Four-dimensional flow assessment shows coronary artery flow reversal in severe aortic regurgitation
Mahesh Chandra Garg, Pankaj Garg

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
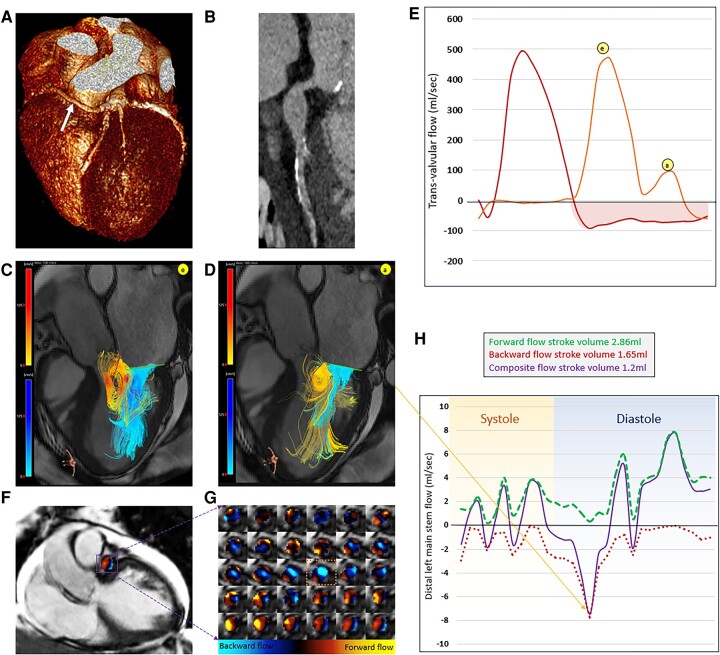 Figure 1
Figure 1- —Wellcome Trust10.13039/100010269
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Aortic Disease and Treatment Approaches · Cardiac Imaging and Diagnostics
Case description
A 65-year-old man with a history of chest discomfort on exertion, breathlessness, and moderate aortic regurgitation (AR) was referred for cardiovascular magnetic resonance (CMR). A previous cardiac computed tomography showed that the left main stem (LMS) was aneurysmal (21 × 21 × 28 mm), and he had an anomalous coronary artery (right coronary origin from the LMS: benign course) (Figure 1A). Cardiovascular magnetic resonance examination was performed on a 1.5T Siemens Sola scanner (see Supplementary data). The CMR protocol included standard cines, T1 mapping, late gadolinium enhancement, and four-dimensional flow imaging (4D flow). For 4D flow, we used high spatial resolution (1.6 × 1.6 × 1.6 mm). The left ventricle (LV) was significantly dilated in end-diastole (134 mL/m^2^) and end-systole (78 mL/m^2^) with an LV ejection fraction of 44% (Figure 1B). The extracellular volume (ECV) was elevated at 34%.
Four-dimensional flow imaging (4D flow) cardiovascular magnetic resonance imaging of aortic regurgitation and coronary artery. (A) Three-dimensional reconstruction of the heart and coronary arteries using cardiac computed tomography demonstrating that the right coronary artery originates from the left main stem (LMS) (white arrow). (B) Multi-planar reconstruction of the LMS and proximal left anterior descending artery demonstrating LMS dilatation. (C) Three-dimensional blood flow streamlines demonstrating competing aortic regurgitation (red-yellow scale) vs. mitral inflow blood flow (blue scale) during early filling. (D) Three-dimensional blood flow streamlines demonstrating competing aortic regurgitation (yellow) vs. mitral inflow blood flow (blue) during late filling. The aortic regurgitation interferes with the opening of the anterior mitral valve leaflet and restricts the filling. (E) Transvalvular flow curves (mitral, orange flow curve; aortic, red flow curve) computed using valve tracking procedures demonstrate significant holo-diastolic aortic regurgitation. (F) A coronal view cine where dilated left main step was identified and corresponding 4D flow data were then superimposed. (G) The LMS flow for the complete cardiac cycle (beginning with systole similar to flow curves in panel E) demonstrates backward flow during diastole as blue. (H) Coronary flow quantification flow curves demonstrate bi-phasic flow reversal during diastole—which is abnormal and mainly due to negative pressure in the aortic sinus, resulting from aortic regurgitation.
On 4D flow streamline visualization, we observed that the AR was eccentric and thrashing towards the anterior mitral valve leaflet (Figure 1C–E), interfering with late LV filling. Aortic regurgitation quantified by valve tracking methods^1^ was severe, with a regurgitation fraction of 39%.^2^ A distal cross-sectional plane was used to quantify coronary flow (Figure 1F–H). We observed significant flow reversal during diastole. This flow reversal was bi-phasic. Normal coronary flow is ∼250 mL/min. In this gentleman’s case, it was significantly reduced to 60 mL/min, a total reduction of 74%.
In this case, cutting-edge 4D flow CMR imaging was used to unravel coronary flow physiology in a patient with severe AR, and this possibly explains the typical exertional symptoms of chest pain. This pathophysiological process has only been speculated previously in the literature.^3^ Future prospective studies are needed to establish the clinical prognostic role of myocardial ischaemia in the context of AR, where there is no significant coronary artery disease. Importantly, advancements in high-resolution 4D flow CMR imaging will likely broaden its clinical application—especially in coronary arteries.
Supplementary Material
ytae059_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Juffermans JF, Minderhoud SCS, Wittgren J, Kilburg A, Ese A, Fidock B, et al Multicenter consistency assessment of valvular flow quantification with automated valve tracking in 4D flow CMR. JACC Cardiovasc Imaging 2021;14:1354–1366.33582060 10.1016/j.jcmg.2020.12.014 · doi ↗ · pubmed ↗
- 2Vejpongsa P, Xu J, Quinones MA, Shah DJ, Zoghbi WA. Differences in cardiac remodeling in left-sided valvular regurgitation: implications for optimal definition of significant aortic regurgitation. JACC Cardiovasc Imaging 2022;15:1730–1741.35842362 10.1016/j.jcmg.2022.05.006 · doi ↗ · pubmed ↗
- 3George BA, Roberts BJ, Grayburn PA. Diastolic left main coronary flow reversal as a marker of severe aortic regurgitation. Tex Heart Inst J 2012;39:764–765.23109790 PMC 3461678 · pubmed ↗