Prevalence and Epidemiological Characteristics of Anogenital Warts Among Recently Diagnosed HIV-Positive Women on Antiretroviral Therapy in Lagos, Nigeria
Ayodeji K Adefemi, Adeyemi A Okunowo, Rose I Anorlu

TL;DR
This study found that 8.5% of recently diagnosed HIV-positive women in Lagos, Nigeria, had anogenital warts, with factors like low education and high viral load being linked to the condition.
Contribution
The study provides new epidemiological data on anogenital warts in recently diagnosed HIV-positive women in Lagos, Nigeria.
Findings
The prevalence of anogenital warts among recently diagnosed HIV-positive women was 8.5%.
Significant associations were found between anogenital warts and low CD4 count, high viral load, and use of oral contraceptive pills.
Most affected women were single, unemployed, and had no tertiary education.
Abstract
Background Anogenital warts (AGWs) are a prevalent condition resulting from human papillomavirus (HPV) infection, which is the most frequently encountered sexually transmitted infection (STI) on a global scale. Women who are HIV-positive experience a disproportionately high burden of AGWs compared to other populations. It is imperative to comprehend the epidemiological factors linked to the disease within this particular at-risk population. Objectives The objective of the study was to ascertain the prevalence of AGWs and its demographic and socio-biological epidemiological features among recently diagnosed HIV-positive women (HPW) in Lagos, Nigeria. Materials and methods The research was a descriptive cross-sectional study conducted among a sample of 420 recently diagnosed HPW. The study was conducted at the HIV clinic of a tertiary health institution located in Lagos, Nigeria. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
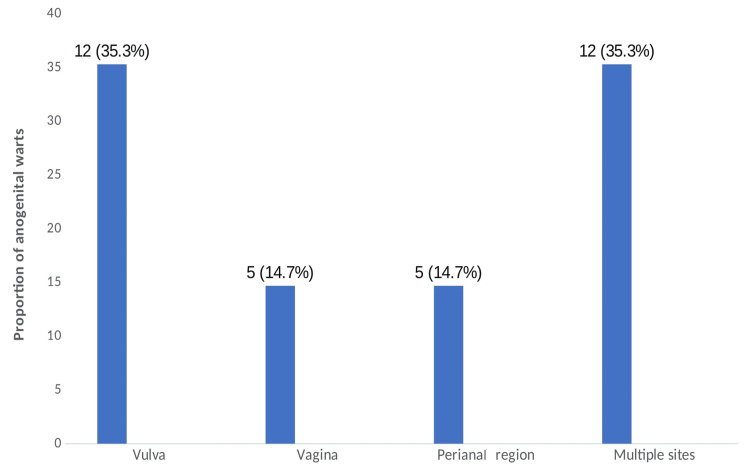 Figure 1
Figure 1| Demographic characteristics | Frequency N=402 | Percentage (%) |
| Age groups (in years) | ||
| <20 | 23 | 5.7 |
| 20–29 | 162 | 40.3 |
| 30–39 | 174 | 43.3 |
| ≥40 | 43 | 10.7 |
| Mean age±SD | 30.7±7.6 | |
| Occupation | ||
| Unemployed | 53 | 13.2 |
| Unskilled labor | 180 | 44.8 |
| Skilled labor | 142 | 35.3 |
| Professionals | 27 | 6.7 |
| Marital status | ||
| Single | 115 | 28.6 |
| Married | 258 | 64.2 |
| Divorced | 21 | 5.2 |
| Widowed | 8 | 2.0 |
| Religion | ||
| Christianity | 373 | 92.8 |
| Islam | 27 | 6.7 |
| Traditional religion | 2 | 0.5 |
| Educational status | ||
| No formal education | 62 | 15.4 |
| Primary education | 111 | 27.6 |
| Secondary education | 185 | 46.0 |
| Tertiary education | 44 | 10.9 |
| Variables | Frequency N=402 | Percentage (%) |
| Parity | ||
| 0 | 63 | 15.7 |
| 1 | 68 | 16.9 |
| ≥2 | 271 | 67.4 |
| Median (IQR) | 4 (2-5) | |
| Number of lifetime sexual partners | ||
| 1-5 | 23 | 5.7 |
| 6-10 | 367 | 91.3 |
| >10 | 12 | 3.0 |
| Median (IQR) | 8 (7-9) | |
| History of multiple sexual partners in spouse | ||
| Yes | 389 | 96.8 |
| No | 13 | 3.2 |
| Use of condom | ||
| Always | 87 | 21.6 |
| Occasionally | 209 | 52.0 |
| Never | 106 | 26.4 |
| Ever used OCP | ||
| Yes | 50 | 12.4 |
| No | 352 | 87.6 |
| History of alcohol consumption | ||
| Regularly | 107 | 26.6 |
| Occasionally | 227 | 56.5 |
| Never | 68 | 16.9 |
| History of smoking | ||
| Yes | 23 | 5.7 |
| No | 379 | 94.3 |
| CD4 counts (cells/mm3) | ||
| <200 | 40 | 10.0 |
| 200–500 | 199 | 49.5 |
| >500 | 163 | 40.5 |
| Median (IQR) | 440 (291-593) | |
| Viral load (copies/ml) | ||
| <1,000 | 120 | 29.9 |
| 1,000 – 10,000 | 210 | 52.2 |
| >10,000 | 72 | 17.9 |
| Median (IQR) | 4510 (838 – 8,780) |
| Variables | AGWs | p-value | ||
| Present, n=34 (%) | Absent, n=368 (%) | Total, N=402 (%) | ||
| Age groups (in years) | 0.312* | |||
| <20 | 4 (11.8) | 19 (5.2) | 23 (5.7) | |
| 20–29 | 15 (44.1) | 147 (39.9) | 162 (40.3) | |
| 30–39 | 11 (32.4) | 163 (44.3) | 174 (43.3) | |
| ≥40 | 4 (11.8) | 39 (10.6) | 43 (10.7) | |
| Occupation | 0.005* | |||
| Unemployed | 11 (32.4) | 42 (11.4) | 53 (13.2) | |
| Unskilled labor | 10 (29.4) | 170 (46.2) | 180 (44.8) | |
| Skilled labor | 10 (29.4) | 132 (35.9) | 142 (35.3) | |
| Professionals | 3 (8.8) | 24 (6.5) | 27 (6.7) | |
| Marital status | <0.001* | |||
| Single | 16 (47.1) | 99 (26.9) | 115 (28.6) | |
| Married | 12 (35.3) | 246 (66.8) | 258 (64.2) | |
| Divorced | 3 (8.8) | 18 (4.9) | 21 (5.2) | |
| Widowed | 3 (8.8) | 5 (1.4) | 8 (2.0) | |
| Educational status | ||||
| No formal education | 11 (32.4) | 51 (13.9) | 62 (15.4) | 0.028* |
| Primary education | 6 (17.6) | 105 (28.5) | 111 (27.6) | |
| Secondary education | 15 (44.1) | 170 (46.2) | 185 (46.1) | |
| Tertiary education | 2 (5.9) | 42 (11.4) | 44 (10.9) | |
| Socio-biological variables | AGWs | p-value | ||
| Present, n=34 (%) | Absent, n=368 (%) | Total, N=402 (%) | ||
| Parity | 0.060# | |||
| 0 | 10 (29.4) | 53 (14.4) | 63 (15.7) | |
| 1 | 6 (17.6) | 62 (16.8) | 68 (16.9) | |
| ≥2 | 18 (52.9) | 253 (68.8) | 271 (67.4) | |
| Number of lifetime sexual partners | 0.060* | |||
| 1–5 | 1 (2.9) | 22 (6.0) | 23 (5.7) | |
| 6–10 | 31 (91.2) | 336 (91.3) | 367 (91.3) | |
| >10 | 2 (5.9) | 10 (2.7) | 12 (3.0) | |
| Usage of condom | 0.161* | |||
| Always | 3 (8.8) | 84 (22.8) | 87 (21.6) | |
| Occasionally | 20 (58.8) | 189 (51.4) | 209 (52.0) | |
| Never | 11 (32.4) | 95 (25.8) | 106 (26.4) | |
| Usage of OCP | <0.001# | |||
| Yes | 12 (35.3) | 38 (10.3) | 50 (12.4) | |
| No | 22 (64.7) | 330 (89.7) | 352 (87.6) | |
| Alcohol intake | 0.421* | |||
| Regular intake | 10 (29.4) | 97 (26.4) | 107 (26.6) | |
| Occasional intake | 21 (61.8) | 206 (55.9) | 227 (56.5) | |
| Never | 3 (8.8) | 65 (17.7) | 68 (16.9) | |
| Smoking | <0.001* | |||
| Yes | 20 (58.8) | 3 (0.8) | 23 (5.7) | |
| No | 14 (41.2) | 365 (99.2) | 379 (94.3) | |
| CD4 (cell/mm3) | <0.001* | |||
| <200 | 31 (91.2) | 9 (2.5) | 40 (10.0) | |
| 200–500 | 2 (5.9) | 197 (53.5) | 199 (49.5) | |
| >500 | 1 (2.9) | 162 (44.0) | 163 (40.5) | |
| Median (IQR) | 101 (55-164) | 470 (325-934) | ||
| Viral load (copies/ml) | <0.001* | |||
| <1,000 | 0 (0.0) | 120 (32.6) | 120 (29.9) | |
| 1,000–10,000 | 10 (29.4) | 200 (54.3) | 210 (52.2) | |
| >10,000 | 24 (70.6) | 48 (13.1) | 72 (17.9) | |
| Median (IQR) | 67,000 (8,650-132,714) | 3,880 (764-8,020) | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Genital Health and Disease · Urological Disorders and Treatments
Introduction
Anogenital warts (AGWs) are a result of infection with human papillomavirus (HPV), which is the most prevalent sexually transmitted infection globally [1]. A significant number of sexually active individuals, both male and female, are likely to get the HPV infection at some point in their lives. Nevertheless, this condition typically resolves on its own, and the virus is naturally eliminated by the immune-competent human system [2,3]. In cases where the human immune system is compromised or defective, such as in individuals who are HIV positive, the virus can persist within the body and lead to a range of diseases associated with HPV [1,3,4].
AGW is a sexually transmitted disease primarily caused by low-risk HPV (LrHPV) types 6 and 11, which account for over 90% of cases [1,5,6]. HPV is epitheliotrophic in nature, and it specifically targets and infects the epithelial surfaces, leading to the development of aberrant growth. This growth might manifest as cutaneous, affecting the skin surfaces, or non-cutaneous, affecting the mucosa surfaces [5]. AGWs frequently manifest in the vulvar, vaginal, cervical, perineum, and perianal areas in females [7,8]. In males, it can manifest in various areas, including the penile shaft, glans, external urethral meatus, scrotum, urethra, perineum, and anal regions [7]. AGWs can manifest as discrete or confluent features, displaying variable sizes. These lesions typically appear as reddish, pinkish, or brownish hyperpigmented areas, which may have a fleshy, papular, keratotic, or cauliflower-like texture [7-10].
The majority of AGWs are typically asymptomatic and are commonly detected incidentally, either by the patient or by the attending physician during clinical examination [9]. Nevertheless, it may be linked to various issues, including physical, emotional, psychological, and economic challenges. Typical physical symptoms commonly associated with AGW include pruritus, discomfort, vaginal discharge, bleeding, burning sensations, and dyspareunia [7-9]. Emotional and psychological challenges related to AGW encompass various psychosocial and psychosexual issues. Psychosocial problems may manifest as feelings of shame, embarrassment, guilt, and depression. On the other hand, psychosexual problems may involve a decrease in sexual drive due to the fear of one's partner discovering their AGW condition, experiencing embarrassment after disclosure, and concerns about transmitting AGW to sexual partners [6,8]. Additionally, it is important to note that this condition carries a substantial economic burden, particularly among individuals in the young reproductive-aged demographic who may lack the financial means to cover the extensive costs associated with both direct and indirect treatment expenses [6,9].
The correlation between HIV and HPV remains incompletely elucidated; nonetheless, it is postulated that HIV may exhibit a symbiotic association with HPV infection. Research has demonstrated that the presence of HPV infection significantly elevates the likelihood of acquiring HIV infection. Conversely, the presence of HIV infection intensifies the persistence of HPV infection and its progression to disease [11-14]. The interaction between these factors contributes to the increased prevalence of HPV infection and the significant burden of HPV-related diseases observed in people living with HIV and AIDS (PLWHA) [15]. It is thus unsurprising that AGW, the most prevalent disease caused by HPV, exhibits a higher prevalence and severity among PLWHA in comparison with individuals without HIV/AIDS [13].
The sub-Saharan Africa region exhibits a notable prevalence of HPV and HIV infections, which plays a significant role in the heightened burden of AGW and its unfavorable outcomes in the region [13,14,16]. Furthermore, several factors have been identified as potential influencers of the burden of AGW among PLWHA. These factors include the utilization and adherence to antiretroviral therapy (ART), the duration of ART treatment, the level of HIV-related immunosuppression, the CD4+ cell count, and the HIV viral load [13,17]. Nevertheless, the epidemiological implications of certain factors remain uncertain, particularly within our specific context. Our study aimed to assess the prevalence of AGW and its demographic and socio-biological epidemiological features among recently diagnosed HIV-positive women (HPW) in Lagos, Nigeria.
Materials and methods
Study design and setting
The research was a comparative cross-sectional study carried out among recently diagnosed HPW who attended the AIDS Prevention Initiative in Nigeria (APIN) clinic at Lagos University Teaching Hospital, Lagos, Nigeria, between March 2016 and September 2016. The APIN clinic provides healthcare services to a patient population of over 10,000 PLWHA, with females comprising more than 60% of the total. The clinic operates a general outpatient clinic daily, while specialized clinics are scheduled on specific days. HPW were provided with counseling on cervical cancer screening and were referred to the cytology and colposcopy clinic for screening. Individuals experiencing gynecological issues received counseling and treatment and were referred to the gynecological outpatient clinic for further assessment and treatment.
Study population and eligibility criteria
The study population consisted of recently diagnosed HPW who sought treatment at the APIN clinic within the institution. In the context of this study, a recently diagnosed individual with HIV/AIDS refers to someone who has received a diagnosis of HIV/AIDS within the past six months and has recently initiated ART. Patients with clinical evidence of AGWs on pelvic examination were classified as the study group, while those without clinical evidence of AGWs were classified as the comparison group.
The study included recently diagnosed HPW, aged 18 years and older, who were sexually active, and had attended the APIN clinic. Only those who provided informed consent were included in the study. In contrast, individuals who were under the age of 18, not sexually active, or unwilling to participate in the study were excluded from the research.
Sample size determination and recruitment of study participants
The sample size was determined using the formula (n=Z^2^p (1−p)/d^2^) [18], with an absolute error margin of 5% (d=0.05), type 1 error of 5% (Z=1.96), and a prevalence of AGW (p) of 9.3% [19]. The minimum sample size was determined to be 124, taking into account a non-response rate of 15%. HPW who met the eligibility criteria were provided with information about the study's purpose and subsequently recruited using a convenient sampling method following the acquisition of informed consent.
Instrument of survey and data collection
The survey instrument utilized in this study was a pretested structured data form designed to collect pertinent demographic and socio-biological information from the participants. The demographic information collected included the participants' age, religion, occupation, educational status, and marital status. The socio-biological data collected included information on the type of marriage, usage and duration of OCPs, condom usage, smoking history, and alcohol consumption. Additional socio-biological data collected included the number of childbirths, total count of lifetime sexual partners, history of multiple sexual partners in the spouse, and details regarding the viral load and CD4 count levels.
The questionnaires were administered by trained research assistants to all eligible study participants in an interviewer-administered format following the acquisition of informed consent. Before the study began, a pretest of the questionnaire was conducted among a convenient sample of 20 recently diagnosed HPW who were attending the HIV clinic at another hospital. The purpose of this pretest was to evaluate the clarity of the questionnaire's instructions, the ease of comprehension, the appropriateness of its content, and to identify any potential ambiguity within the questionnaire. The findings from the pilot study were used to make appropriate enhancements to the study questionnaire.
Clinical examination
All participants underwent a comprehensive examination of their external genitalia conducted by the attending gynecologist. The clinical examination took place in a designated consultation room with a female chaperone following the acquisition of informed consent. The participants were positioned supine on the examination couch, with the vulva appropriately exposed. A comprehensive examination of the entire vulva, perineum, and anal regions was performed under proper illumination to assess for the presence of warts. A speculum of suitable size was inserted to expose the vaginal walls and cervix adequately. Subsequently, a thorough examination was conducted to determine the presence of any warts. HPW with identifiable AGW were counseled and administered suitable treatment.
Data analysis
The data were entered into the computer, cleaned, and validated. Data analysis was done using IBM SPSS Statistics for Windows, Version 23.0 (Released 2015; IBM Corp., Armonk, New York, USA). Descriptive statistics were presented as frequencies and percentages in tables or figures. Continuous data were assessed for normality using Shapiro-Wilk test. Normally distributed variables were presented as mean±standard deviation (SD), while skewed variables were expressed as median and interquartile range (IQR). Data were grouped into categories for ease of analysis, and bivariate analysis was done using Pearson’s chi-square test (or Fisher’s exact test) and Student’s t-test (or Mann-Whitney U test) to compare categorical and continuous variables, respectively. Statistical significance was set at a p-value <0.05 and a 95% confidence interval.
Ethical consideration
Ethical approval (ADM/DCST/HREC/APP/394) was obtained from the Human Research and Ethical Committee of Lagos University Teaching Hospital before conducting the study. Informed consent was obtained from all participants before their enrollment in the study. The study was carried out in accordance with the Declaration of Helsinki (1964).
Results
Out of a total of 420 participants that were enrolled in the study, 402 (95.7%) had complete data and were included in the final analysis.
Demographic characteristics of study participants
Table 1 presents the characteristics of the study participants. The mean age of the participants was 30.7±7.6 years, with the majority (43.3%, 174/402) between the ages of 30 and 39 years followed by 20 and 29 years (40.3%, 162/402). A greater proportion of the participants were married (64.2%, 258/402), Christians (92.8%, 373/402), had a secondary level of education (46.0%, 185/402), and had an unskilled occupation (44.8%, 180/402).
Socio-biological characteristics of study participants
The median parity of the participants was 4 (2-5), with the majority having a parity of 2 and above (67.4%, 271/402). All the participants were sexually active, with the majority having between six and 10 lifetime sexual partners (91.3%, 367/402) and a median total lifetime sexual partner of 8 (7-9). Most of the women (96.8%, 389/402) had sexual partners who had other sexual partners and used condom for contraception (87.6%, 352/402). The median CD4 count was 440 (291-593) cells/mm^3^, with the majority having a CD4 count between 200 and 500 cells/mm^3^ (49.5%, 199/402), while the median viral load was 4,510 (838-8,780) copies/ml, with approximately half of the participants having a viral load of 1,000-10,000 copies/ml (52.2%, 210/402) (Table 2).
Prevalence and distribution of AGWs
The prevalence of AGWs among recently diagnosed HPW was 8.5% (34/402). The majority of the warts were located on the labia (35.3%, 12/34), followed by the vagina (14.7%, 5/34) and perianal region (14.7%, 5/34), while 35.3% (12/34) were located on more than one region, commonly the labia and perianal regions (Figure 1).
Site distribution of AGWs among recently diagnosed HPW on antiretroviral drugs (n=34).AGWs: anogenital warts; HPW: HIV-positive women.The data have been represented as frequency (n) and percentage (%).
Demographic and socio-biological factors associated with AGWs among HPW
It was observed that occupation (p=0.005), marital status (p<0.001), and educational status (p=0.028) were the only demographic factors that were significantly associated with the occurrence of AGWs among HPW. The majority of the HPW who had AGWs were unemployed (32.4%, 11/34), single (47.1%, 16/34), and did not have tertiary education (94.1%, 32/34). More than two-thirds of the AGWs occurred in women between the ages of 20 and 39 years, with women <20 years and ≥40 years having the lowest prevalence of AGWs. However, age was not significantly associated with the presence of AGWs (p=0.312) (Table 3).
*Table 3: Demographic factors associated with AGWs among study participants.AGWs: anogenital warts.p-value <0.05 is considered significant. The data have been represented as frequency (n) and percentage (%).Fisher's exact test.
Some socio-biological factors were found to be associated with the occurrence of AGW. The use of OCP and smoking were significantly associated with HPW having AGW (p<0.001, respectively). Similarly, lower levels of CD4 count and higher levels of viral load were significantly associated with the occurrence of AGW among HPW (p<0.001, respectively). On the other hand, parity, total number of lifetime sexual partners, use of condoms, and alcohol intake were not significantly associated with having AGW (p>0.05) (Table 4).
*Table 4: Socio-biological factors associated with AGWs among study participants.AGWs: anogenital warts; OCP: oral contraceptive pill; IQR: interquartile range.p-value <0.05 is considered significant. The data have been represented as frequency (n), percentage (%), and median (IQR).Fisher's exact test.#Pearson's chi-square test.
Discussion
This study aimed to investigate the prevalence, pattern, and epidemiological factors related to clinically diagnosed AGWs among recently diagnosed HPW who were receiving ART. The prevalence of AGWs was found to be 8.5% (34/402), with the majority of lesions observed on the labia. Occupation, marital status, and educational status were the significant demographic factors associated with AGWs among HPW. Additionally, sociobiological factors such as the use of OCPs, smoking habits, CD4 count, and viral load were significantly associated with AGW.
HIV infection is commonly recognized as a substantial risk factor for the development of AGWs, with a higher prevalence and incidence observed among individuals living with HIV and AIDS compared to those who are not infected [17,20]. This is consistent with the findings in our study where the prevalence of AGWs (8.5%, 34/402) among HPW is higher than that reported among non-HIV-infected women by Dareng et al. (1.0%) [9] in Nigeria and Low et al. (1.6%) [21] in Burkina Faso among non-HIV-infected women. A systematic review and meta-analysis reported that the prevalence of AGW was five times higher in HPW compared to women who are HIV-negative [17]. This finding can be attributed to the increased susceptibility of HPW to multiple HPV infections, and compromised cell-mediated immunity, which hinders the clearance of the HPV infection in this population [9,22].
There is a lack of available data regarding the prevalence and epidemiological characteristics of AGW among HPW in our environment. Our study revealed a higher prevalence of AGW compared to the findings reported by another author in Abuja, Nigeria. In Abuja, the prevalence rate was documented to be 5.0% [9]. These findings align with research conducted in Russia, which indicates that the prevalence of AGW among women varies across different regions of the country, ranging from 4.9% to 8.9% [19]. The prevalence observed in our study was higher than the reported figure in some other African countries like South Africa (5.7%) and Burkina Faso (7.0-7.5%) [13,21]. This is not unexpected, as the prevalence of AGW is influenced by various factors such as geographical location, socio-cultural characteristics, sexual behavior, the prevalence of HIV infection, and immune susceptibility within the studied population [9,21].
The study revealed that demographic factors, including occupation, educational level, and marital status, exhibited a significant association with the presence of AGW in HPW. The prevalence of AGW was notably higher among women who were unemployed and had a lower level of education in the HPW population. Occupation and educational attainment significantly influence the socioeconomic status of individuals. A correlation has been consistently observed between low level of education, occupation, and low socioeconomic status, which has been identified as a risk factor for having AGW [9]. According to the available data, individuals with higher levels of education or occupations in professional fields tend to exhibit a reduced likelihood of experiencing AGW [21]. However, it is essential to note that these findings contradict the results of another study, where education and occupation did not impact the risk of developing AGW [14].
Marital status was associated with AGWs among HPW in our study. HPW who are single were more likely to have AGWs compared to those who were married. This observation aligns with the results reported in certain studies, yet it contradicts the findings reported in another study [9,14]. This phenomenon can likely be attributed to the increased vulnerability of unmarried women to engaging in risky sexual behaviors, such as having multiple sexual partners, engaging with partners who have multiple sexual partners, and having a high number of sexual partners [23-25], which are risk factors for AGW. Although the majority of women in our study who had AGW were under the age of 30, our analysis did not find a significant association between age and the diagnosis of AGW. These findings align with the results observed in certain studies [21,25] and are contrary to others [9,23].
The use of hormonal contraceptives, particularly OCPs, has been found to be linked to the potential risk of developing AGWs [23,26-28]. This is consistent with the findings in our study, where a significant proportion of HPW with AGWs had a history of OCP use compared to those without AGWs. Conversely, OCP was not associated with an increased risk of AGW in some other studies [29]. It is believed that steroids such as estrogen and progesterone can enhance the transcription of HPV and suppress both cellular and non-cellular immune responses to HPV infection [26]. This probably underlines the role of OCP in the persistence of HPV infection.
Similar to findings from our study, smoking has been shown in several studies to be associated with an increased risk of AGW in women and men irrespective of their HIV status [17,21,27,28]. This risk is probably dose-dependent, with heavy smokers having an increased risk compared to non-heavy smokers [1,30]. Immune suppression induced by smoking has been suggested as a possible reason for this association [1,30].
Research has demonstrated that sexual behavior is a significant risk factor linked to the diagnosis of AGWs in both men and women. This suggests that AGW is acquired through sexual transmission [30]. Studies have documented a positive correlation between an increased number of lifetime sexual partners and the risk of developing AGWs [23,27,29,30], but this was not associated with having AGWs in our studies. This is probably due to the generally high rate of sexual activities and a high number of lifetime sexual partners reported among the study participants, irrespective of the diagnosis of AGW.
PLWHA are typically more susceptible to AGWs compared with the non-HIV-positive population due to the higher risk of acquisition and persistence of HPV infection from immunosuppression. Viral load (VL) and CD4 count levels are surrogate markers of the severity of HIV infection and immune suppression among PLWHA. Several studies have shown a significant correlation between the level of VL, CD4 count, and risk of developing AGWs among PLWHA [3,4,9,11,13-15,17,20,21]. High levels of VL and low CD4 count levels are associated with AGWs in this group of people, which is consistent with findings from our study. This buttresses the need for early detection and treatment of HIV infection and the importance of HPV vaccination among this population to prevent HPV-related diseases like AGW.
Limitations
Like in any study, our study has its limitations. The diagnosis of AGWs in this study was made clinically by inspecting the anogenital region. Though histological diagnosis is the most reliable way to diagnose AGW, most AGWs are usually diagnosed clinically. Findings from this study may not reflect the factual findings in the general population of HPW as it is a hospital-based study, and it only focused on a subset of recently diagnosed HPW on ART. Since all the participants were on ART and the duration of the use of ART was relatively short, the study assumed that the use of ART had no impact on the occurrence of AGW.
Conclusions
Based on our findings, we conclude that the prevalence of AGW among recently diagnosed HPW was 8.5% (34/402), with the majority of AGW located on either the labia majora or minora. Demographic factors such as occupation, marital status, and educational status were significantly associated with a diagnosis of AGW, with women who were unemployed, single, and without tertiary education having a higher prevalence of AGW. Similarly, low CD4 count level, high viral load, history of the use of OCP, and smoking were socio-biological factors associated with the diagnosis of AGW among HPW. There is a need to further evaluate the impact of these epidemiological factors in more robust studies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Incidence of anogenital warts: epidemiological risk factors and real-life impact of human papillomavirus vaccination Int J STD AIDS Tyros G Mastraftsi S Gregoriou S Nicolaidou E 4133220213316780310.1177/0956462420958577 · doi ↗ · pubmed ↗
- 2Effectiveness of topical and ablative therapies in treatment of anogenital warts: a systematic review and network meta-analysis BMJ Open Barton S Wakefield V O'Mahony C Edwards S 09201910.1136/bmjopen-2018-027765 PMC 683063731676644 · doi ↗ · pubmed ↗
- 3Update on the epidemiological features and clinical implications of human papillomavirus infection (HPV) and human immunodeficiency virus (HIV) coinfection Microorganisms Pérez-González A Cachay E Ocampo A Poveda E 10471020223563048910.3390/microorganisms 10051047 PMC 9147826 · doi ↗ · pubmed ↗
- 4Incidence, persistence, clearance, and correlates of genital human papillomavirus infection and anogenital warts in a cohort of men living with human immunodeficiency virus in South Africa Sex Transm Dis Chikandiwa A Pisa PT Muller EE Tamalet C Mayaud P Chersich MF Delany-Moretlwe S 3473534620193098563610.1097/OLQ.0000000000000979 PMC 6485297 · doi ↗ · pubmed ↗
- 5Ano-genital warts and HIV status- a clinical study J Clin Diagn Res Dhumale SB Sharma S Gulbake A 0411201710.7860/JCDR/2017/24610.9171 PMC 532447328274028 · doi ↗ · pubmed ↗
- 6Position statement for the diagnosis and management of anogenital warts J Eur Acad Dermatol Venereol O'Mahony C Gomberg M Skerlev M 100610193320193096898010.1111/jdv.15570 PMC 6593709 · doi ↗ · pubmed ↗
- 7Systematic review of the incidence and prevalence of genital warts BMC Infect Dis Patel H Wagner M Singhal P Kothari S 391320132334744110.1186/1471-2334-13-39PMC 3618302 · doi ↗ · pubmed ↗
- 8An overview of genital warts Nurs Stand Richards S 465028201410.7748/ns 2014.02.28.24.46.e 834424517695 · doi ↗ · pubmed ↗