Vascular Ensheathment Reflects Characteristic Migratory Behavior of Paragangliomas
Leor Needleman, Floyd Christopher Holsinger, Justin P Annes

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
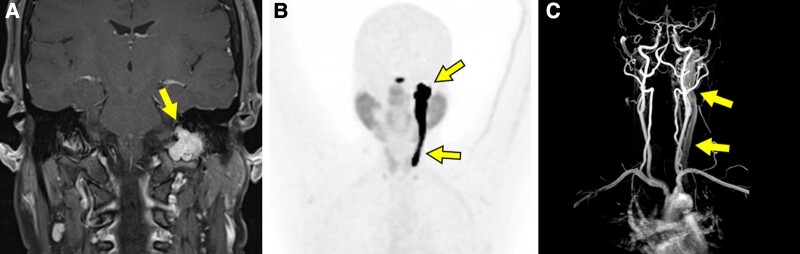 Figure 1
Figure 1- —National Institutes of Health10.13039/100000002
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdrenal and Paraganglionic Tumors · Hormonal Regulation and Hypertension
Image Legend
A 43-year-old female patient presented with recurrent left ear infections and left-sided pulsatile tinnitus. Magnetic resonance imaging (MRI) revealed a left jugular fossa mass eroding the skull base consistent with a glomus jugulare (GJ) tumor (Fig. 1A, arrow). Plasma catecholamine metabolites were normal and genetic testing for hereditary paraganglioma was negative. Functional imaging (^64^Cu-DOTATATE positron emission tomography) to assess the extent of primary disease and evaluate for metastasis showed marked uptake in the left jugular foramen with tumor extension along the internal jugular vein (JV) to the level of the thyroid (Fig. 1B, arrows). The caudal tumor extension was not apparent on the initial skull-base MRI. Magnetic resonance angiography showed splaying of the left internal and external carotid arteries and circumferential involvement of the JV (Fig. 1C, arrows). Head/neck paragangliomas can grow within the JV adventitia. In the Fisch classification system of temporal bone paragangliomas, class C tumors spread inferiorly along the JV and are subclassified according to the extent of carotid artery involvement (1). In a surgical series of 16 paragangliomas with JV invasion, GJ tumors were most frequently represented (69%) (2). Functional imaging may be superior to anatomic imaging for visualizing the migratory behavior of paragangliomas along vasculature.
Magnetic resonance imaging, 64Cu-DOTATATE positron emission tomography and magnetic resonance angiography of the skull base and neck.
The reference list from the paper itself. Each links out to its DOI / PubMed record.