expression pattern in sub-centimetric papillary thyroid carcinoma and accompanying lymph node metastases. HE- and p53 immunohistochemical staining in small papillary thyroid carcinoma (A, B) and lymph node metastases (C, D) in patient 13Fig. 2Ki-67 count in sub-centimetric papillary thyroid carcinoma and accompanying lymph node metastases. Ki-67 staining and detection pattern in papillary thyroid carcinoma (A, B, C) and lymph node metastases (D, E. F). B and E represent higher magnification images of A and D. Num Detections: number of detected cells. Num Positive: number of positive cells. Num negative: number of negative. % positive: % of Ki-67 positive cells
TERT status by RNAscope® in lymph node metastases
None of the 22 specimens showed TERT expression using RNAscope. In one of the tumors with accompanying lymph node metastases from squamous cell carcinoma, TERT expression was observed in squamous cell carcinoma in the basal portion of the tumor while being absent in superficial cell layers, as well as in the metastasis of papillary thyroid carcinomas (Fig. 3).Fig. 3TERT RNAScope® in lymph node metastases from sub-centimetric papillary thyroid carcinoma. TERT RNA expression in lymph node metastases from squamous cell carcinoma (HE: A, TERT RNA Scope®: B, C) and papillary thyroid carcinoma (HE: D, TERT RNA Scope®: E, F). Scale bar 100 µm (A, B), 400 µm (D, E), 60 µm (C, F)
Discussion
Although erased as a papillary thyroid carcinoma subtype in the updated 5th WHO classification system, papillary carcinomas measuring 1 cm or less were considered a subclass of papillary thyroid carcinomas and were included from 2004 until 2022 in the WHO classification of thyroid tumors under the term “microcarcinomas”. They are frequently incidental findings and traditionally show good clinical behavior. However, studies have observed lymph node metastasis in up to up to 65% of patients [11]. A more recent observational study including 293 patients with papillary thyroid microcarcinoma from 2003 to 2019 detected lymph node metastasis in 13.7% of patients, which were clinically unexpected in 9.8% and suspected in 3.8%. The authors found patient’s age < 45, tumor size ≥ 0.6 cm, the tall cell variant of papillary thyroid carcinoma, extrathyroidal extension and angioinvasion to be risk factors for lymph node metastasis on multivariate analysis [12]. In the study of 551 patients with papillary thyroid microcarcinomas by So et al., male gender, tumor multifocality, and extrathyroidal extension were predictive factors for lymph node metastasis on multivariate analysis. Their incidence on lymph node positivity was 37% [14]. Similarly, Gu et al. detected lymph node metastasis in 29.5% of their 268 studied patients with papillary thyroid microcarcinomas and found male sex, younger patient’s age, and tumor diameter on ultrasound > 0.5 cm to be risk factors for nodal involvement [15].
In our study, the mean tumor size was 0.52 cm. Additionally, the presence of other histological features like stromal desmoplasia, encapsulation, and multifocality were inconsistent in our group of patients with papillary thyroid carcinomas measuring ≤ 1 cm and harboring lymph node metastasis. Furthermore, BRAF V600E mutations have been shown to be a poor prognostic factor with regard to persistence of disease, recurrence, and overall survival [6, 7, 16]. In particular, the presence of coexisting BRAF V600E and TERT promoter mutations is associated with worse clinical outcome [17–21]. Studies on small papillary carcinomas (papillary thyroid microcarcinomas) found hotspot TERT promotor mutations in 0 to 8.7% of tumors [22–24]. Other studies have shown that not only TERT promotor mutations with the common hotspots C228T and C250T are linked to adverse outcome, but also aberrant TERT promoter methylation patterns, gains of the TERT gene locus at chromosome 5p15.33, and TERT mRNA overexpression [25–27]. When looking at TERT mRNA levels Pestana et al. found in their study of 244 thyroid samples malignant tumors to have higher TERT mRNA expression compared to benign lesions. The highest mRNA levels were found in more aggressive histotypes like poorly differentiated thyroid carcinoma, but also papillary thyroid carcinoma. These are known to harbor the highest frequencies of TERT alterations among thyroid lesions. Furthermore, mRNA expression was also found in the absence of TERT promotor mutations [28]. Generally, sequencing studies are time consuming and not always feasible, due to small tumor size and limited material. So far, there is no reliable IHC assay for TERT expression on the market [29]. Recently an assay for RNA in situ hybridization RNAscope® has been developed with the advantage of capturing all RNA aberrations leading to increase RNA expression. Examining the correlation between RNA-sequencing and the RNAscope® assay in 48 different tissue types gave promising results, while the in-situ hybridization method has the advantage of visualizing the expression pattern on a cellular level, making it possible to identify heterogenous TERT expression in different cell types [13]. All examined lymph nodes from our cohort of papillary thyroid “microcarcinomas” were negative for TERT using RNAscope®. This goes into a similar direction as the study by Lee et al. who examined TERT promotor mutation status in combination with BRAF V600E mutations in a cohort of 504 consecutive patients with sub-centimetric papillary thyroid carcinomas measuring. They found a co-occurrence of TERT and BRAF alterations in 16 (3.2%) patients but no association with lymph node metastasis [30]. Another study looking at 16 patients with small papillary carcinomas and their lymph node metastases found BRAF V600E mutation in 75% of tumors, but a low mutational burden in both lymph node metastases and primary tumors. No* TP53* mutations were observed in this study; TERT promotor mutations were not examined [31]. Also, we did not observe an abnormal p53 expression by immunohistochemistry as a surrogate parameter for an underlying TP53 mutation. Perera et al. also identified TP53 mutations in only 1% of their cohort of small papillary thyroid carcinomas with neck lymph node metastases and mutations were restricted to pN1b tumors [32].
In summary, we have examined 22 papillary thyroid carcinomas, measuring ≤ 1 cm with simultaneous lymph node metastasis, in regard to their TERT mRNA expression status, BRAF V600E and p53 status. We did not observe any expression of TERT mRNA in the lymph node metastasis, as well as no abnormal p53 expression, both in primary tumors, as well as the accompanying lymph node metastases. With respect to morphology, 16 lesions showed a classic pattern, while 6 belong to the follicular subtype. Stromal dysplasia, encapsulation and lymphoid infiltrate varied across primary tumors.
Conclusion
Taken together, our data indicate that TERT expression level alterations are not involved in the development of early lymph node metastasis in patients with sub-centimetric papillary thyroid carcinomas.
As our sample size is relatively small and TERT promotor mutations were not evaluated in this study, subsequent prospective studies confirming our findings are needed and are in preparation. In particular, studies are warranted exploring novel molecular marker and or morphological factors for the prediction of early lymph node metastasis to better risk stratify patients with small tumors.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kitahara CM Sosa JA Understanding the ever-changing incidence of thyroid cancer Nat Rev Endocrinol 2020161161761810.1038/s 41574-020-00414-932895503 PMC 7476643 · doi ↗ · pubmed ↗
- 2Mao J Risk Factors for Lymph Node Metastasis in Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis Front Endocrinol (Lausanne)20201126510.3389/fendo.2020.0026532477264 PMC 7242632 · doi ↗ · pubmed ↗
- 3Coca-Pelaz A Papillary Thyroid Cancer-Aggressive Variants and Impact on Management: A Narrative Review Adv Ther 20203773112312810.1007/s 12325-020-01391-132488657 PMC 7467416 · doi ↗ · pubmed ↗
- 4Song YS Park YJ Genomic Characterization of Differentiated Thyroid Carcinoma Endocrinol Metab (Seoul)201934111010.3803/En M.2019.34.1.130912334 PMC 6435845 · doi ↗ · pubmed ↗
- 5Landa I Genomic and transcriptomic hallmarks of poorly differentiated and anaplastic thyroid cancers J Clin Invest 201612631052106610.1172/JCI 8527126878173 PMC 4767360 · doi ↗ · pubmed ↗
- 6Kim TH The association of the BRAF(V 600E) mutation with prognostic factors and poor clinical outcome in papillary thyroid cancer: a meta-analysis Cancer 201211871764177310.1002/cncr.2650021882184 · doi ↗ · pubmed ↗
- 7Liu C Chen T Liu Z Associations between BRAF(V 600E) and prognostic factors and poor outcomes in papillary thyroid carcinoma: a meta-analysis World J Surg Oncol 201614124110.1186/s 12957-016-0979-127600854 PMC 5012084 · doi ↗ · pubmed ↗
- 8Tavares CENDOCRINE TUMOURS: Genetic predictors of thyroid cancer outcome Eur J Endocrinol 20161744 R 117R 12610.1530/EJE-15-060526510840 · doi ↗ · pubmed ↗